info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: July 14, 2017; Published: July 31, 2017
Corresponding author: Dr. Amit Gupta, Professor, Department of Surgery, Room No-305, Jai Prakash Narayan Apex Trauma Centre, All India Institute of Medical Sciences, New Delhi, India
DOI: 10.26717/BJSTR.2017.01.0002226
Abbreviation: GCS: Glasgow Coma Scale; ICU: Intensive Care Unit; ISS: Injury Severity Score.
Alcohol consumption arising as leading risk factor for road traffic injuries and one of the major public health concerns globally. Alcoholism is associated with liver disease, coronary vascular disease, Hypertension, Stroke, acute pancreatitis etc. [1-4]. There has been a rapid change in recent years towards alcohol use in India and originated as one of the main contributors to health problems. Recent studies have demonstrated that drink driving is strongly associated with a higher frequency of road traffic accidents which leads to hospitalization to emergency department [5,6].
The alcohol use is increasing in urban areas, therefore, injuries related to alcohol intake and driving is also increased like road traffic accidents, fire and burns, pedestrian falls and drowning as well as intentional injuries such as violence against oneself or others. In developing countries, like India, alcohol related injuries are matter of concern due to the resource constraint setting as burden of injuries have huge impact on the overall economic growth of the country andmajor part of the GDP is lost due to road traffic injuries.
According to World Health Organization (WHO) estimates, there are about 2 billion people worldwide who consume alcoholic beverages. In India estimated 137000 road traffic deaths are reported with annual increase rate of 3%. It has been estimated that one death occurs at every 3 minute, of these 78% are men mostly between the age group of 20-44 year. In resource constrained countries like India it is major economic burden to the country with an estimated loss of 3% annually. The major causes of road traffic injuries are due to increased traffic congestion on roads, poor vehicle and road maintenance, ignorance and lack of safety concerns among people and the presence of unlicensed and unskilled drivers. Another major factor which contributes is that vehicle use is growing rapidly (11%), however, progress in construction of roads is just 4%. An estimated 21% fatalities have been reported among motorized two wheeler users. It has been found that pedestrians and cyclists are the most vulnerable group of road traffic fatalities. It is assumed that alcohol consumption in the country will go up to 10% in the coming decade. The average age of alcohol consumption is now 19 years as compared to 28 years in 90s. This is due to the improved socio-economic status of middle income group alcohol consumer, liberalization from traditional norms in India. The drinking has become status symbol among the youth which is influenced by the glamorization of drinking by celebrities especially by film actors. Promotions of the liquor products due to the major competition in the market also responsible for the increase use of alcohol in the society. The aim of the study was to demonstrate the demographic profile, physiological parameters i.e. GCS, Airway, Region etc., injury severity pattern and mortality of trauma patients following alcohol consumption arriving to the emergency department, Apex Trauma Center in Delhi from September 2013 to November 2013.
The study population consisted of randomly selected breath alcohol positive or negative patients with significant injuries admitted to emergency department of JPNATC, New Delhi for over The study population consisted of randomly selected breath alcohol positive or negative patients with significant injuries admitted to emergency department of JPNATC, New Delhi for over a period of 3 months started from September 2013 to November 2013.A total of 338 randomly selected patients were examined in the emergency department. Of these, 182 were RTI patients with breath alcohol positive (n=89) or negative (n=93). Breathe alcohol analyzer was used for conscious patients and used passive mode for unconscious patients. The clinical assessment was conducted by the duty doctors and documented in the perform available at the department.
The statistical analysis carried out by using SPSS V.23 IBM. The Chi-square test was used to compare categorical variables (Gender, Airway, Region, Admission and Disposition) and Independent- Samples T Test was performed for continues variables (Age, GCS, ISS, Ventilation days, ICU days, Hospital stay) between the two groups. Results were presented in mean + SD, median and number with percentage wherever applicable. The p value less than 0.05 was considered to be statistically significant.
Table 1: Demographic and clinical characteristics of alcohol intoxicated and non-alcoholic patients (n=182).
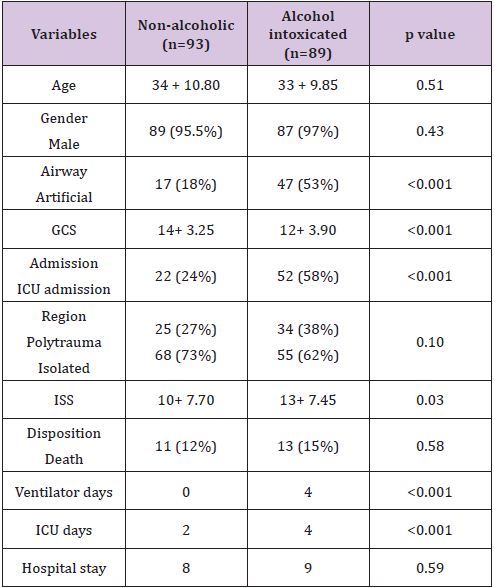
A total 182 RTI patients were selected in the study. Of these, 93 (51%) patients were alcohol negative and 89 (49%) were alcohol positive. All RTI patients recruited in the study were between 30- 40 year age and equally distributed to male and female group. All patients had blunt injury in both the groups. In 89 alcohol positive patients, 47 (53%) had Artificial Airway as compared to 17 (18%), (p<0.001). The GCS score was lower in alcohol positive group (p<0.001). Increased numbers of patients (58%)were admitted to ICU, in alcohol positive group (p<0.001) and had stayed for more days at ICU as compared to alcohol negative group (p<0.001).The patients were on ventilator support for longer time in alcoholic intoxicated patients as compared to non-alcoholic group (p<0.001). These patients had significantly higher ISS score as compared to other group (p<0.03) (Table 1). Note: Age, GCS and ISS presented as mean + SD, Gender, Airway, Admission, Region and Disposition presented as number with percentage and Ventilator days, ICU days and Hospital stay presented as median.
The frequency of drinking and driving is a major risk factor for road traffic crashes universally, however, it varies between countries. It has been shown in studies from low-income countries that between 33% and 69% of fatally injured drivers are alcohol positive. In our study we observed that alcohol consumption significantly affect severity and mortality of the RTI patient. We have observed that patients with positive alcohol levels have lower initial GCS and a higher need for definitive airway, ventilation, ICU stay, higher mean ISS and mortality.
The alcohol intoxication data reporting is extremely missing from the hospitals as there is no strict law in the country for alcohol intake. As per our data it can be concluded that alcohol intoxication can cause significant problems in In-hospital Triage. The important factor in the study is that due to the absence of strict legislation the alcohol consumption amongst the urban middle class is on the rise and 48% of patients are coming to hospitals with injuries are alcohol positive, which shows that increased number of people are still involved in drink driving and alcohol consumption may be the serious risk factor for road traffic injury in urban area like New Delhi.
The GCS is the most commonly used means of quantifying the level of consciousness and for clinical decision making involving patients with traumatic brain injury in emergency departments [7]. Our results are in accordance with the previous studies which also demonstrated that alcohol consumption is associated with a lower GCS score [8,9]. It has been observed in our study that alcohol intoxication can cause significant difficulties in in-hospital triage of the RTI patients and one of the confounding factors of GCS score and other vitals including BP heart rate etc.
Another study from Taiwan shows low ISS score and mortality in blunt head injury patients who were not tested for blood alcohol concentration as compared to those tested. In our study also ISS and mortality rate was found lower in alcohol negative RTI patients compared to positive alcohol group. However, there are some contradictory studies of the impact of alcohol intoxication on the GCS score in trauma patients. Several studies have shown that alcohol consumption not associated with reduction in the GCS score of trauma patients [10-12]. Our study results shows that RTI patients with alcohol positive have low GCS and high ISS and they were admitted in ICU and stayed on ventilator support for longer duration as compared to alcohol negative group which is may be because these patients were in severe condition then the other group of patients when brought to ED. The problem of drunken driving and its consequences is not only an urban phenomenon but is more concerning in highway crashes.
This study revealed that alcohol intoxicated patients have lower initial GCS and a higher need for definitive airway, ventilation, ICU stay, higher mean ISS and mortality as compared to non-alcoholic patients. These alcoholic intoxicated patients have longer duration of stay in ICU with ventilator support. This study revealed that GCS, mean ISS, ICU stay, ventilation time etc. have considerable impact on mortality in alcohol positive patients as compared to non-alcoholic group. The study depicts that alcohol consumption and road traffic injuries are common in urban area like Delhi. There should be more stringent policies by the government in respect to alcohol consumption and road traffic injuries. Alcohol use and road safety should be public health priorities in low and middle income countries where the burden is high.

























