 Review Article
Review ArticleAbstract
Aim: In this article, we analyze the socio-demographic factors that determine the case fatality rate of Covid-19 across developing and developed world.
Introduction: Covid-19’s first case was reported in Wuhan, china and then it spreads throughout the world causing high fatalities. Contrary to prediction, it causes low fatalities in low-income countries. There are certain factors which need to be explored. Although currently there is limited data available about Covid-19 pandemic; however, there are number of factors which are strikingly different in both contrasting world and might be the reason for difference of covid-19 death ratio among different countries. Based on available data, our study will elaborate some factors such as population age structure, BCG vaccination, Malaria incidence and strain of human coronavirus and immune host response system as the main factors in determining this low case fatality rate of covid-19, in low-income countries.
Materials & Study: It is a review article analyzing various factors to emphasize the understanding of some key elements which are not focused yet.
Results & Conclusion: By reviewing original and review articles, moreover, the online material by webpage emphasize on the importance of health system and population age structure. It appeals further research on some factors which might help in some new discovery as medicine is a continuing education.
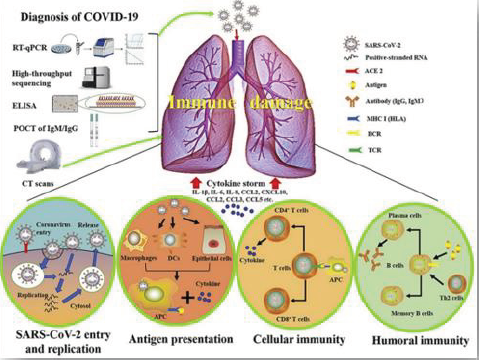
Molecular immune pathogenesis of Covid-19 (Graph 1) [1].
Keywords: Covid-19; Socio-demographic factors; BCG vaccine; Chloroquine and Hydroxychloroquine; Population age structure
Introduction
The covid-19 pandemic has serious outcomes on world in terms
of economic destabilization, mortalities, worsening of morbidities
and a state of unreality. The SARS-COV-2 emerged as a viral illness
in Wuhan province of china and in a short time becomes pandemic
because of its high infectivity, virulence and having ability to spread
in incubation period. This virus belongs to coronavirus family and
it cause mainly respiratory tract illness. Covid-19 cause severity of
symptoms in patients with comorbidities and elderly. Other than
respiratory symptoms, it causes multi-inflammatory syndrome
in children and presentation of this syndrome is unusual and has
some features in similarities with Kawasaki disease [2].
There are various drug trials for treatment of covid-19;
however, no drug regimen is approved by FDA till now.
This review article will explain the few factors that why there
is difference in reported case numbers and case fatality rate in
developing and developed countries. The symptoms, duration of
symptoms and response to treatment vary in individuals; thus, it
is different in countries and may be due to genetic variation along
with difference of ethnicity. It is a debatable topic, and the results of
research will help to understand the disease process and to combat
infectious diseases. The subsequent text will explain few factors
which are currently not available in collaborative way.
Methods and Materials
This is a systematic review article. A literature search was done by using PubMed and google search engine for original and review articles, advisories from professional societies and expert publications since the onset of current covid-19 pandemic.
Discussion
Coronavirus are spherical or pleomorphic enveloped RNA viruses. They are transmitted via airborne droplets to nasal mucosa. Viruses replicate locally in cells of ciliated epithelium causing cell damage and inflammation. In animals, coronaviruses invade different tissues and cause a variety of disease; however, in human, it mainly causes mild upper respiratory infections [3]. However, we have witnessed severe lower respiratory tract infections (lung parenchymal infiltrates) due to coronavirus as SARS in 2002 and MERS in 2011. A novel human coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) was identified in china in December 2019 and become pandemic affecting the world’s population globally [4]. Coronavirus causes more cases and fatalities as compared to SARS and MERS [5] (Figure 1).
Figure 1: Virus causing covid-19 [5].
Mode of Transmission and Detection of Virus
SARS was first transmitted from civets to humans in china and then human-human by respiratory secretions (e.g. families, hospitals). It was mainly transmitted by respiratory droplets and invade via respiratory membrane. SARS-COV-2 was transmitted via bat to humans and then human-human by respiratory secretions and close contact makes its spread more progressively [4,5]. Detection of virus is done by using antigen/antibody by ELISA, Nasopharyngeal/oropharyngeal swab by PCR to detect nucleic acid (Figure 2).
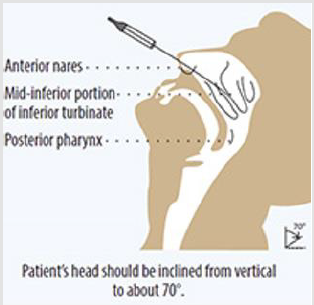
Figure 2: Taking Nasopharyngeal Swab23.
Symptoms
The period between the introduction of virus into the body and the onset of symptoms is called incubation period and it usually lasts for 4-14 days in coronavirus infection. Symptoms varies from person-person in severity and duration; however, the percentage of symptoms [5,6] are as following;
1. Fever 80-90%
2. Cough 60-70%
3. Gastrointestinal complaints 40-50%
4. Loss of sense of smell and touch 30-40%
5. Shortness of breath 20%
The percentage of unusual symptoms are not available till
date. It causes inflammatory syndrome in children and systemic
vasculitis. It is also reported that it affects clotting pathway and
cause death due to pulmonary embolism [1,7]. There are differences
between symptoms of covid-19, common cold and other allergies
(common cold is usually self-limiting and does not cause severe
myalgias (Figure 3).
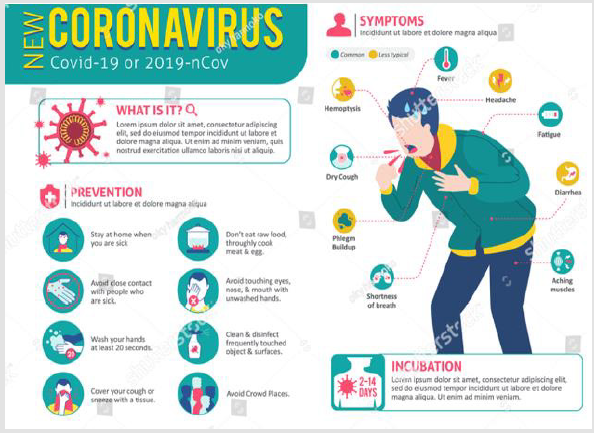
Figure 3: Symptoms ang Prevention of Covid-19.
Incidence and Mortality Rate
Reported case are increasing day by day. Total number of cases are 15,121,824 and deaths are 620,292 [8].
Case Fatality Rate
Definition: Case Fatality Rate is the proportion of deaths from
a certain disease compared to the total number of people diagnosed
with the disease for a particular period.
The case Fatality Rate of covid-19 varies in different countries
and surprisingly higher in developed countries (e.g. Europe, USA)
[8] (Table 1).
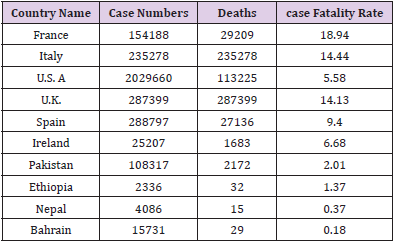
Table 1: Case number, death and case fatality rate of covid-19 in different countries [8].
Case Fatality Rate depends upon various factors; however, the major parameters of worth importance are:
a. Population age structure
b. BCG vaccination
c. Malaria incidence and use of anti-malarias
d. Viral strains and host-immune response
A. Population Age Structure
Population age structure of different countries varies and it is estimated that countries having high growth rate and young median age has low mortality rate by ovid-19 pandemic; although, it opens a new debate and will surely lead to new aspect of population studies and control strategies [9] (Table 2).
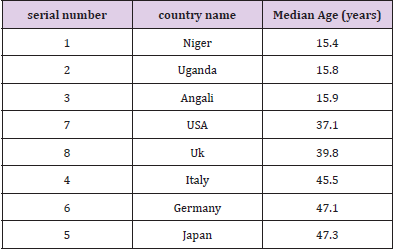
Table 2: Median age of countries.
Age has reciprocal relationship with the mortality rate of covid-19 [9] (Figure 4).
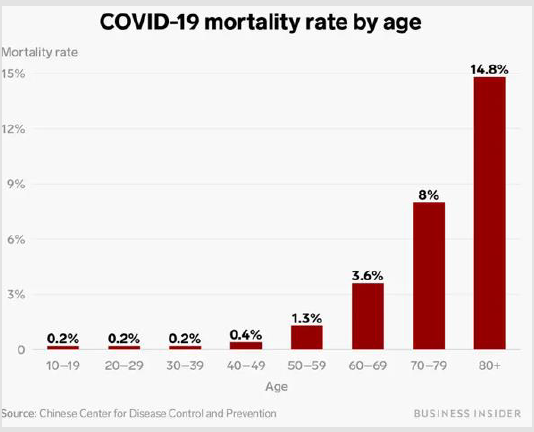
Figure 4: Mortality rate of covid-19 with age.
The mortality rate of covig-19 is surprisingly low in developing countries in contrast to predicted outcome as the countries having high growth rate and young median age shows low mortality rate as shown in below Figure 5 [10].
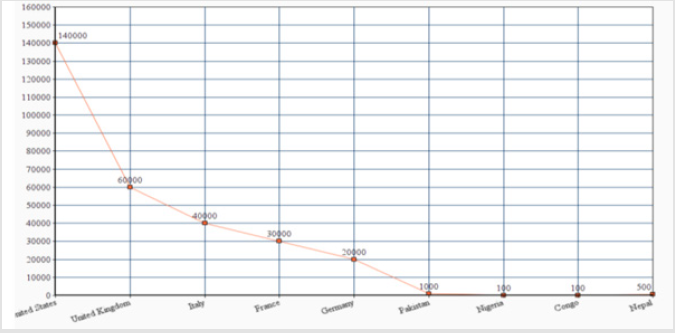
Figure 5: Graph showing case fatality rate of covid-19 in different countries.
B. BCG Vaccination and Covid-19
Bacillus-Calmette-Guerin is almost a 100-year-old vaccine
against a dreadful bacterium known as Mycobacterium Tuberculosis
which cause a disease Tuberculosis affecting different organs.
Research indicates that it is 70-80% effective in protecting against
few forms of tuberculosis (for example pulmonary tuberculosis,
tuberculosis meningitis). It is recommended as a part of Expanded
program of Immunization and administered to newborns
immediately after birth. The countries which are prioritized for BCG
vaccination due to high tuberculosis load has showed less fatality
rate due to covid-19 [5]. Tuberculosis affects different organs with
different severity; however, it initially affects lungs and spread via
respiratory droplets.
BCG protects us from Tuberculosis and other respiratory
infection (influenza, pneumonia) [11]. There is currently no
evidence that BCG helps in protection against covid-19; however,
studies in Germany and Netherland support this evidence. In the
midst of pandemic, it is early to jump on conclusion and surly it
may help to build a vaccine against covid-19 and opens a new
chapter in history [12]. Tuberculin Skin Test is an example of Type
4 hypersensitivity reaction; thus, it supports that BCG increase
one’s response to Type 4 hypersensitivity reaction (Potentiate the
host response via T-Lymphocytes), immune system part which fight
against covis-19.
C. Anti-Malarial and Covid-19
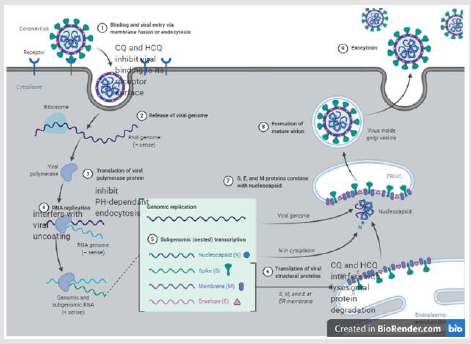
Figure 6: Chloroquine and Hydroxychloroquine interfering the viral replication cycle [14].
The Covid-19 Pandemic implies great stress and responsibility on clinicians. As morbidity and mortality rates are exceptionally high because of this pandemic, number of drug trials are used. Although Chloroquine and Hydroxychloroquine do not have enough literature in support to use as anti-viral agents. However, they are widely used as an antiviral agent in this pandemic [13] as they pose some properties to control viral replication which will be discussed below. The role of Chloroquine and Hydroxychloroquine in civid-19 will be illustrated by this Figure 6 [14].
Chloroquine and Hydroxychloroquine use in covid-19 must be rationalize due to their potential side effect as they cause renal, retinal toxicities and prolong QT interval [15]. If we look at the world map for infectivity of covid-19, there is low infectivity of covid-19 in countries which have high index of malarial infection [16]. These countries use ways to decrease vector-human contact and prophylaxis drugs to decrease malarial incidence [14,17]. This topic has a worth importance in this pandemic.
D. Viral Strains and Host-Immune Response
When a virus (infectious particle) enters into one’s body, the immune system protects it from virus. Virus considered as a foreign particle and presented to special host cells termed as T lymphocytes via Major Histocompatibility complex (MHC type 1 & 2). There are two types of T lymphocytes i-e Cytotoxic T cell and Helper T cell. Cytotoxic T cell kill the viral infected cells and remove from the body (Figure 7).
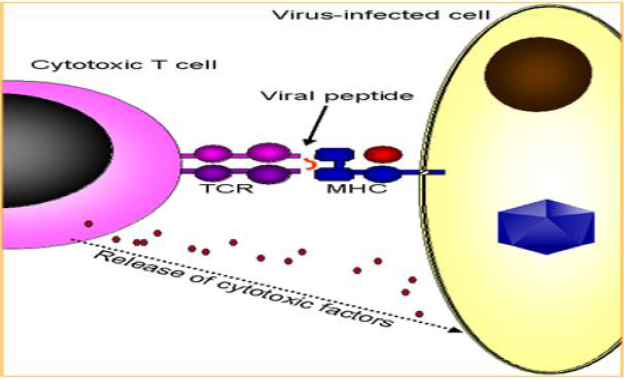
Figure 7: Viral Host Immune Response.
The immune system of body is potentiated by antibodies which are produced by B lymphocytes and help in not only augmentation of immune response but also to protect body next time by memory cells. This mechanism will not help us to save from a disease when there is a weak immune system or a different strain of infectious agent gain entry into one’s body [18].
There are various strains of human coronavirus [17];
1. 229E
2. NL63
3. OC43
4. HKU1
5. MERS-COV
6. SARS-COV
7. SARS-COV-2 (the novel coronavirus which cause 2019
pandemic, COVID-19)
People around the world are commonly infected with 229E,
NL63, OC43 HKU1 and it causes mild upper respiratory infections.
Although there is no data available to confer any immune
response variation among people across the world [9]. As the
people of Nigeria residing in USA are infected with covid-19 while
the overall disease and mortality rate statistics of both countries
varies. There is no convincing data available for genomic variation
of SARS-COV-2 [19]. A study reveals changes in genomic sequence
of human coronavirus and this variation makes changes in its
virulence. That is may be another reason for high mortality rate in
Europe, USA and China [18].
The major risk factor for covid-19 fatalities is also due to
comorbidities which are more in elderly population as compare
to young patients. Although younger people appear generally at
lower risk, everyone must adhere to government restrictions to
protect the millions of people at higher risk due to age or serious
comorbidities [20-26].
Summary
This review article emphasizes the socio-demographic factors for difference of mortality rate due to covid-19 in developing countries. This difference of case fatality rate is surprising, and it urged many researchers worldwide to re-explore the facts. There is difference in population age structure, immunization practices and use of Malarial prophylaxis along with cultural, regional and societal differences. Medicine is a continuous education and it evolves with time. There is no specific theory, thus it demands research and analysis of various factors which in result help us to fight against infectious diseases. There is limited availability of data at time; however, it opens new chapters of research in public health too and thus help to save more lives.
Acknowledgement
To all infected patients and all healthcare workers who represented the first line of defence against the disease.
References
- Li X, Geng M, Peng Y, Meng L, Lu S (2020) Molecular immune pathogenesis and diagnosis of COVID-19. J Pharm Anal 10(2): 102-108.
- (2020) Multi System Inflammatory Syndrome in Children Associated with Covid-19. Centers for Disease Control and Prevention.
- Hegarty Paul K, Ashish Kamat, Helen Zafirakis, Andrew Dinardo (2020) BCG Vaccination May Be Protective against Covid-19.
- Guo YR, Cao QD, Hong ZS, Tan YY, Chen SD, et al. (2020) The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak - an update on the status. Mil Med Res 7(1): 11.
- Levinson Warren, Ernest Jawetz (1992) Medical Microbiology & Immunology. 4th Edn, The University of Texas Medical Branch at Galveston.
- Li LQ, Huang T, Wang YQ, Wang ZP, Liang Y, et al. (2020) COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J Med Virol 92(6): 577-583.
- Clerkin Kevin J, Justin A Fried, Jayant Raikhelkar, Gabriel Sayer, Jan M Griffin, et al. (2020) COVID-19 and Cardiovascular Disease. Circulation 141(20): 1648-1655.
- (2020) Coronavirus. Worldometer.Info.
- (2020) Corona Virus Death Rate by Countries, Fatalities Compared to Cases.
- (2020) United Nations Department of Economic and Social Affairs. United Nations.
- (2015) “BCG Country Prioritization.” World Health Organization.
- Soliman Ranin, Brassey J, Pluddemann A, Heneghan C (2020) Does BCG Vaccination Protects against Respiratory Infections and Covid-19? A Rapid Review of Current Evidence.
- Hashem, Anwar M, Badrah S Alghamdi, Abdullah A Algaissi, Fahad S Alshehri, Abdullah Bukhari, et al. (2020) Therapeutic Use of Chloroquine and Hydroxychloroquine in COVID-19 and Other Viral Infections: A Narrative Review. Travel Medicine and Infectious Disease 35: 101735.
- Hegarty Paul K, Ashish Kamat, Helen Zafirakis, Andrew Dinardo (2020) BCG Vaccination May Be Protective against Covid-19.
- Voisin O, Lorc’h E le, Mahé A, Azria P, Borie MFet al. (2020) Acute QT interval modifications during hydroxychloroquine-azithromycin treatment in the context of COVID-19 infection. Mayo Clin Proc 95(8): 1696-1700.
- (2020) WHO, Malaria. World Health Organization.
- Ferner R, Aronson J (2020) Chloroquine and hydroxychloroquine in covid-19. BMJ 369: m1432.
- (2020) Immune Responses to Viruses, British Society for Immunology. British Society for Immunology.
- Saif Rashid, Tania Mahmood, Aniqa Ejaz, Saeeda Zia, Abdul Rasheed Qureshi (2020) Whole Genome Comparison of Pakistani Corona Virus with Chinese and US Strains along with Its Predictive Severity of COVID-19. BioRxiv.
- Jordan RE, Adab P, Cheng KK (2020) Covid-19: risk factors for severe disease and death. BMJ 368: m1198.
- (2020) Corona Virus Death Rate by Countries, Fatalities Compared to Cases.
- (2020) Covid-19 Global Case Fatality Rate.
- (2020) United Nations Department of Economic and Social Affairs Population. United Nations.
- Goljan, Edward F (2007) Pathology. 5th Mosby.
- Liu Y, Gayle AA, Wilder-Smith A, Rocklov J (2020) The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med 27(2): taaa021.
- Marty FM, Chen K, Verrill KA (2020) How to obtain a nasopharyngeal swab specimen. N Engl J Med 382(22): e76.
