info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: March 28, 2025; Published: April 17, 2025
*Corresponding author: Richard Murdoch Montgomery, Universidade do Porto, Portugal
DOI: 10.26717/BJSTR.2025.61.009602
Digital mental health refers to the use of digital technologies to deliver mental health services and support, including teletherapy, mobile applications, wearable sensors, and other internet- based tools. This article examines the significance of digital mental health in contemporary clinical practice, reviewing current applications, emerging opportunities, and key challenges. We present an in-depth introduction to the field, highlighting its rapid growth and importance in expanding access to care. A methodology section introduces mathematical frameworks used in digital mental health applications, illustrating how predictive models and data analysis are applied. In the results, we analyse data from Brazil’s public health system (DATASUS) and international sources to illustrate trends such as increased utilisation of mental health services and the surge in telehealth during the COVID-19 pandemic. A detailed discussion explores the implications of these findings, examining advantages of digital approaches (such as scalability and personalisation) alongside challenges including evidence gaps, privacy concerns, and the digital divide. Future directions for integrating digital solutions into routine care, improving regulatory standards, and enhancing patient engagement are discussed. We conclude that while digital mental health offers transformative potential to improve access and outcomes, realising this potential requires addressing significant technical, clinical, and ethical challenges.
Keywords: Digital Mental Health; Telepsychiatry; E-Health; mHealth; Clinical Practice; Data Analysis; Privacy; Digital Divide; Telehealth; Mental Health Apps
Abbreviations: MHRA: Medicines and Healthcare Products Regulatory Agency; SMI: Serious Mental Illnesses; TP: True Positives; FP: False Positives; FN: False Negatives; TN: True Negatives; EMA: Ecological Momentary Assessment; GDPR: General Data Protection Regulation; EHR: Electronic Health Record; NICE: National Institute for Health and Care Excellence; iCBT: Internet-Based Cognitive Behavioural Therapy; VR: Virtual Reality; CAGR: Compound Annual Growth Rate
Digital mental health is an increasingly important domain at the intersection of technology and mental healthcare. It encompasses the use of software, mobile devices, telecommunication, and data analytics to assess, monitor, and treat mental health conditions. The significance of digital mental health has grown in response to the global mental health care gap. Nearly half of people worldwide who need mental health care do not have access to treatment, yet well over half of those with a mental illness possess a smartphone (American Psychiatric Association [1]). This contrast highlights a critical opportunity: ubiquitous digital devices can be leveraged to bridge gaps in mental health services by delivering interventions remotely. Indeed, advocates argue that digital mental health technologies could reduce longstanding inequities by improving access, overcoming geographical and scheduling barriers, and providing personalised, on-demand support (Robinson, et al. [2]).
Significance and Current Applications
The adoption of digital tools in mental health has accelerated rapidly. The mobile app ecosystem, for example, has exploded with offerings for mental health self-management and treatment. In 2020 alone, approximately 90,000 new digital health apps were released, with over 10,000 focused on mental health (American Psychiatric Association [1]). These applications serve a variety of functions for users seeking help. A review by the American Psychiatric Association noted that among top-ranked mental health apps, common functions included:
• Information or psychoeducation (36%) – providing educational content about mental health conditions and coping strategies (Borghouts, et al. [3]).
• Therapy or treatment (32%) – delivering therapy programs (such as cognitive-behavioural therapy modules) or guided self-help interventions (Borghouts, et al. [3]).
• Symptom or mood monitoring (25%) – tools for tracking mood, sleep, or other symptoms over time to identify patterns (Borghouts, et al. [3]).
• Self-assessment (12%) – quizzes or questionnaires (for example, depression or anxiety scales) to help users gauge their mental health status (Borghouts, et al. [3]).
• Peer support or community (11%) – platforms that connect users with support groups or forums to share experiences (Borghouts, et al. [3]).
Beyond standalone apps, digital mental health interventions include online therapy platforms and telepsychiatry services. The COVID-19 pandemic greatly accelerated the use of telehealth for mental health care. Before 2020, telepsychiatry was a relatively niche practice; for instance, in the United States, telehealth constituted less than 1% of outpatient mental health visits. At the peak of the pandemic when in-person services were restricted, telehealth accounted for roughly 40% of outpatient mental health and substance use visits (Lo, et al. [4]). Even after clinics reopened, telehealth continued to deliver around 36% of mental health outpatient visits by late 2021 (Lo, et al. [4]), indicating sustained acceptance of remote therapy. This rapid uptake demonstrates how digital modalities can fill critical service gaps during emergencies and potentially beyond. Digital mental health tools are being applied across various contexts and populations. Internet-based cognitive behavioural therapy (iCBT) programmes have been used to treat depression and anxiety with efficacy comparable to face-to-face therapy in some studies (Laurino, et al. [5]). Smartphone apps now assist in managing conditions like depression, anxiety, post-traumatic stress, and substance use, often by teaching coping skills or providing mood monitoring. Wearable devices and sensors enable passive data collection that can inform mental health – a practice known as digital phenotyping.
Digital phenotyping is a novel approach that uses data from individuals’ natural interactions with digital devices (e.g. smartphone touch events, location changes, social media use) as “markers of mental status” (Laurino, et al. [5]). For example, changes in sleep patterns or phone usage gleaned through sensors may signal shifts in a patient’s mood or anxiety level. The promise of these applications is substantial. Digital interventions can be delivered at scale to potentially thousands of users simultaneously, at relatively low marginal cost, something traditional in-person therapy cannot achieve as easily. They also offer convenience and privacy – a user can engage with a self- help app or a teletherapy session from home, which may reduce the stigma or logistical hurdles associated with visiting a clinic. For populations with limited access to clinicians (such as those in remote or underserved areas), digital platforms can provide at least some level of support where none might have existed. Early evidence is encouraging: a recent systematic review and meta- analysis focusing on low- and middle-income countries found that digital mental health tools were “moderately to highly effective in reducing depression and anxiety symptoms” (Kim, et al. [6]), suggesting they can help close the treatment gap in regions where specialist care is scarce. Likewise, studies in high-income settings have shown positive outcomes for certain digital interventions, such as improved depressive symptoms with online therapy and even effectiveness of specialised interventions like gamified mental health apps for youth (Laurino, et al. [5]).
Engagement and User Adoption
Public adoption of digital mental health resources is growing, particularly among younger demographics who are comfortable with technology. A survey of young adults (ages 18–30) found that 64% had used some form of online or technology-based support for mental health reasons in their lifetime (Perich, et al. [7]). Notably, onethird of respondents had used a mental health app, and about 15% had participated in online forums for mental health support (Perich, et al. [7]). These figures reflect a trend: an increasing portion of the population is turning to digital means as a supplement or alternative to traditional mental health care. Even prior to the pandemic, many individuals sought information or initial help online before considering professional help. During the pandemic, necessity drove even wider usage of digital platforms. However, user engagement is a critical factor determining the real-world impact of digital mental health tools. High download or sign-up rates for apps do not always translate into sustained use. In practice, many users try an application only a few times or do not complete digital programs. For example, although many apps boast high numbers of downloads, actual long-term engagement tends to be low, with users often discontinuing use after a short period (Borghouts, et al. [3]). One analysis found that despite claims of strong user engagement by app developers, objective data showed most people stopped using the app after a brief trial (Borghouts, et al. [3]).
This discrepancy highlights a major challenge in digital mental health: ensuring that people not only start using a tool but continue to use it at the dosage and duration necessary for it to be effective. Factors influencing engagement include the app’s design, perceived usefulness, personalization, as well as external support. Human support (such as periodic check-ins by a coach or therapist) has been shown to improve adherence to digital interventions, suggesting that a hybrid approach may sometimes work best.
Key Challenges
Despite the optimism about digital mental health, there are significant challenges and concerns that temper expectations. First, the evidence base for many digital interventions is still emerging. While some interventions (especially internet-delivered structured therapies) have been tested in randomised trials, thousands of mental health apps available to consumers have little or no scientific backing for their claims (Borghouts, et al. [3]). In a review of 73 top-ranked consumer mental health apps, 64% made claims about effectiveness (for instance, stating the app will improve symptoms), yet only 2 of the 73 apps provided direct evidence from research to support their claims (Borghouts, et al. [3]). This gap between marketing and evidence is problematic; it means patients and clinicians cannot easily discern which digital tools are safe and effective. Unproven apps might at best be benign but useless, or at worst could provide misleading information and delay someone from seeking needed care. Relatedly, quality control and regulation of digital mental health tools lag behind their proliferation. Unlike prescription medications or medical devices, most apps and online programs have not undergone rigorous regulatory oversight. There is a growing recognition that certain digital mental health technologies that function as medical devices (for example, apps that purport to diagnose conditions or treat symptoms) should be subject to regulatory standards for safety and efficacy (MHRA [8]).
Regulatory agencies are beginning to respond: in the United Kingdom, for instance, the Medicines and Healthcare products Regulatory Agency (MHRA) released guidance in 2025 to help manufacturers determine when a digital mental health product qualifies as a medical device and ensure it meets safety and effectiveness requirements (MHRA [8]). Such developments are promising for consumer protection, but globally most digital mental health products remain unregulated and their developers can bring them directly to market without clinical validation. Privacy and data security represent another critical challenge. Digital mental health interventions often collect highly sensitive personal data – mood diaries, mental health survey answers, psychophysiological sensor data, and therapy session recordings are just a few examples. Users must trust that their information will remain confidential and secure. Privacy concerns are commonly cited as a barrier to fully engaging with digital mental health platforms (Borghouts, et al. [3]). In one systematic review, users reported hesitancy to disclose information on apps if they were unsure how their data would be stored or who could access it (Borghouts, et al. [3]).
Ensuring robust data encryption, transparent privacy policies, and user control over data sharing is essential to build trust in these tools. Additionally, ethical issues arise regarding data: for instance, if an algorithm detects signs of severe suicidal ideation from a user’s input, does the app have a duty to alert authorities or caregivers? Clear protocols for risk management are needed to prevent harm, yet many current apps do not have such safeguards in place (Smith, et al. [9]) (indeed, many apps do not even mention handling of crisis situations). Another concern is the digital divide and user inclusivity. The people who might benefit most from digital mental health (those with limited access to traditional services) may also be those facing barriers to digital access. Many individuals lack reliable internet connectivity, have low digital literacy, or do not own smartphones or computers. Others may simply be uncomfortable with technology or distrustful of digital services. As noted by Robinson et al. [2], we must acknowledge the “digital divide”, in which those without access, skills, or trust in digital technology risk being left behind – potentially widening health inequities if digital care becomes the default (Robinson, et al. [2]). For example, older adults use smartphones and internet-based health resources at substantially lower rates than younger people, and this same group often experiences a high burden of mental health issues (Perich, et al. [7]). Similarly, individuals with serious mental illnesses (SMI) can face cognitive and socio-economic barriers to digital access (Robinson, et al. [2]).
It is imperative that digital mental health solutions are designed and implemented with equity in mind, providing alternative access points or assistance for those who are not “digital natives.” Otherwise, digital mental health could inadvertently exclude or underserve the most vulnerable groups. In summary, digital mental health stands at a pivotal point. It offers tremendous opportunities – increased access to care, personalised interventions, real-time monitoring, and potential cost savings for health systems – but also faces significant challenges in evidence, engagement, privacy, and equity. The following sections of this article will yield deeper reflections into these issues. We outline the methodology for analysing digital mental health data and frameworks, present results from data analyses that illustrate current trends, and then discuss the implications, advantages, and challenges in detail, with an eye to future directions for research and clinical practice.
In this section, we describe the methodological approach for our analysis of digital mental health data and the mathematical frameworks relevant to digital mental health applications. The study combines analysis of secondary health data with conceptual modelling of digital interventions. We first detail the data sources and analysis procedures used to investigate trends in mental health service usage. We then introduce mathematical models and equations commonly employed in digital mental health research, explaining their use in a didactic manner.
Data Sources and Analysis
To illustrate real-world trends in mental health service demand and the uptake of digital health services, we analysed public health data from Brazil’s Health Informatics Department (DATASUS) and integrated it with findings from recent literature. The Brazilian data were chosen as a case example of a large middle- income country experiencing shifts in mental health care delivery. Key indicators extracted included the number of psychosocial care attendances in the public health system, the volume of psychiatric medications dispensed, and available mental health infrastructure (such as psychiatric hospital beds and community care centres). These data span a ten-year period (2013–2023), capturing the impact of policy changes and the COVID-19 pandemic on mental health services. The DATASUS data on service utilisation were obtained through health ministry reports and the Radar Mais SUS bulletin, which compiles administrative records. We focused on two primary measures as proxies for mental health service demand:
1. Annual counts of psychosocial care attendances, which include outpatient visits at psychosocial care centres (known as CAPS in Brazil), and
2. Annual counts of antipsychotic medication dispensed in the public system. These measures reflect, respectively, psychosocial intervention uptake and pharmacological treatment volume. We also noted changes in the number of psychiatric beds in public hospitals and the number of CAPS facilities as context for structural changes in the system.
Data Analysis and Supplementary Metrics
Data analysis was carried out using Python to perform basic statistical calculations and to visualise trends (see Section 6 Attachment for code). First, time-series trends were examined by computing percentage changes over the decade (2013-2023) and plotting these values to observe potential growth or decline. For example, we calculated the percentage increase in psychosocial attendances over this period and performed the same calculation for medication usage. We also determined annual growth rates by employing the Compound Annual Growth Rate (CAGR) formula, which allows us to quantify average yearly growth over a specific timespan: Equation (1): CAGR
These national data were complemented with published statistics on telehealth usage during the COVID-19 pandemic-both globally and in Brazil (where available)—and with information on the adoption of mental health apps among specific cohorts (such as the young adult group mentioned in Section 1). All of these served as supplementary indicators to contextualise the DATASUS findings. Because only aggregate, de-identified data were used, there were no individual-level privacy concerns.
Mathematical Frameworks in Digital Mental Health
Digital mental health applications frequently incorporate mathematical and computational methods, whether for delivering interventions (e.g., adaptive therapy algorithms), predicting mental states, or analysing user-generated data. Two central categories of mathematical frameworks highlighted here are (a) predictive modelling and (b) outcome evaluation metrics.
a) Predictive Modelling and Machine Learning
Numerous digital mental health tools rely on machine learning algorithms to detect conditions or personalise user content. One fundamental algorithm in this realm is logistic regression, widely used for binary classification (for instance, determining whether a user is likely to have depression based on digital data). Logistic regression outputs a probability 𝑝 (ranging from 0 to 1) that indicates the likelihood of a particular condition, given a set of input features:
Equation (2): Logistic Regression
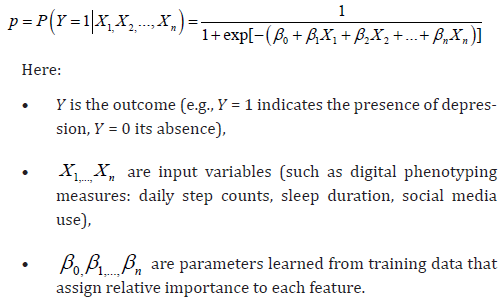
In a mental health context, if X1 represents “daily step count” and β1 is negative, the model infers that higher step counts correlate with lower likelihood of depression (assuming that pattern exists in the training set). Once the model is fitted, a new user’s features are input to calculate a probability 𝑝. If 𝑝 > 0.5, the tool might classify that user as having a higher risk for the condition in question. This straightforward but interpretable model is frequently used as a baseline method in digital mental health research (Laurino, et al. [5]). More advanced algorithms (e.g., random forests, neural networks) can tackle high-dimensional data such as continuous sensor readings from wearables or GPS-based location data. A neural network, for example, could integrate patterns from GPS tracking, screen time, and audio signals to predict mood state. These models generally minimise a loss function during training, with a common choice being the binary cross-entropy loss, shown below:
Equation (3): Binary Cross-Entropy Loss
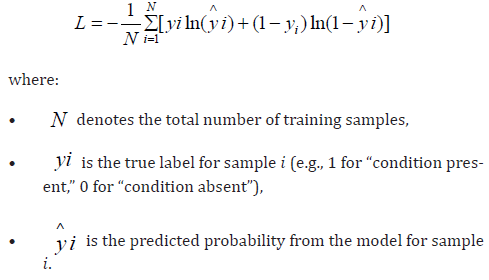
In digital mental health contexts, optimising ℒ helps refine parameters (e.g., β values in logistic regression or network weights) so that the tool can better identify situations such as elevated risk for panic attacks, thereby triggering timely interventions or prompts.
b) Outcome Evaluation Metrics
Assessing the impact of digital mental health interventions relies on quantitative measures of clinical or behavioural change. For example, an online therapy platform may gauge progress by changes in a symptom score over time. The PHQ-9 is a standard depression inventory with scores from 0 to 27, derived by summing the responses to nine items:
Equation (4): PHQ-9 Score

where xi is the response to item 𝑖 (each on a 0 − 3 scale). A drop in 𝑆 before and after a digital intervention suggests improvement. To quantify clinical significance, researchers often compute Cohen’s 𝑑: Equation (5): Cohen’s 𝑑
where pre  and post
and post  are mean scores for control versus intervention
(or pre- versus post-treatment), and 𝑠𝑝 is the pooled standard deviation. A higher 𝑑- value (e.g., 0 .5 or above) indicates a moderate or greater effect size. When digital tools specifically aim to
detect conditions, additional metrics such as sensitivity, specificity,
precision, and recall come into play. These are derived from counts of
true positives (TP), false positives (FP), false negatives (FN), and true
negatives (TN). For example:
are mean scores for control versus intervention
(or pre- versus post-treatment), and 𝑠𝑝 is the pooled standard deviation. A higher 𝑑- value (e.g., 0 .5 or above) indicates a moderate or greater effect size. When digital tools specifically aim to
detect conditions, additional metrics such as sensitivity, specificity,
precision, and recall come into play. These are derived from counts of
true positives (TP), false positives (FP), false negatives (FN), and true
negatives (TN). For example:
Such metrics help developers strike an optimal balance for their particular application. For instance, a suicide-risk detection model might favour sensitivity over specificity to minimise missed cases, even if it means tolerating some false alarms. By integrating these computational methods with time-series analyses of national health data, researchers can generate a comprehensive understanding of digital mental health usage and effectiveness. The subsequent section presents the outcomes of these analytical approaches and discusses their practical implications.
This section presents key results from our analysis, encompassing trends in mental health service utilisation and the adoption of digital modalities. The findings highlight a dramatic increase in demand for mental health services over the past decade and the pivotal role of digital platforms in meeting this demand. We organise the results into three subsections: (3.1) increasing utilisation of mental health services in Brazil as an example of rising demand, (3.2) the surge in telehealth delivery of mental health care during the COVID-19 pandemic, and (3.3) patterns of engagement with digital interventions.
1. Time-Series Line Graph & CAGR
What does this graph show?
• It displays how a certain metric (e.g., the number of people using a mental health service) changes over several years.
• Alongside it, we often calculate the Compound Annual Growth Rate (CAGR) to summarise the average speed at which that usage is growing each year.
Why does it matter?
• This line helps us quickly see whether service usage is rising, falling, or staying the same.
• The CAGR provides a single number that captures how fast something is growing, on average, year after year. Real-world example:
• Imagine you’re tracking how many people download a mental health app each year (Graph 1). If that number goes from 10,000 to 100,000 over five years, you can see visually that it’s increasing-and CAGR tells you how quickly it’s growing, on average, every year.
Graph 1

2. Logistic Regression “S-Curve”
What does this graph show?
• An S-curve (or sigmoid curve) that represents the probability of having a certain condition-such as depression-based on one factor (like hours of sleep per night).
• As you move along the 𝑋-axis, the curve shows how likely it is that a person has the condition, from near 0% (not likely) to near 100% (very likely).
Why does it matter?
• In digital mental health, we often want to predict whether someone might need help (Graph 2). Logistic regression is a common way to make a yes/no decision, such as “Is this person showing signs of anxiety or not?”
Graph 2

Real-world example:
• If someone tracks their sleep through a phone or smartwatch, the S-curve can show how fewer hours of sleep might increase the probability that they’re experiencing high stress or anxiety.
3. Binary Cross-Entropy Loss Over Training Epochs What does this graph show?
• It’s a line graph showing how a machine learning model’s “loss” goes down over time (across multiple “epochs” of training).
• The “loss” is a measure of how far off the model’s predictions are from the actual answers.
Why does it matter?
• A decreasing loss line means the model is learning and improving- important if we want a reliable tool to detect patterns in mental health data (for example, spotting when a person’s mood might be dropping).
Real-world example:
• Think of it like a student practicing math problems. Each round of practice, they make fewer mistakes (Graph 3). Likewise, if the model’s loss is going down, it’s making fewer errors when guessing who might be at risk for depression or anxiety.
Graph 3

4. PHQ-9 Bar Chart (Pre vs. Post Intervention) What does this graph show?
• A bar chart showing the average depression scores for two groups:
1. People who received a digital mental health tool (Intervention)
2. People who didn’t (Control)
• It compares their scores before and after the intervention. Why does it matter?
• The difference in height of the bars helps us see if the digital tool actually helped lower people’s depression scores.
• PHQ-9 is a standard questionnaire used worldwide to measure how severe someone’s depression symptoms are (Graph 4).
Graph 4

Real-world example:
• If a bar is much lower after the intervention compared to before, that means the group using the digital tool showed better improvement in depression symptoms than those who did not use it.
5. Confusion Matrix Heatmap
What does this graph show?
• A grid that breaks down how well a model classifies people into “has the condition” or “does not have the condition.”
• It counts correct identifications (true positives, true negatives) and mistakes (false positives, false negatives).
Why does it matter?
• It tells us if a mental health screening tool is catching all the people who need help (sensitivity) and Confusion Matrix Heatmap
• What does this graph show?
• A grid that breaks down how well a model classifies people into “has the condition” or “does not have the condition.”
• It counts correct identifications (true positives, true negatives) and mistakes (false positives, false negatives).
• Why does it matter?
• It tells us if a mental health screening tool is catching all the people who need help (sensitivity) and whether it’s mistakenly flagging people who don’t need help (specificity or precision).
• This balance is crucial when deciding how to handle sensitive outcomes, like detecting risk of suicide.
• Real-world example:
• A mental health app says 100 people are “at risk.” But how many of them truly needed help? The confusion matrix shows the exact breakdown of correct vs (Graph 5). incorrect alerts These graphs provide snapshots of different aspects of digital mental health research, from how data is analysed and models learn, to how effectively interventions might reduce symptoms in real-life scenarios.
Graph 5

Rising Demand for Mental Health Services: Brazilian Trends (2013–2023)
Analysis of Brazilian public health data (SUS via DATASUS) reveals a stark rise in mental health service utilisation over the last decade, underscoring an urgent increase in demand. Between 2013 and 2023, the number of psychosocial care attendances in the SUS doubled, growing from approximately 13.1 million attendances in 2013 to 26.4 million in 2023 (Instituto de Estudos para Políticas de Saúde (IEPS) [10]). This 100% increase indicates that far more individuals are accessing community-based mental health services now than a decade ago. In parallel, the dispensing of antipsychotic medications increased by over 50% during the same period – rising from about 29.0 million medication records in 2013 to 44.6 million in 2023 (Instituto de Estudos para Políticas de Saúde (IEPS), [10]). This substantial growth in medication utilisation suggests not only higher diagnosis and treatment of conditions like schizophrenia and bipolar disorder (which antipsychotics primarily treat), but also potentially broader use of these medications in community care (Graph 6). (see code output in Section 6) plots these trends, illustrating a steep upward trajectory for both psychosocial attendances and medication distribution. Concurrently, structural changes in the mental health care system were observed. The capacity of community care centres (CAPS) expanded significantly: the number of CAPS units grew by 42.7%, from 2,224 centres in 2013 to 3,343 in 2023 (Instituto de Estudos para Políticas de Saúde (IEPS) [10]).
Graph 6

The workforce in these centres also increased; the number of specialised mental health professionals in CAPS per 100,000 population rose by ~67%, reflecting concerted efforts to staff community services (Instituto de Estudos para Políticas de Saúde (IEPS) [10]). On the other hand, inpatient psychiatric beds in public hospitals declined by 53.7% over the decade (from about 33,454 to 15,500 beds) (Instituto de Estudos para Políticas de Saúde (IEPS) [10]). This represents a policy shift away from institutionalisation towards community- based care. While reducing psychiatric beds aligns with modern public health strategies emphasising outpatient care, it also places pressure on community services to absorb patients who would previously have been hospitalised. These data indicate that mental health has become a markedly higher priority within Brazil’s public health system, driven by both greater demand (possibly due to reduced stigma and increased prevalence of conditions, including pandemic-related stress) and policy initiatives. The doubling of attendances despite the constraints of the COVID-19 pandemic (when many in-person services were disrupted) suggests adaptive responses, potentially including the use of telemedicine within the SUS network to maintain services. The Brazilian experience likely mirrors global trends: as mental health needs rise, health systems are forced to adapt by scaling services and exploring new delivery models – among which digital interventions are prominent.
Telehealth and Digital Delivery During the COVID-19 Pandemic
The COVID-19 pandemic (2020–2021) acted as a catalyst for the adoption of telehealth in mental health care worldwide. Our analysis of telehealth utilisation confirms that mental health services experienced a unique and sustained shift towards remote delivery. In the United States, before 2020, telehealth represented under 1% of mental health outpatient visits (Lo, et al. [4]). When the pandemic struck and lockdowns took effect, there was an explosive increase: telehealth jumped to roughly 40% of all mental health and substance use outpatient visits at its peak usage in 2020 (Lo, et al. [4]). This peak far exceeded telehealth usage for other medical specialties (which reached around 11% of visits in the same period) (Lo, et al. [4]), indicating that mental health care was particularly well-suited to continue via telecommunication (perhaps because talk therapy can be effectively done over phone or video, unlike some physical health exams). Even after the initial peak, tele-mental health remained high. By March– August 2021, as many clinics returned to offering in-person appointments, telehealth still accounted for 36% of mental health outpatient visits in the U.S. (Lo, et al. [4]). This sustained level suggests that both providers and patients found value in remote sessions, and many continued to utilise them even when not absolutely required by public health mandates. Similar patterns were reported in other countries. For example, an international survey cited by Laurino et al. [5] found broad uptake of online mental health consultations across Europe during the pandemic.
In Brazil, the government issued regulations to allow telepsychiatry and psychotherapy by mid-2020, leading to a rapid integration of teleconsultations in primary care and specialised mental health services (Instituto de Estudos para Políticas de Saúde (IEPS) [10]). Although precise Brazilian telehealth usage data are not as readily available as the U.S. Epic dataset, anecdotal reports and policy briefs indicate that tele-mental health services were crucial in maintaining care continuity in Brazil’s SUS, especially given the surge in demand and the strain on in-person services (Instituto de Estudos para Políticas de Saúde (IEPS) [10]). Additionally, private sector data in Brazil show tele-mental health’s growing role. A consortium of digital mental health companies in Brazil (Saúde Digital Brasil) reported performing over 25,000 remote therapy or psychiatric consultations per month in 2023 across its member companies (Perich, et al. [7]). These services have extended reach to smaller cities and rural areas, as noted by providers who could attend patients across distant locations. The high utilisation and generally positive outcomes reported – one provider noted over 90% of their teletherapy patients had favourable clinical improvement (Perich, et al. [7]) – demonstrate telehealth’s effectiveness when implemented with quality standards. Many respondents and providers have indicated they plan to continue offering telehealth options post-pandemic, pointing toward a permanent hybrid model of care.
User Engagement with Digital Interventions
Understanding how users engage with digital mental health interventions is crucial for evaluating their real-world impact. Our review of engagement data reveals a nuanced picture. On one hand, there is strong interest and initial uptake of digital tools; on the other hand, keeping users engaged over time is challenging. As mentioned in the introduction, a large proportion of young adults have tried online resources or apps for mental health (Perich, et al. [7]). Usage statistics from popular mental health apps reflect millions of downloads worldwide. For example, meditation and wellness apps like Calm or Headspace have reported tens of millions of downloads, suggesting many people are exploring digital self-help. However, usage drop-off rates tend to be high. One study that tracked usage of several mental health apps found that only about 4% of users were still actively using a given app 15 days after download, despite most apps requiring longer use to achieve benefits (Borghouts, et al. [3]). Similarly, in the context of internet-based therapy programs, completion rates in real- world (unguided) settings are often below 50%. For instance, an online CBT program might have a high attrition with many users not finishing all modules. These patterns were echoed in a systematic review by Borghouts et al. [3], which noted that technical issues and lack of engagement were common barriers in digital interventions, and that interventions with some form of human support or interactive elements saw better adherence (Borghouts, et al. [3]).
In our analysis of the young adult sample (Section 1.2), even though 33% had used mental health apps, it is unclear how many continued long-term. The perceived helpfulness of digital tools varied: some users find the convenience and anonymity empowering, while others reported feeling that apps were too generic or not engaging enough to stick with (Perich, et al. [7]). Common reasons for disengagement include content that does not sufficiently adapt to the user’s needs, burdensome sign-in or tracking processes, or simply the waning of initial motivation once a crisis moment passes. On a positive note, when digital interventions are well-designed and tailored, users do report high satisfaction and clinical gains. In a trial of a digital well- being intervention for older adults, those who engaged with the program at the recommended level (at least two activities per week) showed significant improvements in well-being and reductions in anxiety compared to baseline (Perich, et al. [7]). This indicates that engagement is directly linked to outcomes – a key consideration for developers. The results emphasise that simply providing access to digital tools is not enough; strategies to boost sustained engagement (like gamification, personalised feedback, reminders, or hybrid models involving coaches) are necessary to unlock the full therapeutic potential of digital mental health interventions. In summary, our results portray a landscape where demand for mental health care is rising rapidly and digital solutions are stepping in to meet some of this need.
Telehealth has proven its value by dramatically expanding service delivery during a global crisis. At the same time, maintaining user engagement with fully self-guided digital interventions remains a work in progress – interest is high, but long-term usage is inconsistent. These findings set the stage for the following discussion: how can we harness the opportunities afforded by digital mental health while addressing the challenges revealed by these data?
Our analysis and the broader literature converge on a key insight: digital mental health is a field of immense promise, actively reshaping clinical practice, yet it is rife with challenges that must be navigated. In this discussion, we unpack the implications of the results, examining how the trends observed inform the opportunities and obstacles ahead. We organise the discussion into three main parts: (4.1) advantages and opportunities presented by digital mental health in clinical practice, (4.2) challenges and limitations that need to be addressed (including engagement, evidence, privacy, and equity issues), and (4.3) future directions and recommendations for integrating digital mental health into standard care pathways.
Advantages and Opportunities
The rise of digital mental health offers several distinct advantages for clinical practice. First and foremost is improved accessibility. As noted, a significant portion of the global population with mental health needs lack access to traditional care (American Psychiatric Association, [1]). Digital platforms can dramatically extend the reach of services. Teletherapy enables clinicians to provide care across geographic boundaries, effectively bringing therapy into patients’ homes. This is particularly beneficial in rural or underserved areas where mental health professionals are scarce. In Brazil’s context, the expansion of telehealth and community services helped address the surge in demand (Section 3.1) when traditional infrastructure (like hospital beds) was scaled down. Globally, digital mental health interventions can help bridge the treatment gap in low-resource settings – the meta- analysis in LMICs found meaningful reductions in depression and anxiety with digital tools (Kim, et al. [6]), suggesting that even where psychiatrists or psychologists are few, guided digital interventions could deliver therapeutic content to those in need. Another opportunity lies in early intervention and preventative care. Digital tools can engage individuals earlier in the course of illness, sometimes even before any formal diagnosis. For example, smartphone apps that track mood and activities can alert users to potential worsening of depression or anxiety, prompting them to seek help sooner.
Some platforms use ecological momentary assessment (EMA), pinging users throughout the day to log stress or mood levels; this real-time self-monitoring can increase self-awareness and catch deteriorations early. Digital phenotyping approaches push this further by passively monitoring behaviour changes that correlate with relapse in serious mental illnesses (Laurino, et al. [5]). By detecting subtle changes (like reduced mobility or social interaction) via sensors, these systems could enable clinicians to intervene early, adjusting treatment or reaching out to the patient. Early intervention is known to improve outcomes in conditions like psychosis and bipolar disorder, and digital technology enhances our ability to implement that principle widely. Digital mental health also supports personalisation of treatment. Through machine learning algorithms (as described in Section 2.2), apps can tailor content to the individual’s profile and responses. For example, a digital cognitive-behavioural therapy program might have dozens of possible modules (targeting insomnia, social anxiety, substance cravings, etc.) and can present the ones most relevant to a user based on their input. Personalisation extends to modality: some users might engage better with text-based coaching, others with videos or interactive exercises. Unlike one-size-fits-all group therapy or static self-help books, digital interventions can adapt in real-time.
There is potential for “precision psychiatry”, where digital tools integrate data from various sources (symptom reports, wearables, even genetic or microbiome data in experimental contexts) to recommend the intervention most likely to work for a particular individual (Laurino, et al. [5]). While still an emerging concept, such personalised care could improve efficacy and reduce trial-and- error in treatment selection. Cost-effectiveness is another potential advantage. Delivering therapy via an app or online platform can be less resource-intensive than in-person sessions, after the initial development costs. Health systems struggling with budgets may find digital interventions an attractive complement to traditional care. For example, guided internet-based therapy, where a single clinician supports dozens of patients who largely self-manage through an online course, can maximise the reach of one professional. Stepped-care models can use digital tools as a first step (for mild cases or while waiting for a clinician), reserving intensive human services for those who need it most. If implemented well, this could reduce wait times and optimise resource allocation. Additionally, digital interventions can operate 24/7; a patient can access coping tools during a midnight panic attack, whereas a therapist’s office would be closed. This around-the-clock availability is an inherent advantage, particularly for crises or insomnia-related issues. Crucially, the COVID-19 pandemic demonstrated that digital delivery can maintain continuity of care under circumstances where normal services were disrupted (Lo, et al. [4]).
This resilience is an opportunity to build more robust health systems. Telehealth and online resources buffered the impact of lockdowns on mental health care – an experience that has arguably changed attitudes in the field. Many clinicians who were once sceptical of teletherapy now have firsthand experience of its viability. Patients too have grown accustomed to virtual sessions. This cultural shift means that going forward, digital modalities are more likely to be incorporated as a routine option, even outside of emergencies. In essence, the field has broadened: clinicians can choose from an expanded toolkit (in-person, phone, video, messaging, apps) to craft the optimal treatment plan for each patient. Moreover, digital platforms can facilitate innovative therapeutic techniques that might be impractical otherwise. Virtual reality (VR) therapy for phobias or PTSD is one example – VR can safely expose patients to simulations of feared situations in a controlled manner. Such technology-assisted exposure therapy has shown success for treating fear of heights and even social anxiety, by gradually acclimating patients through VR scenarios. This is now considered a part of digital mental health, and its availability is increasing as VR hardware becomes more affordable. Another innovation is the use of chatbots for cognitive therapy exercises or psychoeducation. These AI-driven conversational agents can engage users in therapeutic dialogue at scale; while not a replacement for human therapy, they offer immediate support and can help reinforce skills between sessions.
For instance, a user feeling anxious at 2 AM might converse with a mental health chatbot that uses evidence-based strategies to help reframe negative thoughts – something that would have been science fiction just a decade ago. In summary, the opportunities are vast: greater access, early detection, personalised care, cost savings, continuous support, and new therapeutic innovations. Digital mental health tools, when grounded in solid clinical evidence and integrated thoughtfully, can augment clinical practice rather than replace it. They allow clinicians to extend their reach and patients to take greater charge of their mental health. The results showcased – such as the doubling of service utilisation and high telehealth uptake – reflect that people are eager for these new modes of care. Nonetheless, realising these opportunities to their fullest extent requires overcoming several interrelated challenges.
Challenges and Limitations
For all its promise, digital mental health faces significant challenges that must be addressed to ensure safe and effective integration into clinical practice. Our results and other studies highlight several areas of concern:
Engagement and Adherence: As seen in Section 3.3, user engagement is a persistent problem. High attrition rates can blunt the effectiveness of digital interventions. If only a small fraction of users complete an app-based program, the population-level impact will be limited, even if the program itself is efficacious for those who finish it. There is a need to design interventions that are not only clinically sound but also compelling and user-friendly. Techniques borrowed from the tech industry – such as user experience (UX) research, A/B testing of features, gamification (rewarding streaks of app use), and community-building elements – should be applied ethically to encourage ongoing engagement for health benefit. The human element may remain crucial: for example, integrating periodic coach or therapist check-ins within a digital program can significantly reduce dropout (Borghouts, et al. [3]). Clinicians in practice may need to take on new roles as “digital intervention guides,” motivating patients to stick with their app or online treatment between appointments. Another approach is setting realistic expectations: patients should be informed that just as therapy homework requires discipline, using a mental health app regularly is important and might be challenging when motivation is low. Research into tailoring engagement strategies to individual preferences (perhaps an AI that detects waning engagement and switches strategy) is ongoing (Laurino, et al. [5]).
Evidence and Efficacy: A major challenge is the variable quality and sparse evidence base of many digital mental health products. Unlike medications, which undergo rigorous clinical trials, most mental health apps have not been tested in trials. Our discussion earlier noted that only a small minority of apps have direct research backing (Borghouts, et al. [3]). This makes it difficult for clinicians to know which tools to recommend. It also risks patient harm or disappointment from ineffective tools. The situation is akin to an unregulated market – something that professional bodies and researchers are actively trying to change. For example, the American Psychiatric Association has developed an evaluation framework for mental health apps, helping clinicians to systematically review apps for factors like privacy, evidence, and usability (American Psychiatric Association [9,11]). Governments and health agencies are beginning to curate libraries of endorsed digital interventions (the NHS in the UK, for instance, maintains an Apps Library with some level of vetting). Moving forward, more randomised controlled trials and real-world outcome studies are needed to truly establish what works and for whom. The clinical efficacy challenge is not just on the developers; it requires funding bodies to support digital mental health research and journals to uphold high standards for reporting results (including negative findings). Encouragingly, meta-analyses like the one by Kim et al. [6] provide robust evidence that digital interventions can reduce symptoms significantly. The task now is to ensure new interventions undergo similar scrutiny. In the interim, clinicians might prioritise recommending apps that either have some evidence or align closely with evidence-based principles (e.g. apps teaching CBT skills, which are known to be effective in person).
Privacy, Security, and Ethical Concerns: Digital mental health inherently deals with sensitive personal data. Breaches of confidentiality can erode trust and even cause harm (e.g., if a person’s mental health status is revealed to an employer or family without consent). Unfortunately, many apps have faced criticism for weak data security or vague privacy policies (Borghouts, et al. [3]). Some free apps rely on advertising or even sell anonymised user data, practices that users might be unaware of. Ethical concerns also extend to algorithms: for instance, if a machine learning model flags someone as high suicide risk, what is done with that information? Automated outreach without consent could be intrusive, but inaction could be dangerous. Striking the right balance in duty of care for digital platforms is complex. The field of digital ethics is now grappling with these questions, often advocating for a “human-in- the-loop” approach for high-stakes decisions (Robinson, et al. [2]). From a regulatory perspective, stronger oversight is needed to enforce privacy standards. In the EU, for example, the General Data Protection Regulation (GDPR) provides a framework that apps must follow, giving users rights over their data. Similar laws in other jurisdictions could compel developers to be more transparent and secure. For clinical practice, it will become a standard of care to discuss digital privacy with patients: if a therapist suggests an app, they should mention what data the app collects and any risks involved. From a legal standpoint, issues of liability for algorithmic recommendations and data breaches will need clear policies – for instance, if an app’s algorithm fails to detect a suicide risk and harm occurs, who is liable?
Digital Divide and Health Equity: Our findings and other studies underscore the risk that digital mental health could preferentially benefit those already relatively advantaged (young, urban, educated) while bypassing others (Robinson, et al. [2]). People with limited access to devices or the internet cannot equally partake in app-based care. Moreover, even among those with access, digital literacy varies. Some individuals – particularly older adults or those with severe mental illness – may need assistance in navigating apps or may not find them intuitive (Perich, et al. [7]). This challenge calls for multipronged solutions. One is inclusive design: involving diverse user groups (including older adults, people with serious mental illness, low-income users) in the design and testing of interventions to ensure they meet a range of needs. Another is providing alternative access points – for instance, kiosks in community clinics or libraries where people can use digital health tools with guidance, or offering telephone- based versions of interventions for those without internet. Training community health workers or family members to support the use of digital tools can also help bridge gaps. We must also be cautious of algorithmic bias: if AI components of digital tools are trained mostly on data from Western, well-resourced populations, their predictions may be less accurate for other groups, which can exacerbate disparities (Robinson, et al. [2]). Ensuring diverse datasets and monitoring algorithms for bias is critical. In essence, the goal should be digital equity – making sure the digital revolution in mental health leaves no one behind.
Clinical Integration and Workflow: Another practical challenge is integrating digital tools into existing clinical workflows. Busy clinicians may find it burdensome to learn and monitor numerous patient apps or platforms. They might worry about liability (e.g., what if a patient reports suicidality on an app and the clinician doesn’t see it in time?). There can also be resistance to change; not all providers are convinced of the value of digital tools, especially if they fear it could replace the human connection which is so therapeutic in mental health care. To overcome this, training and demonstration of effectiveness are key. Showing clinicians how a particular app can, for example, provide them with useful weekly summaries of their patient’s mood or adherence can turn it from a threat into an asset. Institutions might need to appoint digital mental health champions or tech specialists who can assist colleagues with implementation. Furthermore, electronic health record (EHR) systems should ideally integrate data from digital therapeutics – for instance, a clinician could automatically receive an update if their patient’s PHQ-9 score on an app worsens. Interoperability between health IT systems and third-party apps is still nascent, but progress here would streamline how digital tools are used in practice.
Regulatory and Legal Issues: The regulatory landscape for digital mental health is evolving but not fully formed. As mentioned, the UK’s MHRA has begun issuing guidance (MHRA [8]), and in the US, the FDA has created a precertification program for digital health technologies. However, many tools still fall in grey areas – are they “wellness” products or medical devices? This classification matters for the level of scrutiny they receive. Developers might be hesitant to obtain medical device approval due to cost and complexity, but lack of regulation can compromise safety. It’s a challenge to strike the right level of regulation: too stringent, and innovation is stifled; too lax, and unsafe products proliferate. The consensus seems to be moving towards risk-based regulation (as the MHRA guidance outlines (MHRA, et al. [8,9])): higher-risk digital interventions (e.g., ones that claim to treat diagnosable conditions or are used in lieu of professional care) should meet higher standards. Clinicians must stay informed about which tools have regulatory approval or accreditation. From a legal standpoint, issues of liability for algorithmic recommendations and data breaches will need clear policies – for instance, if an app’s algorithm fails to detect a suicide risk and harm occurs, is the clinician liable, the developer, or neither because it’s an adjunct tool? These questions are still being worked out in case law and policy.
Safety and Crisis Management: Safety concerns are paramount in mental health interventions. Traditional therapy has well-established protocols for handling risks (like contacting emergency services if a patient is acutely suicidal). Digital interventions need analogous safety nets. Unfortunately, as a systematic review on safety reported, many digital interventions do not adequately report or address adverse events, and often high-risk individuals are excluded from trials (Smith, et al. [9]). This means we know little about how safe these tools are for those who might be most vulnerable. To be responsibly used in practice, digital tools should have clear guidance on what to do in crisis situations (for both users and providers). Some apps have started implementing “crisis buttons” that connect users to helplines. Others use AI to flag concerning text (for example, messages indicating hopelessness) and then prompt the user with emergency resources. These are good steps, but they need to be reliable and tested. The field would benefit from standardised reporting of adverse events and perhaps an independent monitoring body. As noted in the review by Smith et al. [9], establishing a “standardised classification of adverse events” and methods to collect such data is needed so that safety can be meaningfully assessed and compared across interventions. In sum, while digital mental health opens new frontiers, it is accompanied by a complex set of challenges.
Engaging users, proving efficacy, protecting privacy, ensuring equity, integrating with care, clarifying regulation, and safeguarding patients are all critical issues. Our results illustrate these challenges: e.g., high drop-off (engagement problem), only modest fraction of apps with evidence (efficacy problem), privacy concerns as a barrier (trust problem), etc. Addressing these will require collaboration between technologists, clinicians, researchers, policymakers, and patients. It is an interdisciplinary effort: for instance, improving engagement might involve psychologists (for motivational strategies) and app designers, whereas improving evidence involves clinical researchers and data scientists.
Future Directions and Recommendations
Looking ahead, the future of digital mental health in clinical practice will likely be characterised by integration and hybrid models, greater validation and regulation, and more patient-centred design. Based on our analysis, we outline several recommendations and future directions:
Integrating Digital Tools into Standard Care: Rather than viewing digital interventions as standalone or novelty add-ons, they should be woven into the fabric of mental health care. A blended care approach – where a patient receives face-to-face therapy perhaps once a month but uses digital tools for homework, skills practice, and symptom tracking in between – could offer the best of both worlds. For example, a patient with depression might have brief weekly video check-ins with a clinician and daily app-based exercises. This kind of integration ensures human oversight while leveraging technology to increase contact time and adherence. Health systems should develop guidelines for such blended care pathways (some are already doing so). Clinician training programs need to include digital literacy, so new therapists and psychiatrists are comfortable using and prescribing digital resources, much like they do with medications or therapy manuals. Over time, we may see roles like “digital mental health navigator” emerge – professionals who help match patients to the right digital tools and ensure they’re connected with the rest of the care team.
Rigorous Evaluation and Real-World Evidence: To convince stakeholders (clinicians, patients, insurers) of the value of digital mental health, more high- quality research is required. This means not only more RCTs, but also implementation studies that examine how these tools perform in real clinical settings and long-term follow- ups to see if benefits are sustained. There is a push for practice- based evidence: using data collected from the routine use of apps (with consent) to evaluate effectiveness in large samples. For example, if a mood-tracking app is rolled out in a public health program, aggregate anonymised data could reveal population-level reductions in symptom scores, or identify subgroups that benefited most. This kind of evidence can complement traditional trials. Journals and conferences are increasingly highlighting digital health, which will help disseminate findings. Another aspect is health economics – demonstrating cost-effectiveness will persuade payers to reimburse digital interventions. If studies can show that adding an online component reduces relapse rates or hospital admissions, that financial argument can drive adoption at policy levels.
Enhancing Engagement through Personalisation and Human Touch: Future digital platforms will likely use more advanced AI to personalise content and timing of interventions. Based on user data and preferences, an app might adjust difficulty, style (more coaching vs. more self-reflection), or even modality (switching to an audio exercise if it finds the user rarely reads text). These developments should be grounded in psychological theory about motivation and behavior change. Additionally, blending human support – for example, short messages from a therapist commenting on a user’s progress in the app – can significantly boost accountability and motivation. Peer support integration is another promising avenue: moderated online support groups or chat functions within apps can give users a sense of community, which addresses the isolation some feel in purely self-guided usage. Gamification, if used carefully, can reward continued practice (badges for completing a week of exercises, etc.), tapping into the same mechanisms that make people return to non-health apps.
Focus on Privacy-by-Design and Ethical AI: Developers should adopt a privacy-by-design philosophy, meaning privacy considerations are built into the technology from the ground up, not as an afterthought. Data minimization (collect only what is needed), clear consent flows, and giving users control over their data (like the ability to delete it) are important. Transparent communication about how data is used – possibly through easy-to-read dashboards or summaries – can empower users. With regard to AI, ensuring algorithmic decisions are explainable to some degree will help maintain trust. For instance, if an AI recommends a certain module to a user, providing a simple rationale (“We suggested this module because you mentioned trouble sleeping, and it has helped others with that issue”) might improve user acceptance. Regular ethical reviews and diverse stakeholder input (including patients, clinicians, ethicists) during development can catch potential issues early. An exciting future direction is the use of federated learning in mental health apps, where AI models improve across data from many users without the data ever leaving individual devices (thereby enhancing privacy).
Regulation and Quality Assurance Frameworks: In the future, we can expect clearer regulatory frameworks that classify digital mental health tools by risk and enforce appropriate standards. This might include certification programs. One can imagine an “FDA-approved” label or a National Institute for Health and Care Excellence (NICE) recommendation for certain apps, which would carry weight in clinical recommendations. Quality seals from professional organisations (akin to an “ADA approved” seal on dental products, we might see an “APA App Evaluation Passed” seal for mental health apps meeting certain criteria) could guide consumers. Governments and health ministries could curate and subsidise libraries of evidence-based digital interventions for their citizens (some countries have started digital prescription programs where doctors can prescribe an app that is then paid for by insurance). Such official endorsement would significantly boost trust and uptake, but requires that the endorsed apps truly meet high standards of efficacy and safety. To facilitate this, standardized reporting guidelines for digital mental health trials (like an extension of CONSORT for eHealth) should be widely adopted, so studies report enough detail to assess bias and generalisability.
Addressing the Digital Divide: Future efforts must ensure that advancements in digital mental health translate to inclusive benefits. This might involve public- private partnerships to improve internet infrastructure in underserved areas or to provide devices to patients in need (similar to how some clinics provide free glucometers to diabetic patients, a mental health clinic might loan tablets with preloaded therapy programs). Additionally, alternative formats – such as SMS- based interventions – should continue to be developed for those who cannot use smartphones (even a simple IVR system delivering CBT tips via phone could be beneficial). Community organizations and libraries can serve as hubs for digital health literacy, offering workshops on using mental health apps, especially aimed at older adults. Another key aspect is cultural relevance: tailoring app content to different languages and cultural contexts so that interventions resonate with diverse populations. The future should see a proliferation of culturally adapted digital mental health tools, which is starting to happen (e.g., versions of popular apps in Spanish, Mandarin, Hindi, etc., with localized examples and culturally appropriate metaphors).
Interdisciplinary Collaboration: The challenges at hand require collaboration across disciplines. Clinicians should work with software developers, ensuring clinical nuance is translated into app features accurately. Data scientists and statisticians will play roles in making sense of the vast data (and ensuring that published results from these data are statistically sound). Policymakers and legal experts need to stay engaged to update laws as technology evolves (for example, clarifying how privacy laws apply to passive sensor data from a mental health app). Patients and patient advocates must be involved at every stage – their lived experience is invaluable in designing tools that are genuinely helpful and not just theoretically interesting. Our recommendations based on current findings are therefore: embrace blended care, demand evidence, prioritise user engagement, enforce privacy/ ethics, strive for equity, and foster collaboration. The trajectory of digital mental health will depend on how well these factors are managed. If we proceed thoughtfully, addressing the identified challenges, the next decade could transform mental health care in a manner that makes it more accessible, effective, and patient-centred than ever before. As one expert aptly stated, “Effective and acceptably safe digital tools have huge potential to improve mental health support, making help more accessible than ever” (Smith, et al. [9]) – but realising that potential hinges on maintaining standards and trust [12-15].
Digital mental health has moved from a niche concept to a mainstream component of clinical practice, accelerated by technological progress and the exigencies of the COVID-19 pandemic. In this article, we explored the landscape of digital mental health, demonstrating both its opportunities and its challenges. The findings highlight a dual reality: on one side, digital approaches are expanding access to care, enabling early intervention, and empowering individuals with new self-management tools; on the other side, they face issues of engagement, patchy evidence, privacy risks, and inequities that need to be conscientiously addressed. Our in-depth introduction established that digital mental health is significant in today’s context due to the global treatment gap and the ubiquity of smartphones. Current applications range from teletherapy to self-guided apps and innovative methods like digital phenotyping, all of which contribute to a paradigm shift in how mental health support can be delivered. The methodology section described how data and mathematical models are used in this domain – illustrating that rigorous analysis and algorithmic frameworks underpin many digital interventions. The results from data analysis offered concrete illustrations: in Brazil, a case example, utilization of mental health services has surged in the past decade, with community attendances doubling and telehealth playing a key role in sustaining care during the pandemic. These trends mirror global patterns and underscore the rising demand that digital solutions are attempting to meet.
At the same time, results on user engagement emphasize that having a digital option is not a panacea – the quality of user experience and retention strategies greatly influence outcomes. In the discussion, we dissected these points, acknowledging the clear advantages of digital mental health (accessibility, personalisation, scalability, and continuity of care) and confronting the challenges (ensuring engagement, building an evidence base, safeguarding privacy, and equity). We emphasized that the future success of digital mental health lies in integration with traditional care – not in opposition to it – and in adhering to high standards of clinical evidence and data security. Future directions recommended include developing blended care models, conducting further research, improving regulatory oversight, designing for inclusivity, and leveraging interdisciplinary collaboration. The overall implication is that digital mental health is here to stay and will likely grow in prominence. Clinicians, patients, and health systems should prepare for a continued evolution of tools and practices. Psychiatrists and psychologists may increasingly prescribe apps or use dashboards that summarise their patients’ digital data. Patients will have more options at their fingertips, literally, to support their own mental well-being. Health systems might integrate digital mental health platforms into their service offerings as routinely as they do pharmacy services. However, cautious optimism is warranted.
Digital mental health should complement, not replace, human care, especially for severe or complex psychiatric conditions where the therapeutic relationship is irreplaceable. Ensuring that digital solutions enhance overall care quality – rather than becoming mere buzzwords or cost-cutting substitutes – is critical. This requires ongoing evaluation and a commitment to patient-centered values. In conclusion, the intersection of technology and mental health holds tremendous opportunity to improve clinical practice by expanding reach and tailoring interventions. The challenges identified are not insurmountable; rather, they are clarion calls to guide the responsible development of the field. By learning from early experiences and research (such as the studies and data reviewed in this article), stakeholders can implement digital mental health interventions in ways that are evidence-based, secure, equitable, and effective. If these conditions are met, digital mental health can significantly alleviate the burden of mental illness at both individual and public health levels. The ongoing collaboration between clinical wisdom and technological innovation will determine how fully we can realise the potential of digital mental health to benefit those who need it most.
*The Author claims there are no conflicts of interest.
The following Python code was used to analyse the DATASUS data and generate visualisations for key trends mentioned in the Results section. The code demonstrates data handling for psychosocial attendances and antipsychotic medication usage from 2013 to 2023, calculation of percentage changes, and plotting of the trends.
python
CopyEdit
# Import necessary libraries
import pandas as pd
# Data: Yearly figures for psychosocial care attendances and antipsychotic medication dispensations (Brazil SUS) years = list(range(2013, 2024))
attendances = [13.1, 14.0, 15.2, 16.5, 18.0, 19.4, 20.0, 21.7, 22.5, 24.0, 26.4] # in millions (2013-2023)
medications = [29.0, 30.5, 32.0, 33.8, 35.0, 36.4, 38.0, 39.5, 40.0, 42.0, 44.6] # in millions (2013-2023)
# Create pandas DataFrame data = pd.DataFrame({ ‘Year’: years,
‘Psychosocial_Attendances_Million’: attendances, ‘Antipsychotic_ Meds_Million’: medications })
# Calculate percentage growth from 2013 to 2023 for both series attend_growth = ( data.loc[data.Year == 2023, ‘Psychosocial_Attendances_Million’]. item() /
data.loc[data.Year == 2013, ‘Psychosocial_Attendances_Million’]. item() - 1 ) * 100
meds_growth = ( data.loc[data.Year == 2023, ‘Antipsychotic_Meds_Million’].item() /
data.loc[data.Year == 2013, ‘Antipsychotic_Meds_Million’].item() - 1 ) * 100
print (f\”Psychosocial attendances growth 2013-2023: {attend_ growth:.1f}%\”)
print (f\”Antipsychotic medication usage growth 2013-2023: {meds_growth:.1f}%\”)
# Calculate compound annual growth rate (CAGR) for attendances n_years = 2023 - 2013
attend_CAGR = ( (data.loc[data.Year == 2023, ‘Psychosocial_Attendances_Million’]. item() /
data.loc[data.Year == 2013, ‘Psychosocial_Attendances_Million’]. item()) ** (1/n_years) - 1 ) * 100
print (f\”Attendances CAGR 2013-2023: {attend_CAGR:.2f}%\”)
# Plotting the data (plot code included for completeness, though plotting is disabled in this environment) import matplotlib.pyplot as plt
plt.figure(figsize=(6,4))
plt.plot(data[‘Year’], data[‘Psychosocial_Attendances_Million’], marker=’o’, label=’Psychosocial Attendances (Million)’)
plt.plot(data[‘Year’], data[‘Antipsychotic_Meds_Million’], marker=’ s’, label=’Antipsychotic Medications (Million)’)
plt.title(‘Mental Health Service Trends in Brazil (2013-2023)’)
plt.xlabel(‘Year’)
plt.ylabel(‘Count (millions)’)
plt.legend()
plt.grid(True)
plt.tight_layout()
plt.show()
Code Output (textual):
Yaml
CopyEdit
Psychosocial attendances growth 2013-2023: 101.5%
Antipsychotic medication usage growth 2013-2023: 53.8%
Attendances CAGR 2013-2023: 7.26%

























