 Mini Review
Mini ReviewAbstract
Chronic kidney disease (CKD) is a worldwide public health problem, both for the number of patients and the cost of treatment involved. A retrospective study of 2 years was conducted among CKD Stage-V (End stage renal disease) patients admitted in nephrology wards, those undergoing dialysis and kidney transplantation in SKIMS between 1st October 2015 and 30st September 2017. The prevalence of catastrophic health expenditure on ESRD patients was 95% in our retrospective study. The prevalence of distress financing on ESRD patients was 70% in our both retrospective studies.
Keywords: End Stage Renal Disease; Health; Distress; Financing, Expenditure
Introduction
Chronic Kidney Disease (CKD) is a worldwide public health
problem, both for the number of patients and the cost of treatment
involved. In India, it is reported that the progression of CKD to
End Stage Renal Disease (ESRD) is rapid due to the factors such as
lack of medical facilities, poor control of risk factors and delayed
referral to nephrologists [1]. The prevalence of CKD and ESRD are
estimated at 7852 and 1870 per million respectively [2,3]. In India,
the number of deaths due to ESRD was 3.78 million in 1990 (40.4%
of all death) and is expected to increase up to 7.73 million in 2020
(66.7% of all death) [4]. It is estimated that only 10-20% of ESRD
patients in India continue long term Renal Replacement Therapy
(RRT). It is estimated in India in 1 year, there are 3,500 new renal
transplants + 3,000 new Continuous Ambulatory Peritoneal
Dialysis (CAPD) initiation + 15,000 new Maintenance Hemodialysis
(MHD) patients [5].
Limited resources for health care and lack of protection against
catastrophic health spending have led to over-reliance on Out of
Pocket (OOP) health expenditure in India [6]. This in turn results
in exposure to high financial risk, which pushes patients and
their families into catastrophic poverty following diagnosis of life
consuming diseases like cancer & ESRD [7]. With this background,
the present study was undertaken with the prevalence of distress
financing and catastrophic health expenditure among ESRD
patients.
Aims and Objectives
To Study prevalence of distress financing and catastrophic health expenditure among ESRD patients attending SKIMS.
Material and Methods
Study Design and Duration
A retrospective study of 2 years was conducted among CKD Stage-V (End stage renal disease) patients admitted in nephrology wards, those undergoing dialysis and kidney transplantation in SKIMS between 1st October 2015 and 30st September 2017.
Sampling
Using simple random sampling, 20% of the patients admitted in nephrology wards, those undergoing dialysis and kidney transplantation in SKIMS.
Study Tool
After obtaining the list of patients admitted in nephrology wards, those undergoing dialysis and kidney transplantation in SKIMS, the patients were contacted, consent taken from them after explaining the scope and purpose of study and were subjected to a questionnaire which was pretested by conducting a pilot study. The response rate was 86%. Out of pocket expenditure, catastrophic health expenditure and distress financing was studied.
Exclusion Criteria
Those patients who refuse to participate in the study were excluded from the study
Statistical Analysis
Data was analyzed with the help of SPSS software (version 23.0). All the categorical data was shown in the form of frequency and percentages & continuous data was shown in the form of averages and standard deviations.
Results
A total of 200 patients were studied.
Distress Financing
It is defined as borrowing from family/friends, selling possessions, or taking out loans to fund expenditure of the disease (Table 1).
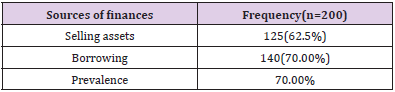
Table 1.
Catastrophic Health Expenditure
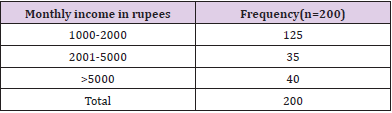
Table 2: Showing Monthly Income in Rupees.
In our study we used definition of Catastrophic health expenditure: monthly out of pocket expenditure > 25% of monthly household income. It was observed that 80% of the patients had monthly income less than or equal to 5000 rupees while 85% of the patients had monthly health expenditure more than fifteen thousand rupees. Overall prevalence of catastrophic health expenditure was found to be 95% (Tables 2,3).
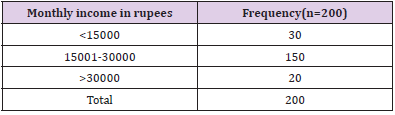
Table 3: Showing Monthly expenditure in Rupees.
Discussion
Health care delivery in India is going through a process of
transition, more so the tertiary specialty care of chronic diseases
like diabetes, hypertension, cardiac diseases, kidney or liver failure,
mental illness and cancer. Patients, more commonly those from the
lower economic strata, have difficulty in availing the health care
services because of the costs involved in diagnostic and curative
procedures. Even in public hospitals where the cost of care is low,
patient had to bear several direct and indirect costs, commonly
referred to as out-of-pocket expenditure (OOPE), which impoverish
them further. As a result, patients with life threatening diseases
requiring tertiary care often go untreated even if they are aware
of the availability of high-quality services. It can also lead to delay
in diagnostic and curative procedures and even causing deaths of
several thousands of poor patients. This issue has been a concern
for nation’s health policy, which should address the cost, quality
and accessibility of health care [8].
The prevalence of catastrophic health expenditure on ESRD
patients was 95% in our retrospective study and 96% in our
prospective study. Christina Bradshaw et al in their study reported
that 91% of ESRD patients had catastrophic health expenditure
[9]. Gunjeet Kaur et al reported in their study catastrophic health
expenditure in 40-50% patients [10]. The prevalence of distress
financing on ESRD patients was 70% in our both retrospective
and prospective studies. Christina Bradshaw et al in their study
reported that 77% of ESRD patients had distress financing [9]. The
study by Gunjeet Kaur et al reported that 60% patients had distress
financing [10].
Conclusion
Chronic kidney disease (CKD) is a worldwide public health problem, both for the number of patients and the cost of treatment involved. The prevalence of catastrophic health expenditure on ESRD patients was 95% in our retrospective study. The prevalence of distress financing on ESRD patients was 70% in our both retrospective studies.
Conflict of Interest
None
Source of Funding
None
Ethical Clearance
Taken
References
- Ballal HS (2007) The burden of chronic kidney disease in a developing country, India. Ouest 9: 12-19.
- Agarwal SK, Dash SC, Irshad M, Raju S, Singh R, et al. (2005) Prevalence of chronic renal failure in adults in Delhi, India. Nephrol Dial Transplant 20(8): 1638-1642.
- Mani MK (2003) Prevention of chronic renal failure at the community level. Kidney Int Suppl 63(83): S86-S99.
- Modi GK, Jha V (2006) The incidence of ESRD in India: A population based study. Kidney Int 70(12): 2131-2133.
- Agarwal SK, Srivastava RK (2009) Chronic kidney disease in India: challenges and solutions. Nephron Clin Pract 111(3): c197-203.
- Dielman J, Campbell M, Chapin A, Eldrenkamp E, Fan VY, et al. (2017) Evolution and patterns of global health financing 1995-2014: development assistance for health, and government, prepaid private, and out of pocket health spending in 184 countries. Lancet 389(10083): 1981-2014.
- Shahrawat R, Rao KD (2012) Insured yet vulnerable: out of pocket payments and India’s poor. Health Policy Plan 27(3): 213-221.
- Mohanti BK, Sanghamitra Das, Kuldeep S, Soumitra D (2011) Estimating the economic burden of cancer at a tertiary public hospital: a study at the All India Institute of Medical Sciences (Doctoral dissertation, Utkal University).
- Bradshaw C, Gracious N, Narayanan R, Narayanan S, Safeer M, et al. (2019) Paying for hemodialysis in Kerala, India: A description of Household Financial Hardship in the Context of Medical Subsidy. Kidney Int Rep 4(3): 390398.
- Kaur G, Prinja S, Ramachandran R, Malhotra P, Gupta KL, et al. (2018) Cost of hemodialysis in public sector tertiary hospital of India. Oxford University Press on behalf of ERA-EDTA. Clinical Kidney Journal 11(5): 726-733.
