info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: December 12, 2017; Published: December 15, 2017
Corresponding author: Yeon Jun Jeong, Department of General Surgery, Chonbuk National University School of Medicine, 20, Geonji-ro, Deokjin-gu, Jeonju-si, Jeollabuk-do 54907, Korea
DOI: 10.26717/BJSTR.2017.01.000598
A giant umbilical cord is a rare malformation of the umbilical cord. We report the case of a term male newborn with a 25*5cm umbilical cord and pericentric inversion of chromosome 9 [inv(9)(p12q13)] associated with a patent urachus, which required surgical repair.
Keywords: Chromosome Inversion; Giant Umbilical Cord; Operative Exploration; Patent Urachus
A giant umbilical cord is a rare anomaly of the umbilical cord that can easily be diagnosed on prenatal scan. This malformation can present as a cyst in the umbilical cordantenatally, whereas the most common symptom is leakage of urine from the umbilicuspostnatally. Although it is rare, operative exploration must be performed to repair the associated urachal remnant [1]. Here, we report the case of a new born with a diffuse giant umbilical cord and pericentric inversion of chromosome 9.
A male infant weighing 2420g was born at 36 weeks of gestation by cesarean section to a 31-year-old mother. The Apgar scores were 9 and 10 at 1 and 5minutes, respectively. Routine ultrasonography conducted in the 16th week of gestation showed cystic changes in the umbilicus, and chromosomal examination of amniotic fluid conducted in the 20th week of gestation showed 46, XY, inv (9) (p12q13). However, fetal development was progressing successfully. At delivery, the infant presented with a diffuse giant umbilical cord measuring 25cm in length and cm in diameter with a glistening surface and hydropic consistency (Figure 1). No abdominal contents were noted within the cord. The cord was clamped approximately 30cm from the abdominal wall, where it became thinner. Ultrasonography conducted when the infant was 2 days old showed a probable connection between the umbilicus and bladder, which was confirmed by a fistulogram.
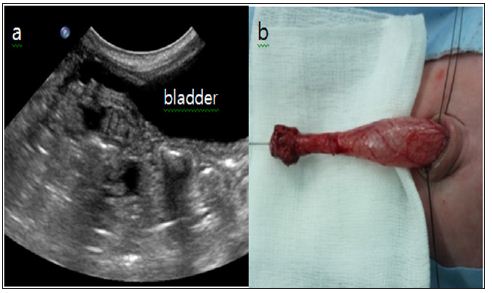
Figure 1: a. Prenatal ultrasonography image in the 34th week of gestation showing the dilated umbilical cord with edema and b. Postnatal findings of the neonate with a diffuse giant umbilical cord.

The dried umbilical stump detached after 14 days, but a granulomatous structure remained, and persistent umbilical fluid loss from the clamped umbilicus indicated urine leakage. Operative exploration was conducted via an infra umbilical incision when the infant was 16 days old. The umbilical cord was contiguous with aurachal remnant (Figure 2). Excision and repair of the urachal remnant was completed. Histological examination of the umbilical cord confirmed the presence of focal edema with no epithelial lining. On postoperative day 9, a fistulogram showed no evidence of leakage in the bladder. The infant was discharged in good health, and all follow-up examinations were normal.
Figure 2: a. Ultrasonography showing a connection between the umbilicus and bladder and b. Surgical resection performed on the 16th day of life (dissected and everted patent urachus).
A review of the literature showed that the finding of a giant umbilical cord is a patho gnomonic sign for the presence of a patent urachus, which requires surgical intervention, and only a few related case series have been published thus far [1-6] (Table 1). The exact etiology of the giant umbilical cord, however, remains unknown. One hypothesis suggests that reflux of fetal urine into the umbilical cord via the patent urachus, results in swelling of Wharton’s jelly. Wharton’s jelly of human umbilical cords was infused with distilled water, 0.9% saline, 3% saline, or 10% saline. Enlargement occurred in the umbilical cords infused with distilled water or 0/9% saline. Tsuchida and Ishida concluded that prolonged reflux of fetal urine into the umbilical cord, via a patent urachus, caused umbilical cord swelling [4]. Patent urachus arises from incomplete regression of the connection between the cloaca, which is the future bladder, and the allantois, which ist he extra embryonic urinary bladder [6].
Table 1: Summary of prior reports associated with giant umbilical cords.

Therefore, close clinical observation is necessary since continuous urinary loss from the umbilicus serves as a clinical indicator or persistent urachus. To our knowledge, cases of a giant umbilical cord with pericentric inversion of chromosome 9 have not been previously reported. Pericentric inversion in the heterochromatic region of chromosome 9 [inv (9), inv (9) (p11q13), or inv (9) (p12q13)], is the most common found in the human karyotype [7]. Although it is categorized as a minor chromosomal rearrangement that is not correlated with abnormal phenotypes, this inversion has often been reported to be associated with mental retardation or multiple congenital anomalies [8,9]. A high frequency of inv (9) (p12q13) was detected in children with dysmorphic features and congenital anomalies [10]. From our experience with this rare anomaly, we recommend that chromosomal examination along with immediate operative exploration be conducted for infants born with a giant umbilical cord. Further, imaging studies for patent urachus are also essential.

























