info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: July 15, 2017; Published: July 31, 2017
Corresponding author: Adeniyi Mayowa Jeremiah, Department of Physiology, Faculty of Basic Medical Sciences, College of Health Sciences, University of Ilorin, Ilorin, Nigeria, Pmb 1515 Ilorin, Nigeria
DOI: 10.26717/BJSTR.2017.01.000238
A high fat diet is widely known in scientific consensus to be associated with abnormal lipid and uric acid metabolisms. The dose-related influence of Combined Oral Contraceptive (COC) in both human and animal models on blood lipid parameters is still controversial. Therefore the aim of the study is to investigate the effect of high fat diet (HFD) and two different doses of a COC on plasma lipid profile and uric acid in female wistar rats. Rats were divided into vehicle treated, high dose COC (HCOC, receiving 7.5μg Levonegestrel/1.5μg of estradiol), low dose COC, (LCOC receiving 1.5μg Levonegestrel/0.3μg of estradiol), High Fat (HF receiving 20%w/w of vegetable oil (turkey brand) supplemented feed), HF+HCOC (receiving both 7.5μg Levonegestrel/1.5μg estradiol and HFD) and HF+LCOC (receiving 1.5μg Levonegestrel/0.3μg of estradiol and HFD). Rats were given distilled water, HCOC, LCOC, HFD, HCOC+HF and LCOC+HF for 8 weeks. When compared with vehicle group, HCOC treatment led to a significant increase (P<0.05) in total cholesterol (TC). LCOC treatment also caused a significant rise (P<0.05) in total cholesterol, triglyceride and uric acid. Rats fed HFD showed a significantly higher (P<0.05) total cholesterol and Total/HDL-C ratio. HCOC+HF administration led to a significant elevation (P<0.05) of total cholesterol and Low density lipoprotein (LDL-C). LCOC+HF administration produced a significant increase in total cholesterol, LDL-C, Triglyceride/HDL-C ratio, Total/HDL-C ratio, LDL-C/HDL-C ratio and uric acid. In conclusion, combined oral contraceptive and high fat diet administrations resulted in an elevated total cholesterol and uric acid. The effect on Triglyceride/HDL-C, Total/HDL-C, LDL-C/HDL-C and uric acid was dependent on dose of the contraceptive, the effect on TC and LDL was not dose- dependent. Administrations of low dose of combined oral contraceptive and high fat diet may produce a greater cardiovascular risk than administration of high dose of combined oral contraceptive and high fat diet.
Keywords: Combined Oral Contraceptives; High Fat Diet; Lipid Profile; Uric Acid; Wistar Rats
Abbreviations: HDL: High-Density Lipoprotein; LDL: Low Density; TG: Triglyceride; COC: Combined Oral Contraceptive; HFD: High Fat Diet; TC: Total Cholesterol; LH: Luteinizing Hormone
Nutrition, one of the characteristics of all living organisms is also known as an important player in the aetiology of hyperlipidemia, [1,2], hyperuricemia [3] and atherosclerosis [4]. High-Density Lipoprotein (HDL), Low-Density (LDL) and triglyceride (TG), lipid profile ratios such as Total/HDL, LDL/HDL, TG/HDL and uric acid are associated with cardiovascular diseases [5]. Higher concentrations of LDL, triglyceride, Total/HDL, LDL/HDL, TG/HDL and lower concentrations of functional HDL increase the risk of atherosclerosis. In human, hyperuricemia has been associated with metabolic syndrome components such as obesity, hyperglycemia, hypertension and atherosclerosis. It is associated with dyslipidemia [5].
Different studies in both human and animal models have shown that the type and amount of fat are associated with change in levels, composition and metabolism of serum lipid and uric acid. For example, diets rich in saturated fatty acid have been shown to cause an increase in postprandial lipid level in human in comparison with polyunsaturated n-3 or n-6 fatty acid [6], diets rich in monounsaturated fatty acid has neutral effect on total cholesterol [7]. High fat and ketone infusion in the absence of fasting resulted in a competition between ketones and uric acid for a common tubular secretory site and a decrease in uric acid clearance [3]. Baker et al. [8] reported that serum uric acid was 5.6 and 10.8 times greater in obese and overweight subjects than non-obese subjects.
Fatty acids are naturally occurring acid which are pharmacologically beneficial and even essential to health and in their absence symptoms develop. For instance, Linoleic acid is an essential unsaturated omega-6 necessary for eicosanoid synthesis [9,10]. Linolenic acid is another essential fatty unsaturated acid but of omega-3 type [10]. It reduced cardiac arrhythmias and mortality [11], improved aspects of muscular recovery and increased cell membrane fluidity [12]. Vegetable oils, products from oil bearing seeds are rich sources of saturated and unsaturated fatty acid (including trans- unsaturated fatty acid) and have been used to form high fat diets which have been reported to exert a profound effect on lipid profile. For example, consumption of a high fat diet from corn oil, butter or margarine in mice resulted in an elevated triglyceride whereas supplementation with soybean oil, palm oil, olive oil or sunflower produced a decrease in triglyceride and total cholesterol [13]. Corn oil -rich diet resulted in a significant accumulation of hepatic unesterified fatty acid and decrease Diacyglycerolacyl transferase expression. Increased dietary fat intake raised systolic blood pressure, diastolic blood pressure, compromised endothelial mediated relaxation in hypertensive rats, elicits hypertensive response and induced perivascular fibrosis before development of overt obesity [14].
In Nigeria, turkey palm pure vegetable oil (popularly called turkey oil by Nigerians) is one of the most widely consumed vegetable oil. Although the label on the container indicated it is cholesterol free, chemical analysis using High Performance Chromatography by Okpuzor et al. [15] showed it contained 1.9mg/ ml of cholesterol. Several works have showed that cholesterol is the main cause of atherosclerotic lesions which are the major causes of coronary heart disease [16,17]. Furthermore, as far as amelioration of diet induced hyperlipidemia in animal model is concerned several chemical agents have been shown to produce positive lipid profile. For instance while vitamin A was shown to increase the level of high density lipoprotein [18], NO-188 demonstrated tendency to enlarge HDL particle size [19]. Also, folic acid and estrogen (in the form of 17B estradiol) respectively reduced high fat induced hypercholestolemia in rats due to their antioxidant and anti-atherogenic activity [20]. Although, estrogen is known to induce synthesis of nitric oxide which may reduce the risk of atherosclerosis, it is unclear whether it is responsible for the cardioprotective activity in premenopausal women. Oral contraceptive pills are hormonal agents that provide an effective means of birth control. They are of different types and compositions. One type of oral contraceptive pill is Combined Oral Contraceptive (COC). Combined Oral n increased risk of both arterial and venous thrombosis [21].
However, modern combined oral contraceptive contain progestogen, classed as a second or third generation and which are all derivatives from19-nor testosterone [22] and contains low dose of estrogen between 20–35μg and a progestogen [23]. The dominant component of modern combined oral contraceptive, progestin inhibits ovulation by suppressing the cyclical release of luteinizing hormone (LH) from the anterior pituitary gland. Progestins also create thick cervical mucus that slows sperm transport and inhibits capacitation [22].
Estrogens are known to be powerful antioxidants independently of their binding to the estrogen receptors and the hormonal functions [24]. They also have beneficial effects on blood lipid parameters, these effects include a reduction in LDL, an increase in HDL, but it increases plasma triglyceride levels [25]. On the other hand, Knopp et al. [26] (1994) had found that progestins appear to slow the stimulatory effect of estrogens on lipoprotein transport in the bloodstream [25] and actively prevents pregnancy [27]. Several researchers have reported the advantages [28], complications and side-effects of combined oral contraceptives [29]. The effects of combined oral contraceptives on plasma lipid and lipoproteins have also been studied. An increase in serum triglycerides, which are mainly present in very low density lipoprotein, has been reported [30]. Another study reported that the serum cholesterol level was unchanged in women taking low-dose combined oral contraceptives; however the proportion of serum cholesterol carried by high-density lipoprotein (HDL) was decreased, while that carried by low density lipoprotein (LDL) and VLDL was increased [31]. Olatunji et al. [32] showed that high dose of a combined oral contraceptive decreases HDL-C in female rats, while both high and low doses of the agent increase triglyceride. There is no report on the effect of high fat diet from turkey oil and two different doses of a combined oral contraceptive on lipid profile and uric acid in female rats at the time of this study.
Women are exposed to sex steroids in several formulations such as oral contraceptives and Hormone Replacement Therapy. Turkey vegetable oil is a cheaply available product derived from plants. Apart from the increase in consumption rate of this ingredient during festive season, it has been known not to be cholesterol-free.
The aim of this study is to investigate the effect of high fat diet from turkey oil and two different doses of a combined oral contraceptive on plasma lipid profile and uric acid in female rats
The objectives of the study are to investigate:
i. The effect of high dose of COC on plasma lipid profile and uric acid
ii. The effect of low dose of COC on plasma lipid profile and uric acid.
iii. The effect of high fat diet on plasma lipid profile and uric acid.
iv. The effect of high dose of COC and high fat diet on plasma lipid profile and uric acid.
v. The effect of low dose of COC and high fat diet on plasma lipid profile and uric acid.
48 female Wistar rats weighing between 140 – 160g were obtained from united sacrificial farm, opposite Bechadims hotel, off. Unilorin road, Tanke Oke Odo, Ilorin. The rats were housed in a well-ventilated wooden cage with demarcations in the animal house at University of Ilorin Research Laboratory, Department of Physiology, Faculty of Basic Medical Sciences, and University of Ilorin (Table 1).
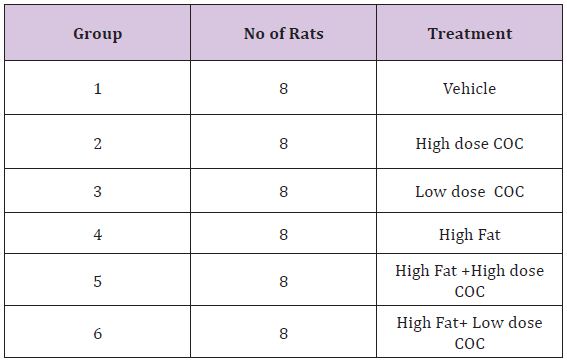
Table 1:Experimental Grouping.
The animals used for this investigation were given pelletized high fat and normal diets obtained from Oluwagbemisola Livestock Feeds, Offa garage, Ilorin. 2kg of turkey vegetable oil was supplemented with 8kg of feed prepared in accordance with the method of Woods et al., (2003)[33] to make 20%w/w of high fat diet (HFD). Standard chow (normal diet) was a turkey vegetable oil deficient feed. Turkey vegetable oil consists of 46% saturated fatty acid, 42% mono-unsaturated fatty acid and 12% of polyunsaturated fatty acid (Table 2).
A tablet of oral contraceptive pill containing 0.15mg Levonegestrel and 0.03mg Ethinylestradiol was dissolved in 5ml of distilled water (High dose) and 25ml of distilled water (Low dose) respectively. 0.3ml was given to each rat (containing 7.5μg Levonegestrel /1.5μg Ethinylestradiol for high dose preparation and 1.5 μg of Levonegestrel / 0.3μg of Ethinylestradiol for low dose preparation).s
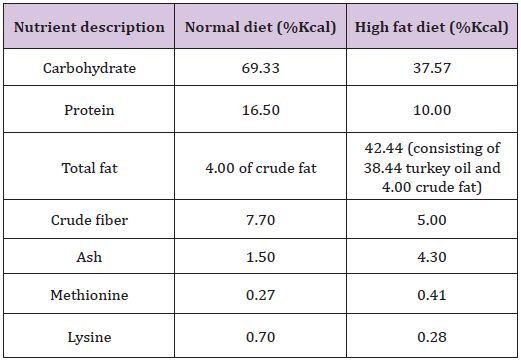
Table 2:The nutritional composition (%Kcal).
a) Group 1: Received distilled water (0.3 ml; p.o.), along with normal feed and was designated as vehicle treated.
b) Group 2: Received distilled water (0.3 ml; p.o.) containing a combination of 7.5μg Levogestrel/1.50μg Ethinylestradiol daily along with normal feed and was designated as High dose Combined Oral Contraceptive (HCOC).
c) Group 3: Received distilled water (0.3 ml; p.o.) containing a combination of 1.5μg Levogestrel /0.30μg Ethinylestradiol daily along with normal feed and was designated as Low dose Combined Oral Contraceptive (LCOC).
d) Group 4: Were fed with a HFD (20%w/w) but not treated with Levonegestrel and ethinyl estradiol drug and was designated as High Fat (HF).
e) Group 5: Received distilled water (0.3 ml; p.o.) containing a combination of 7.5μg Levonegestrel/1.50μg Ethinylestradiol daily along with a HFD (20%w/w).
f) Group 6: Received distilled water (0.3 ml; p.o.) containing a combination of 1.5μg Levonegestrel /0.30μg Ethinylestradiol daily along with a HFD (20%w/w).
Administration of OC was done each day for a period of 8 weeks with the use of oral gavage while the animals were fed with the use of feeding trough for 8 weeks as well. The rats were sacrificed by cervical dislocation, and the blood was collected through cardiac puncture into lithium heparin bottle. The blood samples were centrifuged to obtain the plasma. The plasma was separated into a plain bottle for each sample and was analyzed for plasma total cholesterol, high-density lipoprotein, low density lipoprotein, triglyceride and uric acid.
Enzymatic colorimetric determination of total cholesterol according to the following reactions.
Cholesterol ester + H20 cholesterol esterase Cholesterol +fatty acid
Cholesterol +02 cholesterol esterase 4-cholesten-3-one + H202
2H202+ Phenol+ 4-Aminoantipyrine peroxidase Red quinone +4 H20
i. Cholesterol RI (4x50ml): It consists 50mmol/l of pipes buffer (pH 6.90), 24mmol/l of phenol and 0.5mml/lz of sodium cholate.
ii. Cholesterol R2 (4x50ml): It consists ≥200U/l cholesterol esterase, ≥250U/l of cholesterol oxidase, ≥1000U/l of peroxidase and 0.5mmol/l of 4-aminoantipyrine.
iii. Cholesterol standard (1x4ml): with cholesterol standard concentration -200mg/dl.
Table 3 showing the procedure for total cholesterol
i. They were then mixed and incubated for 5minutes at 370c.
ii. The absorbance of the sample and standard was measured against reagent blank.
Cholesterol concentration (mg/dl) = (Absorbance of sample/ absorbance of standard) x 200.
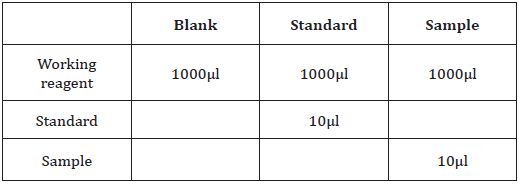
Table 3:The procedure for total cholesterol.
Anti human β-lipoprotein antibody in reagent R1 binds to lipoproteins (LDL, VLDL, and chylomicrons) other than HDL. The antigen-antibody complexes formed block enzyme reactions when reagent R2 is added. Cholesterol esterase and cholesterol oxidase in reagent R2 react only with HDL-C. Hydrogen peroxide produced by the enzyme reactions with HDL-C yields a blue color complex upon oxidative condensation of F-DAOS (N-ethyl-N-(2hydroxy-3- sulfopropyl)-3-5-dimethoxy 4-fluoroaniline, sodium salt) and 4 aminoantipyrine in the presence of peroxidase. By measuring the absorbance of the blue color complex produced, at the optimum wavelength of 593 nm, the HDL-C concentration in the sample be calculated when compared with the absorbance of the HDL- C Calibrator.
a. HDL –C DIRECT R1 2 x 15 ml; It consists 30mmol/L of Good’s buffer (pH 7.0), 0.9 mmol/L of 4-aminoantipyrine, 1U/mL of POD 2.4 and sufficient amount of Anti human β-lipoprotein antibody.
b. HDL –C DIRECT R2 2 x 5 mL; It consists 30 mmol/L of Good’s buffer (pH 7.0), 4 IU/mL CHE, 1U/mL CO 20 and 0.8 mmol/L of F-DAOS.
c. HDL –C DIRECT CALIBRATOR 1 x 3 ml.
Table 4 showing the procedure for lipoprotein
HDL-C (mg/dl) = (Absorbance of sample/absorbance for calibrator) x concentration of the calibrator
LDL-C (mg/dl) = Absorbance for blank/absorbance for calibrator x concentration of the calibrator.
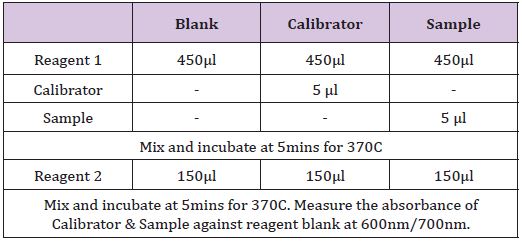
Table 4:The procedure for lipoprotein.
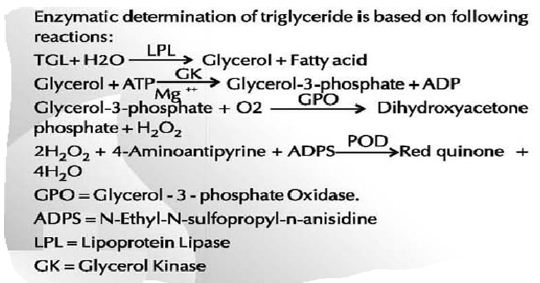
Figure 1:Principle.
Triglyceride R1 (1x53ml/2x53ml): It consists 50mmol/l of Pipes-buffer (pH 7.0), 1mmol/l of ADPS and 15mmol/l of magnesium salt.
i. Triglycerides R2 (5X10ml/5x20ml); It consists 1100U/l of Lipoprotein lipase, 800U/l of Glycerol Kinase, 5000U/l of Glycerol-3-phosphate oxidase, 350U/l of peroxidase and 0.7mmol/l of 4-Aminoantipyrine
ii. Triglyceride standard (1x5ml/1x5ml) with 200mg/dl of Triglyceride standard concentration.
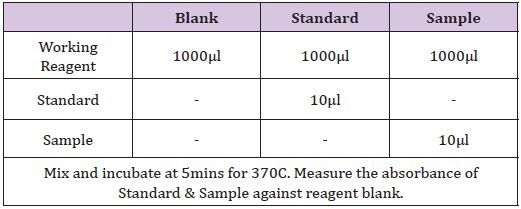
Table 5:The Procedure for triglyceride.
Table 5 showing the Procedure for triglyceride
Triglyceride (mg/dl) = (absorbance of sample/ absorbance of standard) x200.
Total/HDL= Plasma Total cholesterol (mmol/l)/HDL-C (mmol/l)
Triglyceride/HDL-C= Plasma Triglyceride (mmol/l)/HDL-C (mmol/l)
LDL-C/HDL-C=Plasma LDL-C (mmol/l)/HDL-C (mmol/l)
Enzymatic determination of uric acid according to the following reactions.
Uric acid + 2H20+02 uricase Allantoine+CO2 +H202
2H202+4-Aminoantipyrine+DHBS Peroxidase Red quinone+H202+HCl
DHBS-3, 5-Dichloro-2-Hydroxybenzenesulfonic acid.
Uric acid R1: It consists 100mmol/l Phosphate buffer (pH 7.5) and 2mmol/lDHBS.
Uric acid R2: It consists 0.23mmol/l of 4-Aminoantipyrine, 660U/l peroxidase and 60U/l uricase.
Uric acid standard concentration- 6mg/dl.
Table 6 showing the procedure for uric acid estimation
Uric acid concentration (μmol/l) = (Absorbance of sample/ absorbance of standard) x6x59.48.
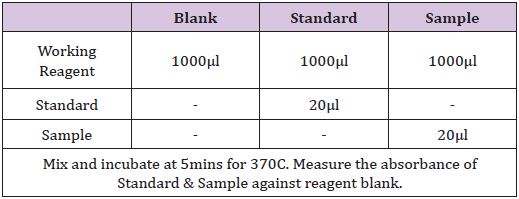
Table 6:The procedure for uric acid estimation.
All data are expressed as means ± standard error of the mean (SEM) for 5 rats per group. Statistical group analysis was performed with SPSS 16.0 statistical software. Statistically significant differences were accepted at p < 0.05 using One –way Analysis of Variance. Least Significance Difference (LSD) test was used to identify the significance of pair wise comparison of mean values among the groups.
There was a significant increase in total cholesterol of HCOC, LCOC, HF, HCOC+HF and LCOC+HF compared with the vehicle (Figure 2).
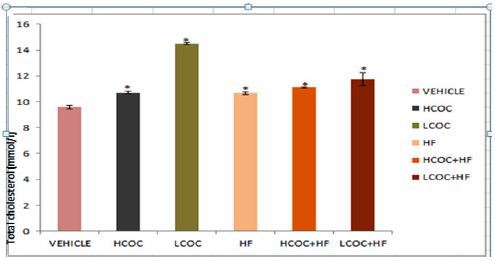
Figure 2:The effect of high fat and COC on total cholesterol. Values are expressed as mean ± S.E.M. of 5 rats per group. *p<0.05 significantly different from vehicle.
There was a significant increase in HDL of HCOC compared to HCOC and HF respectively (Figure 3).
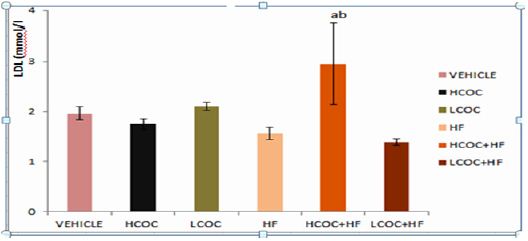
Figure 3:The effect of high fat and COC on HDL. Values are expressed as mean ± S.E.M. of 5 rats per group. ap<0.05 significant difference from HOC. bp<0.05significant difference from HF.
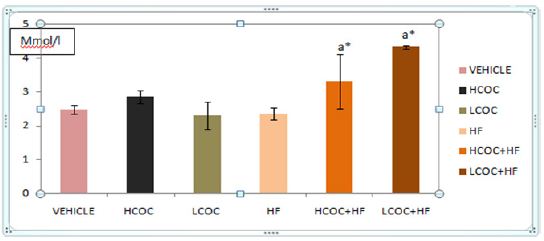
Figure 4:The effect of high fat and COC on LDL. Values are expressed as mean ± S.E.M. of 5 rats per group. *p<0.05 significantly different from vehicle. ap<0.05 significant difference from HF.
There was a significant increase in TG of LCOC compared to vehicle and there was a significant decrease in TG of HCOC compared to LCOC (Figure 5).
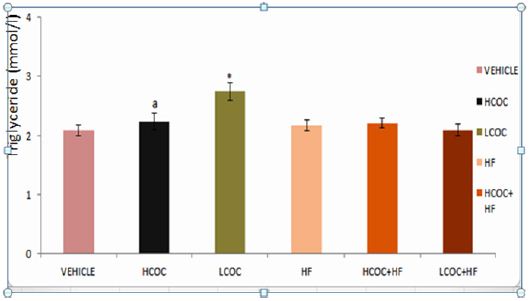
Figure 5:The effect of high fat and COC on triglyceride. Values are expressed as mean ± S.E.M. of 5 rats per group ap<0.05 significant difference from LCOC. *p<0.05 significantly different from vehicle.
There was a significant increase in Total/HDL-C of LCOC, HF and LCOC+HF compared respectively with vehicle. There was also a significant decrease in Total/HDL-C of HCOC+HF compared respectively with LCOC and HF. There was a significant increase in Total/HDL-C of LCOC+HF compared with HCOC (Figure 6).
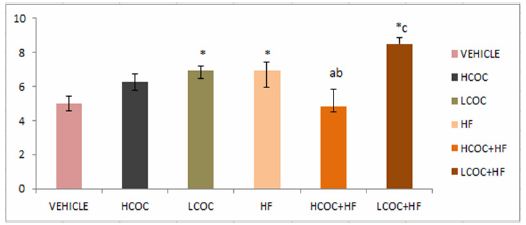
Figure 6:The effect of high fat and COC on Total/HDL-C ratio. Values are expressed as mean ± S.E.M. of 5 rats per group *p<0.05 significantly different from vehicle. ap<0.05 significant difference from LCOC. bp<0.05significant difference from HF. cp<0.05significant difference from HCOC.
There was a significant increase in LDL-C/HDL-C of LCOC+ HF compared with vehicle, HCOC and LCOC respectively. There was a significant decrease in LDL-C/HDL-C of HF compared with LCOC. There was also a significant decrease in LDL-C/HDL-C of LCOC compared with HCOC.
The result showed a significant increase in TG/HDL-C of LCOC+ HF compared with vehicle, There was a significant decrease in TG/HDL-C of HCOC+HF compared respectively with HF and LCOC (Figure 7).
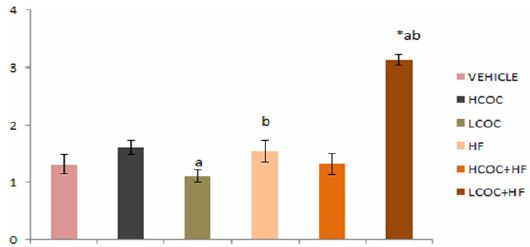
Figure 7:The effect of high fat and COC on LDL-C/ HDL-C ratio. Values are expressed as mean ± S.E.M. of 5 rats per group. ap<0.05 significant difference from HCOC. bp<0.05significant difference from LCOC. *p<0.05 significantly different from vehicle.
There was a significant increase in plasma uric acid of LCOC and LCOC+HF compared respectively with vehicle. There was significant increase of uric acid in LCOC compared respectively with HCOC and HF. There was a significant increase in uric acid of LCOC+HF when respectively compared with LCOC and HF (Figures 8 & 9).
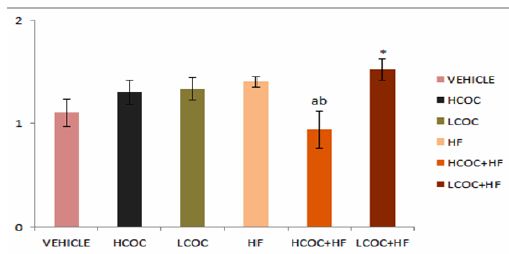
Figure 8:The effect of high fat and COC on Triglyceride/ HDL ratio. Values are expressed as mean ± S.E.M. of 5 rats per group. ap<0.05 significant difference from LCOC. bp<0.05significant difference from HF. *p<0.05 significantly different from vehicle.
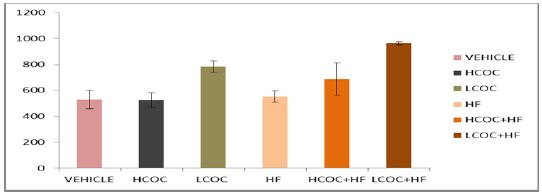
Figure 9:The effect of high fat and COC on plasma uric acid. Values are expressed as mean ± S.E.M. of 5 rats per group. *p<0.05 significantly different from vehicle. ap<0.05 significant difference from HCOC. bp<0.05significant difference from HF.
Decreased high-density lipoprotein cholesterol (HDL-C) and an elevated low-density lipoprotein cholesterol (LDL-C), triglyceride and uric acid are important risk factors for cardiovascular disease [3,34,35]. Reports of different studies on high fat diets had separately documented an elevated total cholesterol, low density lipoprotein (LDL-c), triglyceride (TG) and uric acid and low high density lipoprotein (HDL-c) [3,36]. Oral contraceptives were reported to reduce plasma uric acid while the effect on lipid profile was differing. The present study investigated the effect of high fat diet and two different doses of a combined oral contraceptive on plasma lipid profile and uric acid.
The result showed that high dose of Combined Oral contraceptive (HCOC) treatment led to a significant increase in total cholesterol when compared with vehicle group [37,38]. A number of researchers had showed that estrogen has a beneficial influence on lipid profile. For instance, Akter et al., (2013) [20] claimed that estrogen reduce high fat induced hypercholesterolemia. An increase HDL-c and triglyceride [26] and a decrease in and LDL-C had also been gotten [23,39]. On the other hand, synthetic levonegestrel, progestin and medroxyprogesterone acetate exerted the strongest anti estrogenic effect [40]. Hence, the difference in metabolic effect of combined oral contraceptive use depends on dose and type of progestin component [30]. In this study, the progestogenic agent in micrognon was 5 times the estrogenic agent. Therefore, the increase in total cholesterol may be due to the fact that the progestogenic substance slows down the stimulatory effect of estrogen on lipoprotein transport in the blood stream as reported by Knopp et al.,(1994) [26].
Comparison of HCOC group with LCOC group also showed a significant decrease in triglyceride. In addition, HCOC treatment caused a significant reduction in plasma uric acid when compared with LCOC group but an insignificant decrease in plasma uric acid when compared with the vehicle group. Estrogen is known to increase fractional uric acid excretion and reduce plasma uric acid [41]. Low dose of Combined Oral Contraceptive (LCOC) caused a significant elevation of total cholesterol, triglyceride [32,42] and triglyceride/HDL-C ratio, a predictor of cardiovascular diseases [43] when compared with the vehicle group. However, this result did not contradict the earlier report that low dose oral contraceptive pills are associated with milder side effects but may be due to method adopted in preparing the low dose which resulted in low quantities of levonegestrel/estradiol.
Estrogen is believed to decrease LDL-C [39] and raise HDL-c [26] but at such a low concentration, this effect may be lost. This explanation was also favored by the significant increase in LDL/ HDL ratio of LCOC when compared with HF group which appeared to be due to the fact that LCOC elevated LDL-C more greatly than did by HF. High level of plasma LDL-C is known as a risk factor of cardiovascular disease because oxidized LDL-c becomes attracted by proteoglycan in the arterial wall and brings about initiation and progression of atherosclerosis [43,44]. The significant elevation of plasma uric acid in LCOC when compared with vehicle also concurred with the effect of low dose of estrogen in LCOC group which complied with the dose –dependent influence of estrogen previously reported by Yahyaoui et al., (2008) [41,44].
High fat (HF) administration significantly raised total cholesterol. Although, Okpuzor et al.,(2009) [15] claimed that turkey oil contained cholesterol contrary to the nutritional details conveyed by the label on the container, this study lacked sufficient evidence to justify that Okpuzor’s report was responsible for such an increase since no chemical analysis was done on the oil to ascertain whether it contained cholesterol or not. However, the increase may be attributed to the high level of saturated fatty acid in the diet. Although the manufacturer of the oil again did not indicate the type of saturated fatty acid and whether the mono-unsaturated fatty acid was of cis or trans type, rigorous search of literature showed that vegetable oil derived from palm is richer in palmitic saturated fatty acid than other forms of saturated fatty acid [45] and palmitic acid has been shown to raise the activity level of HMG-coA reductase, an enzyme responsible for endogenous synthesis of cholesterol [46].
TC/HDL ratio which is stronger predictor of coronary artery disease than total cholesterol alone [43] was also significantly raised in HF group when compared with vehicle group. In another development, HF diet reduced plasma uric acid when compared with the LCOC group but exerted an insignificantly increased plasma uric acid when compared with vehicle group. Administration of both High Combined Oral Contraceptive and High Fat diet (HCOC+HF) produced a significant increase on total cholesterol when compared with the vehicle and high fat groups. The change in total cholesterol when compared with vehicle presented in the form of significant increase in low density lipoprotein which has been linked with cardiovascular disease [44]. The elevated low density lipoprotein has been reported to be associated in vasculopathy by impaired vascular production of Nitric Oxide (NO) to form peroxynitrate which in turn plays a role in oxidative vasculopathy [47-49].
Comparisons of HCOC+HF group respectively with HCOC and HF groups showed a significant increase in high density lipoprotein. This implied that administration of both HCOC and HF diet may produce a milder adverse effect than either HCOC or HF. However, the significant increases in HDL and LDL in HCOC+HF group when compared with HF group were not confusing because HCOC+HF tended to increase the mean HDL plasma level slightly more than the mean LDL plasma level. HCOC+HF reduced Triglyceride and Total/ HDL-C when respectively compared with LCOC . It also significantly reduced TG/HDL when respectively compared with high fat as well as when compared with LCOC group. These also buttressed the explanation that HCOC+HF was associated with milder abnormal lipid metabolism than either HCOC or HF alone.
Comparisons of HCOC+HF group respectively with HCOC and HF groups showed a significant increase in high density lipoprotein. This implied that administration of both HCOC and HF diet may produce a milder adverse effect than either HCOC or HF. However, the significant increases in HDL and LDL in HCOC+HF group when compared with HF group were not confusing because HCOC+HF tended to increase the mean HDL plasma level slightly more than the mean LDL plasma level. HCOC+HF reduced Triglyceride and Total/ HDL-C when respectively compared with LCOC . It also significantly reduced TG/HDL when respectively compared with high fat as well as when compared with LCOC group. These also buttressed the explanation that HCOC+HF was associated with milder abnormal lipid metabolism than either HCOC or HF alone. been shown to increase low density lipoprotein [6], the addition of LCOC appeared to cumulatively produce the effect. Further comparisons of LCOC+HF with other groups also showed the unfavorable influence of the combined treatments on lipid profile as well as lipid profile ratios. LCOC+HF significantly increased low density lipoprotein when compared with LCOC and high fat groups respectively. There was a significant increase in triglyceride of LCOC+HF compared with LCOC.
Increase in lipid profile ratios are predictors of coronary heart diseases [50]. For instance, A high level of triglyceride/HDL-c ratio increases atherogenic Index of Plasma (AIP) which reflects the presence of atherogenic small LDL particles [43]. Total/HDL, LDL/HDL and Triglyceride/HDL ratios have also been separately reported as risk factors of cardiovascular events [42-44]. In this study, a significant increase was observed in LDL/HDL, Total/HDL and Triglyceride/HDL of LCOC+HF when compared with vehicle group. LCOC+HF significantly increased Total/HDL and LDL/HDL when compared respectively with HCOC group and LDL/HDL ratio of LCOC+HF group when compared with LCOC.
Moreover, high level of plasma uric acid is known as an independent cardiovascular risk factor, marker of reduced kidney function and a causal risk factor for development and progression of renal disease [51]. In this study there was a significant elevation of plasma uric acid level in LCOC+HF group when compared with vehicle group. Other comparison also showed a significant increase of plasma uric acid level in LCOC+HF when respectively compared with LCOC and HF group. High fat diet is generally known to increase ketone bodies productions which compete favorably with uric acid at the renal filtration membrane because it is a steroid [41]. In this study, LCOC+HF decreased renal excretion of uric acid evidenced by the significant increase in plasma uric acid when compared with either HF or HCOC alone. Although, renal function test was not done in this study, an extensive search of literature showed that elevated uric acid can also be associated with defects of uric acid transport in the nephron [52].
Low dose COC was associated with more abnormal plasma lipid profile and uric acid than high dose COC. The effect of the contraceptive on triglyceride, triglyceride/HDL-C and uric acid was dose dependent while the effect on total cholesterol was not dose dependent. High fat diet from turkey oil was associated with elevated total cholesterol and total/HDL ratio. Administration of Combined oral contraceptive and high fat diet produced an elevated plasma total cholesterol and uric acid. Furthermore, the effect of administration of combined oral contraceptive and high fat diet on triglyceride, triglyceride/HDL, TC/HDL, LDL/HDL and uric acid was dependent on contraceptive dose but the effect on total cholesterol and low density lipoprotein was not dose dependent. In conclusion, administration of both low dose of combined oral contraceptives and high fat diet may produce greater cardiovascular risk than administration of both high dose of combined oral contraceptive and high fat diet.
The study was carried out on lipid profile and uric acid. I recommend that this work should be subjected to further studies to clarify why such low dose should be associated with more abnormal lipid profile result than high dose and understand the mechanisms this may involve. Lastly, it is important that Nigeria ministry of health should ensure that all vegetable oils produced locally or imported to Nigeria conform to international standard and bear on them their correct compositions and sub-components.

























