 Research Article
Research ArticleAbstract
Several studies have attempted to find an explanation for the connection between cardiovascular disease and bacteria. This research aims to clarify this relationship by investigating the experimental induction of cardiovascular diseases exemplified by Infective Endocarditis (IE) by streptococcus mutans in Wistar albino rats, with focus on the host immune response. Streptococcus mutans serotype k (Oral pathogen) IV injection of rats with 0.3 ml of 3 X 107 CFU of was followed by examination of certain haematological, biochemical and molecular parameters identified after 1,3 and 7 days post-challenge. The haematological parameters (CBC) showed a substantial increase (P≤0.05) in WBCs, Plts, MCVs, MCHs and N percent and a significant decrease (P≤0.05) in RBC, L% and HCT. The profile of cardiac enzymes (CK, CK-MB, LDH and Troponin) was considerably elevated (P≤0.05). The inflammation biomarkers of the blood (CRP and ESR) were highly elevated (P≤0.05). Rat inflammatory cytokines (IL-1α, IL-12p70, TNF-α, MCP-1 and IFN-γ) achieved significant alteration in their levels with different patterns except for IL-10. Regarding the innate immune response exemplified here by gene expression patterns of the proinflammatory cytokines (IL1-alpha, CKM and LDHA genes) were investigated using the real time (RT-PCR) technique, the results showed high gene expression due to the induced bacterial disease.
Keywords: Infective Endocarditis, Streptococcus Mutans, innate immune response, Cytokines, CKM, LDHA and IL1-α Genes Expression, Rat
Abbreviations:IE: Infective Endocarditis; CVD: Cardiovascular Disease; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; NRC: National Research Center; AHRI: Animal Health Research Institute; CBA: Cytometric Bead Array; IV: Intravenous; PBS: Phosphate Buffered Saline; CK: Creatine Kinase; CK-MB: Creatine Kinase-MB; IFCC: International Federation of Clinical Chemistry; LDH: Lactate Dehydrogenase; ELISA: Enzyme-Linked Immunosorbent Assays; ESR: Erythrocyte Sedimentation Rate; CBC: Complete Blood Count; CBA: Cytometric Bead Array; IL-6: Interleukin-6; IL-10: Interleukin-10; MCP-1: Monocyte Chemoattractant Protein-1; IFN-γ: Interferon-γ; TNF: Tumor Necrosis Factor; PCR: Polymerase Chain Reaction; LDH: Lactate Dehydrogenase; RBCs: Red Blood Cells Count; MCV: Mean Corpuscular Volume; CKD: Chronic Kidney Diseases; RSR: Erythrocyte Sedimentation Rate; CNS: Central Nervous System
Introduction
Cardiovascular Disease (CVD) refers to more than one disease of the circulatory system including the heart and blood vessels, whether; the blood vessels are affecting the lungs, the brain, the kidneys or other parts of the body [1]. CVDs are considered as the major reason for death globally, many people die due to CVDs than other causes [2]. The WHO has predicted that by 2030, CVDs will remain the leading causes of death, affecting approximately 23.6 million people around the World [3]. Both chronic and acute infections increase the risk of cardiovascular events [4]. This risk of CVDs do not seem to be specific for one type of infection but rather seems to be a universal potential consequence of infection regardless of the organ system affected such as dental infections [5], infection of the urinary tract and upper airway [6] or systemic sepsis [7]. The involvement of oral bacteria in the pathogenesis of CVDs has been the focus of attention in many studies, and several mechanisms have been proposed to explain or support such theories, these theories indicate that the oral lesions are indicators of disease progression and oral cavity can be a window to overall health and body systems [8]. in his study reported that, oral lesions lead to systemic exposure to oral bacteria and that the resulting production of inflammatory mediators is capable of initiating or supporting mechanisms associated with the development of CVDs.
Many scientists have been trying to find a reason for the correlation between dental health and cardiovascular health [9]. By observing what microbes are found at CVD sites, they have found that Streptococcus mutans (Oral pathogen) are often prevalent at the location where the CVDs took place [10], and they refer the reason for the presence of these bacteria to that the bacteria can access these areas by entering the body during dental procedures such as root canals and tooth extractions, or by access through the rotting or infected tooth causing bacteremia [11]. If enough S. mutans enter the bloodstream, the microbes could likely reach the heart tissue. From here the microbes may attach to the endothelial cells. By binding to endothelial cells, they could infect the surface of the heart or create blockages in the heart's inner surface [12]. The fact that S. mutans can remain viable in endothelial cells for prolonged periods indicates that invasive organisms may not be readily cleared by the immune system or antibiotic treatment, potentially contributing to the establishment of chronic disease and the triggering of other pathologies associated with CVDs [10].
Infective Endocarditis (IE) is a bacterial infection of the heart valves or the endothelium of the heart [13]. It often fatal systemic disease and always associated with dental diseases. And it occurs when bacteria in the bloodstream lodge on abnormal heart valves or damaged heart tissue, and occurs rarely in people with normal hearts. So, the people who have certain preexisting heart defects are at risk for developing endocarditis when bacteremia occurs [14]. There are over 1,000 case reports associating dental procedures or disease with the onset of endocarditis [15,16]. Besides, multiple animal models (rats, rabbits and pigs) have shown that oral bacteria and even dental extraction can create endocarditis under experimental conditions [17]. From the other side, when the bacteria enter the bloodstream the immune system forms an inflammatory response to this infection. This inflammatory response can be measured by a variety of inflammatory biomarkers such as nonspecific serum markers of inflammation, including Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP), and leukocyte count (WBCs) which often elevated but are not used to make the diagnosis of acute endomyocarditis [18]. The pro-inflammatory cytokines have been implicated in cardiac dysfunction as part of the acute phase reaction [19].
Many-body systems affected by exposure to the bacteria [20], which could be investigated by measure many important haematological and biochemical parameters such as liver functions [21], kidney functions [22], cardiac profile [23], inflammatory markers [24], complete blood count [25], and measuring pro-inflammatory cytokines which act as mediators to immune response [26], these mediators are released initially at the site of inflammation by activated mononuclear phagocytes, lymphocytes, or other differentiated cell types and have potent local and systemic effects and so, and also by studying the change in some inflammatory-cardiovascular related genes expression [27]. The goal of this study is to evaluate some of Wistar albino rats immune responses towards one of the highly pathogenic bacteria (Streptococcus mutans) in concern to the hazardous endocarditis.
Materials and Methods
Biochemical investigations were developed at the biochemistry Labs of Armed Forces Central Labs, Kobry Al-Kobba, Cairo, Egypt. And the molecular biology investigations were developed in the molecular biology labs in the National Research Center (NRC), Dokki, Egypt.
Experimental Animals
A total of 60 male Wistar albino rats with 120-150 gm body weight were obtained from the animal house in the NRC, housed randomly in twelve stable wire cages (n=5 for each group) with normal temperature and photoperiod. Diets and water were given ad libitum to rats (commercial diet and tap water) and allow acclimating for one week before assay.
Pathogenic Bacteria
The bacterial strain used in this study was Streptococcus mutans pure strains SA53 (serotype k), were kindly obtained from the microbiological archive of the microbiology department, Animal Health Research Institute (AHRI), Dokki, Egypt.It came in the form of an inoculated solution ready to use. This inoculated solution contains 3 X 107 CFU∕ml (nonfatal dose).
Chemicals, Kits and Analyzers
All biochemical analyses were determined using kits purchased from Roche Diagnostics GmbH, Sandhofer Strasse 116, D-68305 Mannheim by using Roche/Hitachi Cobas c311 system. CRP latex test (manual) kit was purchased from BIOTEC Laboratories Ltd Co. (Ipswich, Suffolk, UK). Rat troponin cTnI kit (K-ASSAY) was purchased from Kamiya Biomedical Company 12779 Gateway Drive, Seattle, WA 98168. typically using commercially-available reagents developed for automated clinical immunoanalyzers (ELISA). Haematological parameters of C.B.C were determined by standard methods on automated haematology analyzer (Horiba Medical ABX Micros 60, France). And by using Reagents (Neo- Diluent-M, Neo-M-Lyse and Neo-Cleaner-M) purchased from MANUFACTURER NeoMedica d.o.o. Sv Cara Konstantina 82-86, 18000 Nis, Serbia. The inflammatory cytokines measured by using BD Cytometric Bead Array (CBA) mouse inflammation kit (Becton Dickinson Biosciences Pharmingen, San Diego, CA, USA) was used for the quantitative determination of the cytokines levels according to the instructions of the manufacturer, and by using BD CBA cytometric bead array system. QIAzol® lysis reagent (ready to use) was purchased from QIAGEN ® (AMBION, Inc., Austin, Texas USA). And Riblock™ RNase inhibitor. Revert Aid™ First Strand cDNA synthesis Kit, Polymerase Chain Reaction (Real-time PCR) using TaqMan Universal Master Mix II, with UNG. Primers for IL1A, CKM and LDHAgenes were designed using Primer 5.0 software were purchased from Fermentas life science Co. (Invitrogen Corporation) (Van Allen Way, Carlsbad, Canada).
Methods
The experiments were conducted following ethical guidelines for investigations in laboratory animals.
Experimental Design
The 60 rats were distributed in twelve different wire cages with identical physical environments, each cage contains5 rats (n=5) and each two cages were assigned as a group and its replicate, so we had 6 groups. Groups 1-3 were used as negative controls, and groups 4-6 were used as the (challenged) groups. After one week of the conditioning period we applied a process of immune system stimulation by injecting the challenge groups Intravenous (IV) in caudal vein with 0.3 ml (3 X 107 CFU/ml) of the infectious pathogenic bacteria S. mutans. Other control groups were injected with identical volume Phosphate Buffered Saline (PBS) and used as a negative control. Liver and heart tissues and blood samples were collected from the rat’s groups through three intervals of time; 1day, 3days and 7days post-challenge to carry out the haematological, biochemical and molecular investigation.
Cardiac Profile
The assays of serum Creatine Kinase (CK) activity and Creatine Kinase-MB (CK-MB) activity was determined following the recommendations of the International Federation of Clinical Chemistry (IFCC) but was optimized for performance and stability. serum Lactate Dehydrogenase (LDH) activity was determined using UV assay according to standardized method of [28]. The quantitative determination of cardiac troponin-I(cTnI) were determined using Enzyme-Linked Immunosorbent Assays (ELISA).
Biochemical Markers of Inflammation
C-reactive protein is a non-specific biochemical marker of inflammation which was measured here using ultrasensitive latex immunoassay CRP (BIOTEC Laboratories Ltd Co. (Ipswich, Suffolk, UK). Erythrocyte Sedimentation Rate (ESR) is another biomarker of inflammation, ESR was determined according to [29].
Hematological Investigation and the Inflammatory Cytokines
The haematological parameters were measured on the day of sacrifice as a Complete Blood Count (CBC). Inflammatory cytokines measured according to the manifestation of the work of BD Cytometric Bead Array (CBA) Mouse Inflammation Kit (Peruhype et al., 2006), where Interleukin-6 (IL-6), Interleukin-10 (IL-10), Monocyte Chemoattractant Protein-1 (MCP-1), Interferon-γ (IFN-γ), Tumor Necrosis Factor (TNF), and Interleukin-12p70 (IL- 12p70) protein levels were measured in every sample
Molecular Analyses
Polymerase Chain Reaction (Real-time PCR) was applied using TaqMan Universal Master Mix II, with UNG. Total RNA was extracted from the liver and heart tissues as a pool for the same individual of rats groups, according to the method of (Nicholas and Marko, 2004). RNA concentration and purity were determined by using the Nanodrop-1000 spectrophotometer. RNA integrity was checked by gel electrophoresis. According to the manufacturer’s instructions, genomic DNAwas removed from totalRNAusing the DNase I, RNasefree kit. The DNase I treated RNA was again cleaned with the Gene JET RNA Purification kit, re quantified and stored at -80ºC until used. According to the manufacturer’s instructions. The extracted total RNA was then reverse transcribed with Oligo d(T) primer according to Revert Aid First Strand cDNA Synthesis Kit™ instructions,. NCBI website (http://www.ncbi.nlm.nih.gov/) was used for searching for the target genes IL1-α, CKM and LDHA sequence and the Housekeeping (HK) gene Rattus norvegicus beta actin. The probes and primers were designed using NCBI Blast (http://blast.ncbi.nlm.nih.gov/Blast.cgi) and GenScript (http:// www.genscript.com/) web sites (Table 1).

Table 1: Illustrates the sequences of both the target and housekeeping genes.
Real-Time PCR Using Taqman Universal Master Mix II, Probes and Primers
Real time PCR was carried out using Rotor-Gene Q - QIAGEN instrument with 36 wells using Qiagen PCR Tubes for quantification of gene expression in both target and housekeeping genes. Serial dilution for primer, probe and cDNA samples were made. Concentrations of 50 picomol primer, 5 picomol prope, 1/100 for HK gene and 1/10 for target genes gave the best results (standard concentrations). PCR cycle consisted of a denaturing step for 15 second at 95ºC and annealing/extension step for 1 minutes at 60ºC. PCR amplification was performed in a final volume of 20 μl. Relative gene expression was calculated with the 2^-ΔΔCt method [30] relative to the lowest value for each gene in the whole study. Raw data of real-time threshold cycle (CT) which the real-time measurement of the concentration of the target gene expression and the internal control (Beta actin housekeeping gene) and the fold change which is often used in the analysis of gene expression data in RNA experiments, for measuring change in the expression level of a gene.
The Statistical Analysis
One-way ANOVA was used to determine differences among the treatment groups for each blood analyte. Considering statistically significant (p≤0.05), the means were compared by the use of Duncan’s multiple range test. The analyses were performed using the Statistical Package for Social Sciences Software (SPSS), version 14 (SPSS, Chicago, USA) was used as described by [31].
Results
Clinical Investigation
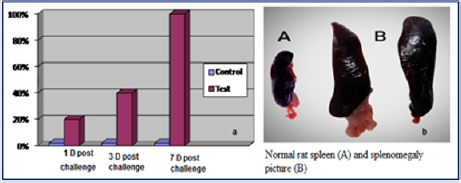
Figure 1: a= Percent of splenomegaly cases among infected groups 1, 3 and 7 days post challenge, b= Normal rat spleen (A) and splenomegaly tissue picture (B).
Experimentally infected rats showed no signs of illness that can be noticed exteriorly except one group that showed about 40% assumed to be weak and ill as signs of disease. No mortalities were recorded along the course of the experiment in all the control and the challenged groups. Investigation of the normal rats’ internal organs, showed no significant lesions where there was a prominent splenomegaly observed in the challenged rat groups ranging from 20% to 100% splenomegaly when compared to control rats. The mean spleen length was about 2.4 ml in the control groups while in the challenged groups was ranging from 3.61 ml to 5.03 ml in the challenge groups suggesting splenomegaly with observation that there was a positive relationship between time after injection and the percent of splenomegaly (Figure 1).
Cardiac Profile
Elevation in cardiac enzymes due to bacterial infections are an early indicator of heart muscle injury in studies of cardiotoxicity, in this study the cardiac profile is exemplified in CK, CK-MB, LDH and cTnI, and the data were reported in Table 2. From cardiac enzymes analyses it was revealed that, There was a highly significant increase in the serum Creatine Kinase (CK), Creatine Kinase-MB (CK-MB), Lactate Dehydrogenase (LDH) and serum Troponin (cTnI) of infected rats than those in control rats after 1, 3 and 7-days postchallenge (P≤0.05).
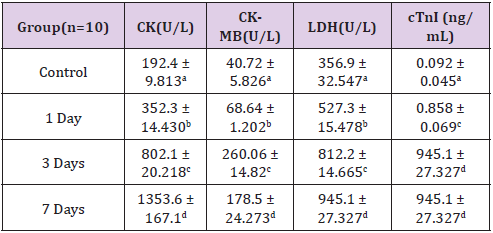
Table 2: Cardiac profile of the control and S. mutans infected rats 1-day post-challenge (mean ± S.D). Values with the different superscript letters are significantly different (P≤0.05) from the control group.
Biomarkers of Inflammation
CRP and ESR levels are associated with inflammation, they are illustrated in Figure 2. There was an observation that CRP levels have significantly increased in the of infected rats than those in control rats after 1-day, 3-days and 7-days post-challenge where ESR levels increased significantly after the first day and the 3ed day of infection but became normal after the 7th day of infection.

Figure 2: The Serum C-Reactive Protein (CRP) and Erythrocytes Sedimentation Rate (ESR) control and infected rats at 1, 3 and 7 days post-challenge (The data were represented as mean ± S.D
Haematological Parameters (CBC)
There was insignificant alterations in Haemoglobin Concentration (Hb) and basophils percentage (B%) of infected rats than those in control rats after the three intervals of time 1, 3 and 7-days post challenge, where a significant decrease in Red Blood Cells Count (RBCs), Haematocrit (HCT) and lymphocytes percentage (L%) (P≤0.05) and a significant increase in Platelets (Plts) count, White Blood Cells (WBCs), neutrophil percentage (N%), monocyte percentage (M%) and the Mean Corpuscular Volume (MCV) (P≤0.05) but insignificant increase in mean corpuscular haemoglobin concentration (MCHC) and eosinophils percentage (E%) in the infected rats than control(P≤0.05)(Figures 3 & 4).
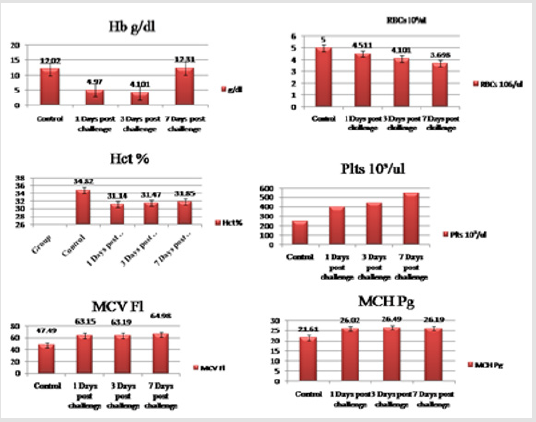
Figure 3: Haematological parameters (Hb, RBCs, HCT, Plts, MCV and MCH) of the control and challenged rat groups at 1-day, 3-days and 7-days post-challenge (The data were represented as mean ± S.D).
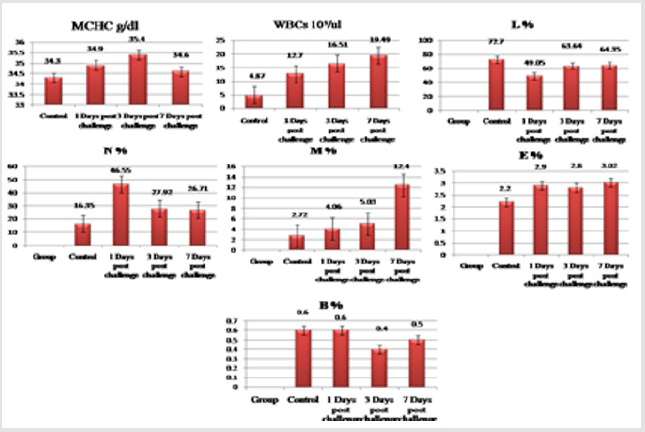
Figure 4: Haematological parameters (MCHC, WBCs, L%, N%, M%, E% and B%) of the control and challenged rat groups at 1-day, 3-days and 7-days post-challenge (The data were represented as mean ± S.D).
Serum Inflammatory Cytokines
There was a highly significant increase in the Interleukin-6 (IL6), Interferon Gamma (IFN-γ), Monocyte Chemoattractant Protein-1 (MCP-1), Interleukin-12p70 (IL12p70) and Tumor Necrosis Factor Alpha (TNF-α) of infected rats than those in control in the three intervals of time 1,3and 7 days post challenge where interleukin-10 (IL-10) showed insignificant increase between the two main tested groups; infected and control groups (Figure 5).

Figure 5: Serum interleukin-6 (IL6), interleukin-10 (IL10), interleukin-12p70 (IL12p70), Tumor Necrosis Factor Alpha (TNF-α), Interferon Gamma (IFN-γ) and Monocyte Chemoattractant Protein-1 (MCP-1) as inflammatory cytokines of the control and infected rat groups 1-day, 3-days and 7-days post-challenge (The data were represented as mean ± S.D).
Molecular Results
Raw data of real time threshold cycle (Ct) which is the real time measurement of concentration of the target genes expression in the PCR reaction after immunization with sub lethal dose of S. mutans bacteria showed an increase in the expression of the cardiac enzymes; Creatine Kinase (CK) and Lactate Dehydrogenase (LDH) and the proinflamatory cytokine (interleukin 1 alpha ) in the infected rats than the control and the internal control Beta actin after 1, 3 and 7 days post challenge with observation that the higher value of expression was clear after three days of the experimental infection followed by values after 5 days and the lowest values was clear after one day of the infection (Figure 6) compared to the internal control; beta actin gene.
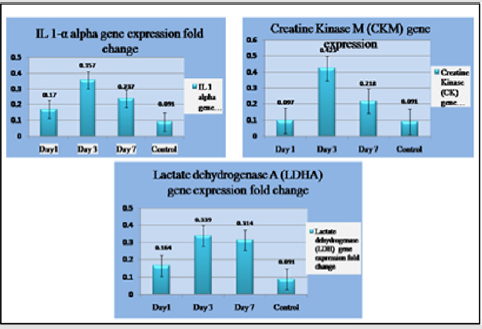
Figure 6: Gene expression of Creatine KinaseM (CKM), Lactate Dehydrogenase A(LDHA) and Interleukin 1 Alpha (IL 1-α) genes compared to beta actin; the house keeping gene 1, 3 and 7 days post challenge with S. mutans.
Discussion
Infectious disease is, by definition; is the consequence of infection by microorganisms such as bacteria, viruses, or parasites [32] Animals respond to the presence of a foreign organism by invoking several physiological changes, including rapid inflammatory changes collectively known as the acute phase response [33]. The release of mediators by resident and infiltrating cells then results in the initiation of systemic responses, including fever, leukocytosis, activation of complement and clotting systems, alterations in the plasma concentration of trace minerals, and changes in liver metabolism, including the production of acute phase proteins (APPs) [34]. Therefore, this study was initiated to evaluate the response of Wistar albino rats to the S. mutans bacterial experimental infection because it may provide insight into the pathogenic mechanisms invoked in S. mutans induced disease. S. mutans; the oral bacteria involved in the pathogenesis of cardiovascular. Several oral pathogens have been detected in diseased cardiovascular lesions, suggesting relationships between oral microorganisms and cardiovascular diseases [35]. The present study was concerned with studying developing bacterial infective endocarditis associated with biochemical, haematological and some genes expression changes induced in a group of rats experimentally infected with S. mutans.
During the experiment, the challenged rats showed no signs of illness that can be investigated exteriorly in the first 3-days post-challenge but starting in the seventh day post-challenge, some individuals (about 60% from the group) assumed to be weak and ill as signs of disease, No mortalities were recorded along the course of the experiment. Clinical investigation of the immunized rats internal organs showed a prominent splenomegaly, this splenomegaly is assumed to be induced by the S. mutans bacterial infection or may be because the acute or chronic infection (bacterial endocarditis) one of the potentials of splenomegaly, this fact was indicated in a study of [36]. Ghasemzadeh and Namazi, 2015 explained the occurrence of splenomegaly by enteritis (inflammation of the internal organs) which caused by certain strains of bacteria among human and animals . Also, the splenomegaly may be due to that the actual immune responses proceed at two sites, one being the local area peripheral to the inflammation sites (e.g. periodontium, in case of oral inflammation), and the other being in secondary lymphoid tissues, such as lymph nodes and the spleen [37]. A study of [38] on infective endocarditis patients indicated that (16.7%) of patients on his study had significant splenomegaly.
Serum chemistry testing to study organs function is imperative for bacterial infection and inflammation. The evolution of blood chemistry parameters in animals is a routine and important tool in clinical veterinary medical practice. This simple technique can provide essential information on the physiological status of animals and therefore help the clinician to make proper medical decisions (Kuldeep et al., 2019). In this study, there is a significantlly elevation in ALT, AST and ALP; the important liver enzymes activities one day post challenge but returned to the normal after 3 and 7 days, these elevations may be due to hepatic toxicity as levels of these enzymes are rapidly increased when the liver is damaged by any cause, including hepatitis or hepatic cirrhosis [39]. Increased serum activities of ALP have been explained by pathological processes such as liver impairment, kidney dysfunction, and bone disease [40] which may be systemic response due to bacterial infection. Our results also match with that of [41] who indicated that the infected patients with bacteremia had significantly higher serum levels of ALT and ALP [42]. indicated that the rats and O. niloticus infected with Colistridium perfringens showed that the liver was aggressively affected, this was proven by the significant elevation in the activities of AST, ALT and ALP enzymes in both animals challenged groups compared to the control ones, and they explained this elevation due to the liver damage caused by the bacterial infection. Ashare et al. (2006) also indicated that the mice with experimentally induced bacteremia with Pseudomonas aeruginosa showed a high elevation in ALT enzyme which specific for liver injury, and the liver shows evidence of microthrombi formation Plasma proteins are synthesized predominantly in the liver, plasma cells, lymph nodes, spleen and bone marrow. In the course of the disease, the total protein concentration and the percentage represented by individual fractions can significantly deviate from normal values (Alberghina et al., 2011). Total Protein (TP) measurements are used in the diagnosis and treatment of a variety of diseases involving the liver, kidney or bone marrow, as well as other metabolic or nutritional disorders [43], and its levels display reasonably predictable changes in response to acute inflammation, malignancy, trauma, necrosis, infarction, burns, and chemical injury [44]. Laboratory-based evidence and the epidemiological studies have investigated the association between coronary heart disease and plasma protein involved in the acute phase response [45].
In this study, there is a significant increase (P≤0.05) in the serum total protein (Hyperproteinemia) in the infected rats, this may be due to liver total protein synthesis was markedly enhanced due to the increase in the synthesis of exported proteins (acute phase proteins) [34] and may be due to response inflammatory reaction [46], and there is a significant increase (P≤0.05) in the serum albumin level (Hyperalbuminemia) as Albumin is the major protein component of serum, this may be due to hepatic disturbance as a result of tissue damage by the inflammation [47], and also there is a significant increase (P≤0.05) in the calculated globulin in serum, This increase in globulin levels accepted due to the increase in TP as result of the acute inflammatory response to the bacterial infection [48]. These acute inflammatory disorders usually produce an increase of some of the proteins from the α1-globulin fraction such as α1-antitrypsin, ceruloplasmin, haptoglobin, and α1-acid glycoprotein [33,49]. There was a significant decrease (P≤0.05) in the calculated serum A/G ratio, A/G ratios may decrease due to globulin levels rising during chronic inflammation [48], or may be due to the progress of an infection is usually associated with marked changes in the serum proteins, associated with an increase in the percentage of the total protein during some stage of the infection, and there is usually a change in the A/G ratio with an increase in the total globulins , this is in accordance to [50]. In summary, the activities of serum liver enzymes (AST, ALT and ALP) were showed a significant elevation in their activities, and also there is an elevation in the protein levels produced by the liver. So, we can say that the liver was aggressively affected by a bacterial infection in rat challenged groups.
Serum creatinine (Cr) assay is the most commonly used endogenous marker for the assessment of glomerular function [51] and is a decomposing product of creatine phosphate in the muscles, so the increase in Cr is clinically indicative of muscular dystrophy or wasting disease. Increased serum creatinine is also indicative of diseases affecting the heart muscle. In accordance with the normal conditions, creatinine is not reabsorbed by the tubules to any appreciable extent [52]. Urea and serum Blood Urea Nitrogen levels (BUN) may provide additional information on renal function as renal proximal tubular cells may increase BUN re-absorption in the setting of increased neuro-hormonal activation [53]. Measurements of uric acid are used in the diagnosis and treatment of numerous renal and metabolic disorders, including renal failure [54].
In this study, Cr levels were elevated in rats in challenged groups from the first day of the experiment and still high to the last day of the experiment. This change in serum creatinine can be explained by the fact that the increase in serum creatinine is observed only with nephron damage [51]. While urea and BUN levels are significantly increased from the third-day post-challenge. Findings from this study are in agreement with the study of [55] who reported that, there is hypertrophy of kidneys was observed in rats infected with S. mutans SA31 strain, and they added that the observations from Gram staining showed a considerable bacterial mass in the kidney, this indicates that the kidneys are target to S. mutans bacteria. Results are also in agreement with those of [56] who indicated that bacterial infection induces its toxicity on the kidney with increased serum urea and creatinine levels and also indicates that the distribution rate of S. mutans strains with collagen-binding proteins in the oral cavity is significantly greater in IgA Nephropathy (IgAN) patients than in healthy controls, suggesting that these strains are potentially involved in the mechanism of IgAN development. For clarification; IgAN is primary chronic glomerulonephritis; kidney disease [22]. indicated that bacterial infections cause renal dysfunction which occurs as part of multi-organ dysfunction due to sepsis, hypotension, hemolysis, or hepatorenal syndrome.
In contrast; this work' results contraindicate with those of [57] who indicated that the kidney of rats experimentally infected with S. faecalis was not affected and showed no significant difference in serum urea concentration measured at time 24h between experimental and control groups of rats and remained almost unchanged at 2-days and 7-days post-infection. But in agreement with study of [58] and McCullough and [59] who indicated that there is renal dysfunction has been associated with adverse cardiovascular outcomes, also match with [60] who indicated that the kidneys are commonly affected in infective endocarditis by a variety of complications of clinical significance. McCullough and [59] reported in their study that there is renal dysfunction has been associated with adverse cardiovascular outcomes. From his study [60] indicated that the kidneys are commonly affected in infective endocarditis by a variety of complications of clinical significance.
Calcium results showed a significant decrease in its levels (hypocalcemia). There are many causes of hypocalcemia, such as renal failure, pancreatitis, steatorrhea and hypoparathyroidism [61]. Hypocalcemia may also be due to protein binding because calcium levels vary with total plasma protein [62], and the difference in the concentration of Ca may also be associated to the kidney disease, where, the chronic kidney disease usually results in hypocalcemia and renal dysfunction may occur with hypercalcemia [63]. So we can say that the high elevation in the serum total protein in the challenged groups affected the total calcium level in the serum causing a decrease in its levels (hypocalcemia), and also this hypocalcemia may be due to kidney injury caused by the bacterial infection. Calcium data in this thesis in agreement with a study of [42] who indicated that rats infected with C. perfringens showed a significant decreased in the serum total calcium levels in the challenged groups after 3-days and 6-days post-challenge and with results of [64] who indicated that hypocalcemia associated with severe infections [65]. reported that hypocalcemia might be a risk factor for quinine cardiotoxicity.
Popular causes of serum electrolyte alterations include inflammation, acid-based status, changes in membrane properties, inflammatory mediators, hemodynamic alterations, and defective renal transport [66]. Potassium (K+) is a major electrolyte in the human body. It is also known as the heart mineral because it directly affects the heart muscle cells, and sodium (Na+) is one of the major cations found in extracellular fluids. Sodium salts are necessary to maintain the balance between calcium and potassium in order to maintain normal cardiac activity [67]. Serum electrolytes (Na+, K+, Ca++) values resulted in this study were none significantly different in the experimental groups when compared to the control group. So we can conclude that the infection with S. mutans does not affect levels of electrolytes in the blood. Electrolytes result of this study are in a match with [68] who indicated no significant (p>0.05) difference was observed in serum electrolytes of infected rats. Our results contraindicate with a study of [69] who found hyponatremia (decrease of Na+ level in the blood) has been observed in many infectious diseases caused by bacteria, viruses and parasites.
However; results of kidney functions indicated that the most common renal markers (urea, BUN, creatinine and total calcium) are affected by the bacterial infection, and the supplementary investigations such as (Uric acid, Na+, K+ and Ca++) not affected with the infection compared with the control groups. These may be due to their elevation occurring in Chronic Kidney Diseases (CKD) which need a longer time to occur more than the course of the experiment. Therefore, we can say the kidney is strongly affected by the bacterial infection. Concerning the Cardiac enzymes biomarkers, Creatine phosphokinase (CK), creatine kinase –MB (CK-MB) fraction, Lactate Dehydrogenase (LDH), Troponin-I (cTnI) and serum aspartate aminotransferase (AST) are currently available tools to evaluate possible cardiac injury in the non-clinical setting [70,71]. Clinically, CK is tested in blood tests as a marker for damage to CK-rich tissue, such as myocardial infarction (heart attack) autoimmune myositides, and acute kidney injury (Moghadam et al., 2016). The CK release rate (the amount of marker depleted from the myocardium that appears in the plasma) is flow-dependent, especially for CK-MB, early marker elevations may be of less significance than later, perhaps even lower, marker elevations. Myocardial release rates of biomarkers may also vary under different clinical conditions (O’Brien et al., 2011).
Lactate dehydrogenase (LDH) is an enzyme found in the liver, kidneys, skeletal muscles, platelets and catalyses the conversion of lactate to pyruvate [72]. Elevated serum levels of LDH have been observed in a variety of disease states, where it reflects the degree of destruction of cells and toxic side effects in tissues that are rich in this enzyme. Mild increases in LDH activity have been reported in cases of myocardial or pulmonary infarction, leukemia, hemolytic anemias, and hepatitis (nonviral) [72]. Cardiac troponin-I (cTnI) is a sensitive and specific marker for detecting myocardial damage. This biomarker is normally not found in the circulation. Injured cardiac muscles release troponin from the contractile proteins into the bloodstream and thus an increased level of serum cardiac troponin-I may suggest myocardial injury [73]. Serum levels of CK, CKMB, LDH and cTnI were found statistically significant to be increased in the three experimental groups of rats compared to the control group by a different pattern referring to cardiac injury. This work' cardiac profile data is matching with the studies of [74] and [57] who indicated that any external stressor, such as the bacterial infection even at a sublethal dose can have a toxicological effect on the liver and other tissues and increased the level of LDH, ALP and CK which all correlate to liver function and muscle lesions, including the myocardium. Cardiac enzymes results here are in agreement with those of [75] stated that S. mutans mainly causes the increase of enzymes involved in myocyte's injury including CK-MB and LDH. And he added leakage of CK-MB isoenzyme and LDH from myocardial tissues to blood is an indicator of acute myocardial infarction, and the amount of LDH and CK-MB level is an index for identifying the cell injury.
Troponin results confirm the hypothesis of endocarditis occurrence; this because many studies have demonstrated that there is a role of troponin I in active infective endocarditis (Sue et al., 2004); Purcell et al. (2008); Shiue et al. (2010) and Esra et al. (2015). One of the most important primary defenses against pathogens is the inflammatory process [27]. The inflammatory response can be measured by a variety of inflammatory biomarkers, such as Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP), ESR, cytokines and total leukocyte count (WBC: described in CBC) (Kim et al., 2015) [76]. The nonspecific markers of inflammation are often elevated but are not used to make the diagnosis of CVD such as IE, but due to their elevation, they may be helpful to confirm the diagnosis [77,78]. in this study, the nonspecific markers of inflammation (ESR and CRP) were found statistically significant to be increased in the three experimental groups compared to the control groups due to the effect of the infection. Rats serum CRP levels were found statistically significant (P≤0.05) to be markedly elevated by eleven-fold 1-day post-challenge, and continued to elevate 3-days post-challenge and 7-days post-challenge, this finding confirm the role of CRP is an acute phase reactant in the innate host defense, clearance of damaged cells, and regulation of the inflammatory response, and in bacterial infection [79]. So we can say that CRP is a good marker for bacteremia this is in accordance with [80].
The inflammatory markers results here is matching with those of [57] who indicated that rats infected with S. faecalis showed an increase in the ESR levels at 24 hr post-injection, and showed a high elevation in CRP concentrations due to the bacterial infection by about 16 fold increases compared with control levels at 1-day after injection [42]. indicated that rats infected with C. perfringens showed statistically significant elevation in serum CRP levels with maximal values by the third day of infection and Shaneen et al. (2010) and Sheikh et al. (2012) in their study indicated that the plasma levels of inflammatory markers such as CRP and ESR have been shown to be a stronger predictor of future cardiovascular events. One of the most important tests used in the diagnosis of the infectious diseases is Complete Blood Count (CBC) with differential count which used to help diagnose and monitor many different conditions, including anemia and infection (Xiao et al., 2016), and also helps in checking for weakness, fatigue, or bruising, that may be present in an organism (Web Medical Reference, 2010). CBC results of rats challenged groups showed that the bacterial infection caused significant difference (P<0.05) in most CBC parameters such as WBCs, RBCs, Plts, L%, N%, M%, MCV and MCH. While other parameters such as Hb, E%, B% and MCHC not influenced by a bacterial infection and showed insignificant difference (P>0.05) when compared with those of the control groups.
Significant decrease in RBCs counts and haematocrit indicate that the erythrocytes are being affected or destroyed with the infection (Harikrishnan et al., 2003 and Martins et al., 2008). A significant increase in platelets count (like in this study) which called thrombocytosis. The thrombocytosis called reactive thrombocytosis or secondary thrombocytosis when the cause is an underlying condition, such as an infection (James, 2019). Results showed significant elevation in WBCs count (Leukocytosis) at the three intervals of time 1, 3-days and 7-days post-challenge, this leukocytosis mainly due to acute inflammatory reaction (i.e neutrophilia and slight monocytosis) which was characteristic of acute infection and a consequent chronicity (Maria et al., 2004). So the rat’s defense mechanisms explain the high production of leucocytes in the challenged groups [68]. Lymphocytes percentage (L%) results showed a decrease in its levels (relative lymphopenia). The induction of Tumor Necrosis Factor (TNF) family members occurs early in the inflammatory response; these engage receptors expressed on lymphocytes and cause lymphocyte apoptosis. The decline in lymphocyte numbers seen in our study is probably the result of large scale lymphocyte apoptosis, which has been seen in several animal models of sepsis, in the spleens of humans who have died of sepsis and in the peripheral blood of patients with sepsis. (Joshi and Kalvak, 2003 and Wyllie et al., 2004).
Monocytes percentage (M%) showed an increase in its levels (relative monocytosis) which may be because these cells are directly involved in phagocytosis of foreign particles or organisms (Rosales et al., 2017). Neutrophils percentage (N%) showed an increase in its levels (relative neutrophilia) this elevation may be because the neutrophils are the first cell line of defense for the innate immune response (José et al 2018), and they are the primary white blood cells that respond to the bacterial infection. This work' results corroborate the prior finding of Wyllie et al. (2004) which state that neutrophilia and lymphopenia were both associated with bacteremia, and added both neutrophilia and lymphopenia were more predictive of bacteremia than the total white blood cell count. Also corroborate with the findings of Geovana et al. (2011) who indicated that the acute inflammatory process is composed of metabolic and cellular changes such as an increase in the white blood cell count and mainly neutrophils. The WBCs elevation in good indicator for progression of the cardiovascular events, and this in agreement with Araújo et al. (2015).
In concern to the inflammatory cytokines investigations on a biochemical base, This study revealed a significant increase in the serum levels of IL-6, IL-12p70, IFN-γ, MCP-1 and TNF-α with different patterns, while IL-10 showed an insignificant increase in its levels compared to the control groups. The mean cause for the different expression patterns of cytokines in the three intervals of time of our study back to that the levels of these cytokines correlated with both disease severity and clinical outcome (Monastero and Pentyala, 2017). The increase in the levels of IL-6, TNF-α and IFNs may be due to they are among the first cytokines produced in response to pathogenic bacteria (i.e the pro-inflammatory cytokines) (Janeway et al., 2001), the high concentration of their levels 1-day post-challenge and decreasing with time may be due to the early timing peak of these cytokines. The pro-inflammatory cytokines play an important role in both recruitment and activation of leukocytes migrating into tissues in response to invading pathogens in early stage of infection. The IL-10 makes down regulation to the pro-inflammatory cytokines such as IFN-γ, IL-12 and TNF-α. We hypothesize that the lower production of IL-10 in the bacterial infection could explain, at least in part, the more exacerbated inflammatory response and the higher clinical impact of this infection (Araújo et al., 2015). So the insignificant elevation of IL-10 allows these cytokines to rise freely (Vinicius et al., 2018). Many pro-inflammatory cytokines and inflammatory biomarkers (such as IL-6) are positively associated with the risk of cardiovascular disease (CVDs) (Welsh et al.,2011). Elevated serum IL-6 levels may suggest ongoing infective endocarditis and might be used to aid in the diagnosis and monitoring of treatment of the disease (Rawczynska et al., 2000).
[2] found that Pro-inflammatory biomarkers, such as tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6) and C-Reactive Protein (CRP), have been shown to associate with CVD risk factors. Findings from this work are in agreement with those of Ding et al. (2006) who indicated that the pro-inflammatory cytokines, including TNF-α, IL-1 and IL-6 are mainly released by macrophages in response to endotoxins secreted by bacteria, also were inconsistence with Shaneen et al. (2010) who indicated that when P. gingivalis (oral bacteria) is recognized by the innate immune system employing toll-like receptors (TLRs), many signal transduction pathways occur leading to a rapid innate inflammatory response which leads to the secretion of many pro-inflammatory molecules including IL-1, IL-6, TNF-α, and prostaglandin (E2). the cytokines findings of this study reinforce a relationship between the expression of inflammatory cytokines, especially IL-6, IL-10, IL-12p70, IFN-γ, MCP-1 and TNF-α and the infection with S. mutans. This study indicates that the immune process to the bacterial infection is very complex, and multiple mechanisms may be involved, and further studies are necessary to define the role of inflammatory cytokines in the diagnosis and prognosis of CVDs.
Investigation of the inflammatory cytokines on a molecular base revealed that the injection of rats by S. mutans induces a priming of the host immune response characterized by increased expression of IL1-α, CKM and LDHA genes in the rat tissues one, three and seven days after the bacterial infection when compared with the uninfected control rats as a response to CVD devolution with the curve peak image characterizes the normal immune response. However, it could be proven that an increase in the levels of expression of genes of the immune system results in enhanced resistance against infection [81]. reported that, to control early bacterial infection before it becomes this severe, IL-1 can help prevent a pathogen from reaching immune-privileged or vulnerable sites, such as the Central Nervous System (CNS), IL-1α is a key mediator of the sterile inflammatory response but is not generally critical for the response to bacterial infection (suggesting that IL-1α contributes to cytokine storm during sepsis, this is in accordance with our results.
The increased expression of striated muscle associated creatine phosphokinase as well as the increased release of the cardiomyocyte enzyme CK in the hearts of Wistar rats suggests that exposure to bacterial infection contributes to cardiomyocyte stress. [82], so from our data; (CK) mRNA expressions; could prove to be an important indices of cardiac cellular damage associated with the S. mutans bacterial infection [83-85]. LDH enzyme is expressed in body tissues, such as blood cells and heart muscle, it is released during tissue damage, so it is a marker of common injuries and disease such as heart failure [86,87]. Diseases that can cause increased LDH in the blood may include liver disease, heart attack, anemia, muscle trauma, cancers, and infections such as encephalitis, meningitis, and viruses [72]. The increased expression of LDH gene is an indication for the increased serum LDH and this result is consistent with [57] who indicated that any external stressor, such as the bacterial infection even at a sub lethal dose can have a toxicological effect on the liver or the heart and leading to increased level of LDH [88-90]. Stephen et al. (2010) in their study indicated that by studying some cases of myocarditis related to acute streptococcal infection [91-93], their initial laboratory findings showed an elevated troponin, together with an elevation of LDH and CPK, suggesting cardiac injury due to streptococcal infection [94,95]. However, this study suggests that S. mutans has a direct effects on the heart, liver and kidney, this may be probably explained by the release of several enzymes to the blood (e.g. heart, liver and kidney enzymes) as the cells of these organs were damaged, a phenomenon that provides the basis for clinical diagnosis [96]. Cytokines and other inflammatory profiles are good indicators and immune responses against bacterial infection to keep health in man and animal due to the prominent changes in their parameters which observed in all infected rat groups compared to the control groups [97].
Acknowledgement
We are thankful to Army Rehabilitation And Rheumatology Center for financial support and National Research Centre, Egypt for the technical assistance to carry out all investigation analysis.
Conflict of Interest
None of the authors has any financial or personal relationships that could inappropriately influence or bias the content of the paper.
References
- Ceren YF, Patricia H, Jeanne MZ, Susie C, Jean H, et al. (2017) Early Identification of Cardiovascular Diseases in People With Spinal Cord Injury: Key Information for Primary Care Providers. Archives of Physical Medicine and Rehabilitation 98(6): 1277-1279.
- Nykänen T, Pihlainen K, Kyröläinen H, Fogelholm M (2020) Associations of nutrition and body composition with cardiovascular disease risk factors in soldiers during a 6-month deployment. International Journal of Occupational Medicine and Environmental Health 33(4): 457-466.
- (2009) WHO. World Health Organization. Cardiovascular disease; Fact sheet No.317. Geneva. Switzerland.
- Cowanl LT (2017) Infection and cardiovascular disease: The atherosclerosis risk in communities study.
- Karim E, Genco RJ, Van D, Thomas E (2015) Oral infections and cardiovascular disease. Journal Trends in Endocrinology and Metabolism 26(6): 315-321.
- Clayton TC, Gaskin M, Meade TW (2011) Recent respiratory infection and risk of venous thromboembolism: case-control study through a general practice database. International journal of epidemiology 40(3): 819-827.
- Mankowski RT, Yende S, Angus DC (2019) Long-term impact of sepsis on cardiovascular health. Intensive care medicine 45(1): 78-81.
- Karnoutsos K, Papastergiou P, Stefanidis S, Vakaloudi A (2008) Periodontitis as a risk factor for cardiovascular disease: The role of anti-phosphorylcholine and anti-cardiolipin antibodies. HIPPOKRATIA 12(3): 144-149.
- Sanchez P, Everett B, Salamonson Y, Ajwani S, Bhole S, et al. (2017) Oral health and cardiovascular care: Perceptions of people with cardiovascular disease. PloS one 12(7): e0181189.
- Abranches J, Zeng L, Bélanger M, Rodrigues PH, Simpson HP J, et al. (2009) Invasion of human coronary artery endothelial cells by Streptococcus mutans Oral Microbiol Immunol 24(2): 141-145.
- Nakano K, Inaba H, Nomura R, Nemoto H, Takeda M, et al. (2006) Detection of cariogenic Streptococcus mutans in extirpated heart valve and atheromatous plaque Specimens. J Clin Microbiol 44(9): 3313-3317.
- Reyes L, Herrera D, Kozarov E, Roldan S, Progulske FA (2013) Periodontal bacterial invasion and infection: contribution to atherosclerotic pathology. J Periodontol 84(Suppl-4): S30-S50.
- Stach C (2015) Characterizing the role of the enterotoxin gene cluster in staphylococcus aureus
- Paik S (2004) Molecular analysis of virulence determinants for endocarditis in Streptococcus mutans and Streptococcus sanguis.
- Chen PC, Tung YC, Wu PW, Wu LS, Lin YS, et al. (2015) Dental Procedures and the Risk of Infective Endocarditis. Medicine 94(43): e1826.
- Taubert KA, Wilson W (2017) Is endocarditis prophylaxis for dental procedures necessary? Heart Asia 9(1): 63-67.
- Li X, Kolltveit KM, Tronstad L, Olsen I (2000) Systemic diseases caused by oral infection. Clinical Microbiology Reviews 13(4): 547-558.
- Bansal T, Pandey AD D, Asthana AK (2014) C-reactive protein (CRP) and its association with periodontal disease: A Brief Review. Journal of clinical and diagnostic research. JCDR 8(7): ZE21-ZE24.
- Mohan ML, Vasudevan NT, Naga PS V (2017) Proinflammatory cytokines mediate GPCR dysfunction. Journal of cardiovascular pharmacology 70(2): 61-73.
- Drexler M (2010) Institute of Medicine (US): What You Need to Know About Infectious Disease. Washington (DC): National Academies Press (US).
- Cai J, Zhang M, Han T, Jiang H (2017) Characteristics of infection and its impact on short-term outcome in patients with acute-on-chronic liver failure. Medicine 96(37): e8057.
- Prasad N, Patel MR (2018) Infection-Induced Kidney Diseases. Frontiers in medicine 5: 327.
- Makara MA, Hoang KV, Ganesan LP, Crouser ED, Gunn JS, et al. (2016) Cardiac electrical and structural changes during bacterial infection: An instructive model to study cardiac dysfunction in sepsis. Journal of the American Heart Association 5(9): e003820.
- George A, George SP, John S, George N, Joe S, et al. (2015) Changes in inflammatory markers in bacterial-and nifedipine-induced gingival inflammation. Journal of international oral health: JIOH 7(Suppl 2): 64-67.
- Han Q, Wen X, Wang L, Han X, Shen Y, et al. (2020) Role of hematological parameters in the diagnosis of influenza virus infection in patients with respiratory tract infection symptoms. J Clin Lab Anal 34: e23191.
- Kany S, Vollrath JT, Relja B (2019) Cytokines in inflammatory disease. International journal of molecular sciences 20(23): 6008.
- Chen L, Deng H, Cui H, Fang J, Zuo Z, et al. (2017) Inflammatory responses and inflammation-associated diseases in organs. Oncotarget 9(6): 7204-7218.
- DGKC (1972) Recommendations of the German Society for Clinical Chemistry, standardization of methods for determining enzyme activities in biological fluids. Z Klin Chem Klin Biochem 10: 182-192.
- Westergren A (1921) Studies of the Suspension Stability of the Blood in Pulmonary Tuberculosis. Acta med Scand 54: 247-282.
- Livak KJ, Schmittgen TD (2001) Analysis of relative gene expression data using real-time quantitative PCR and the 2^-ΔΔCt method. Methods 25: 402-408.
- Dytham C (1999) Choosing and using statistics: A Biologist’s guide. Blackwell Science Oxford.
- Ralph DF (2020) Infectious disease. Encyclopædia Britannica.
- Jain S, Gautam V, Naseem S (2011) Acute-phase proteins: As diagnostic tool. Journal of pharmacy and bioallied sciences 3(1): 118-127.
- Gruys E, Toussaint MJ, Niewold TA, Koopmans SJ (2005) Acute phase reaction and acute phase proteins. Journal of Zhejiang University Science B 6(11): 1045-1056.
- Peter BL, Ann FB, Panos N, Papapanou DD S, Olusegun O, et al. (2012) Periodontal disease and atherosclerotic vascular disease: Does the evidence support an independent association? Circulation 125(20): 2520-2544.
- Chapman J, Bansal P, Goyal A, Azevedo AM (2020) Splenomegaly. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
- Azuma M (2006) Fundamental mechanisms of host immune responses to infection. J Periodont Res 41: 361-373.
- Araújo IR, Ferrari TC, Teixeira CA, Campi AA C, Rodrigues LV, et al. (2015) Cytokine Signature in Infective Endocarditis. PloS one 10(7): e0133631.
- Giannini EG, Testa R, Savarino V (2005) Liver enzyme alteration: a guide for clinicians. CMAJ 172(3): 367-379.
- Jen LY, Hon CC (2003) Serum metabolic enzyme activities and hepatocyte ultrastructure of common carp after gallium exposure. Zoological Studie 42(3): 455-461.
- Minemura M, Tajiri K, Shimizu Y (2014) Liver involvement in systemic infection. World journal of hepatology 6(9): 632-642.
- Marwa MM MA, Abd Al-Galel F, Iman MK A (2014) Zoonotic Bacterial Infection Induced Immune Responses in Fish and Rat: Biochemical and Molecular Studies. Research Journal of Pharmaceutical. Biological and Chemical Sciences. RJPBCS 5(3): 894-924.
- Melillo A (2007) Rabbit Clinical Pathology. Journal of exotic pet 16(3): 135-145.
- Theodore X, O’Connell MD, Timothy J, Horita MD, Barsam KM D (2005) Understanding and Interpreting Serum Protein Electrophoresis. Am Fam Physician 71(1): 105-112.
- Vincenzo P, Massimiliano M, Stefano P, Daniele Taccola (2000) The link of biocompatibility to cytokine production. Kidney International Biocompatibility and cytokines 58(Suppl-76): S96-S103.
- Khalil RH, Khalil RH (2020) Types of acute phase reactants and their importance in vaccination (Review): Biomedical Reports 12: 143-152.
- June SL (2012) Albumin for End-Stage Liver Disease. korean j intern med 27: 13-19.
- Koyama T, Kuriyama N, Ozaki E, Matsui D, watanabe I, et al. (2016) Serum albumin to globulin ratio is related to cognitive decline via reflection of homeostasis: a nested case-control study. BMC Neurol 16: 253.
- Tothova C, Nagy O, Kovac G (2014) Acute phase proteins and their use in the diagnosis of diseases in ruminants: a review. Veterinarni Medicina 59(4): 163-180.
- Zaitsev SY, Bogolyubova NV, Zhang X, Brenig B (2020) Biochemical parameters, dynamic tensiometry and circulating nucleic acids for cattle blood analysis: a review. PeerJ 8: e8997.
- Gounden V, Bhatt H, Jialal I (2020) Renal Function Tests. In: StatPearls [Internet]. Treasure Island (FL).
- Gowda S, Desai PB, Kulkarni SS, Hull VV, Math AA, et al. (2010) Markers of renal function tests. North American journal of medical sciences 2(4): 170-173.
- Shlipak MG, Heidenreich PA, Noguchi H, Chertow GM, Browner WS, et al. (2002) Association in renal insufficiency with treatment and outcomes after myocardial infarction in elderly patients. Ann Intern Med 137: 555-562.
- Christin G, Olga K, Kelli KM, Abdo A (2015) Uric acid as a marker of kidney disease: Review of the current literature. Hindawi Publishing Corporation Disease Markers pp. 382918.
- Ryota N, Masatoshi O, Kazuhiko N (2014) Contribution of the interaction of Streptococcus mutans serotype k strains with fibrinogen to the pathogenicity of infective endocarditis. Infection and immunity 82(12): 5223-5234.
- Taro M, Shuhei N, Keiko K, Ryota N, Tempei S, et al. (2015) Distribution of Streptococcus mutans strains with collagen-binding proteins in the oral cavity of IgA nephropathy patients. Clin Exp Nephrol 19: 844-850.
- Kholoud SR, Iman MK, Rasha EH, Soha SS (2013) The effect of experimental streptococcus infection in myocarditis on some biochemical and inflammatory markers in albino rats. African health sciences 13(4): 1062-1070.
- Aronson D, Mittleman MA, Burger AJ (2004) Elevated blood urea nitrogen level as a predictor of mortality in patients admitted for decompensated heart failure. Am J Med 116: 466-473.
- Mc Cullough PA, Ahmad A (2011) Cardiorenal syndromes. World journal of cardiology 3(1): 1-9.
- Majumdar A, Chowdhary S, Baptista M, Hammond LA, Howie AJ, et al. (2000) Renal pathological findings in infective endocarditis. Nephrology. dialysis. transplantation: official publication of the European Dialysis and Transplant Association. European Renal Association 15: 1782-1787.
- Rao MN, Shoback DM (2018) Hypocalcemia. In: Feingold K. R.; Anawalt B. and Boyce A. et al. editors. Endotext [Internet]. South Dartmouth (MA): MDText.com. Inc.
- Lindsay AL B, Marisa N, Neil SH (2014) Calcium, magnesium and phosphate review. Lab Medicine Winter 45(1): e44-e50.
- Schafer AL, Shoback DM (2016) Hypocalcemia: Diagnosis and Treatment.
- Steele T, Kolamunnage DR, Downey C, Toh CH, Welters I (2013) Assessment and clinical course of hypocalcemia in critical illness. Crit Care 17: R106.
- Soni C, Kumhar M, Gupta B, Singh V, Srimali L, et al. (2000) Prognostic Implication of Hypocalcemia and QTc Interval in Malaria. Indian journal of malariology 37: 61-67.
- Urso C, Brucculeri S, Caimi G (2015) Acid-base and electrolyte abnormalities in heart failure: pathophysiology and implications. Heart failure reviews 20(4): 493-503.
- Fox M (2013) Importance of Sodium. Living Strong Foundation.
- kanluwa TA, Odutola O, Olugbenga OA, Funmilayo DO, Sunday OO, et al. (2015) Serum electrolytes, creatinine (CRT) and hematological (Hg) indices of rats fed on processed Atlantic Horse Mackerel. Journal of Natural Sciences Research 5(3): 2224-3186.
- Daher EF, Soares DS, Filho SL, Meneses GC, Freitas TV, et al. (2017) Hyponatremia and risk factors for death in human visceral leishmaniasis: new insights from a cross-sectional study in Brazil. BMC infectious diseases 17(1): 168.
- Friedrich MG, Sechtem U, Schulz MJ, Holmvang G, Alakija P, et al. (2009) Cardiovascular magnetic resonance in myocarditis. JACC 53(17): 1475-1487.
- Patibandla S, Alsayouri K (2020) Cardiac Enzymes.
- Farhana A, Lappin SL (2020) Biochemistry, Lactate Dehydrogenase (LDH).
- Park KC, Gaze DC, Collinson PO, Marber MS (2017) Cardiac troponins: from myocardial infarction to chronic disease. Cardiovascular research 113(14): 1708-1718.
- Gupta S, Markham DW, Drazner MH, Mammen PP (2008) Fulminant myocarditis. Nature Clin Prac Cardio Med 5(11): 693-706.
- Mohammad A, Sajad J, Nasser A, Nasibe U, Jalal Z (2013) Effect of HEMADO on level of CK-MB and LDH enzymes after ischemia/reperfusion Injury in Isolated Rat Heart. BioImpacts 3(2): 101-104.
- Mostafa MA, Elewa MK, Mohamed NA (2015) Admission leukocytosis. C-reactive protein and erythrocyte sedimentation rate in acute noncardioembolic cerebral ischemia: influence on early outcome. Egypt. J Neurol Psychiatry Neurosurg 52: 223-227.
- Wilson A, Ryan M, Boyle A (2006) The novel role of C-reactive protein in cardiovascular disease: Risk marker or pathogen. International journal of cardiology 106: 291-297.
- Shrivastava AK, Singh HV, Raizada A, Singh SK (2015) C-reactive protein inflammation and coronaryheart disease. The Egyptian Heart Journal 67: 89-97.
- Janciauskiene S, Wrenger S, Welte T (2013) Immunoregulatory Properties of Acute Phase Proteins-Specific Focus on α1-Antitrypsin.
- Yang M, Choi SJ, Lee J, Lee DG, Kim YJ, et al. (2019) Serum procalcitonin as an independent diagnostic markers of bacteremia in febrile patients with hematologic malignancies. PloS one 14(12): e0225765.
- Von Moltke J, Ayres JS, Kofoed EM, Chavarría-Smith J, Vance RE (2013) Recognition of bacteria by inflammasomes. Annu Rev Immunol 31: 73-106.
- Schlattner U, Tokarska-Schlattner M, Wallimann T (2006) Mitochondrial creatine kinase in human health and disease. Biochim Biophys Acta 1762(2): 164-180.
- Alonso GR, Pérez HA, Silvestre RJ, Silvestre J (2011) Cardiovascular disease versus periodontal disease: chronic systemic infection as a link. e476. J Clin Exp Dent 3(5): e476-82. Periodontal microorganisms as a risk factor for heart disease, Journal section: Oral Medicine and Pathology.
- Basil T, Doumashomer G, Biggsrobert L, Arendspatrick V, Pinto C (1972) Determination of Serum Albumin. Standard Methods of Clinical Chemistry 7: 175-188.
- Dhadse P, Gattani D, Mishra R (2010) The link between periodontal disease and cardiovascular disease: How far we have come in last two decades? Journal of Indian Society of Periodontology 14(3): 148-154.
- Di-Giorgio J, Henry RJ (1974) Clinical Chemistry: Principles and Technics. (2nd Edn). Harper and Row, New York NY, USA, pp. 532.
- Fabiny DL, Ertinghausen G (1971) Automated reaction-rate method for determination of serum creatinine with the Centrifi Chem. Clin Chem 17: 696-700.
- Ghasemzadeh I, Namazi SH (2015) Review of bacterial and viral zoonotic infections transmitted by dogs. Journal of medicine and life 8(4): 1-5.
- Gulhar R, Ashraf MA, Jialal I (2020) Physiology. Acute Phase Reactants.
- Lamb E, Newman DJ, Price CP (2006) Kidney function tests. In: Burtis C. A.; Ashwood E. R. and Bruns D. E., Tietz textbook of clinical chemistry and molecular diagnostics. (4th). Elsevier Saunders, St. Louis. MO, USA, pp. 797-835.
- Peruhype MV, Martins FO A, Prata A, Silva LA, Rabello A, et al. (2006) Mixed inflammatory/regulatory cytokine profile marked by simultaneous raise of interferon-gamma and interleukin-10 and low frequency of tumour necrosis factor-alpha (+) monocytes are hallmarks of active human visceral Leishmaniasis due to Leishmania chagasi infection. Clin Exp Immunol 146: 124-132.
- Ruot B, Papet I, Bechereau F (2003) Increased albumin plasma efflux contributes to hypoalbuminemia only during early phase of sepsis in rats. Am J Physiol Regul Integr Comp Physiol 284(3): R707-R713.
- Sampson EJ, Baired MA, Burtis CA, Smith EM, Witte DL, et al. (1980) A coupled-enzyme equilibrium method for measuring urea in serum: Optimization and evaluation of the AACC study group on urea candidate reference method. Clin Che 26: 816-826.
- Schwarzenbach G, Ackermann H (1947) Komplexone V. Die Äthylendiamin‐tetraessigsä HCA 30: 1798-1804.
- Sharma S, Menard P, Mutchler LA (2019) Who to trust? Applying trust to social commerce. Journal of Computer Information Systems 59(1): 32-42.
- Tietz NW, Rinker AD, Shaw LM (1983) IFCC methods for the measurement of catalytic concentration of enzymes Part 5. IFCC method for alkaline phosphatase (orthophosphoric-monoester phosphohydrolase, alkaline optimum, EC 3.1.3.1). J Clin Chem Clin Biochem 21: 731-748.
- Weichselbaum TE (1946) An accurate and rapid method for the determination of proteins in small amounts of blood serum and plasma. Amer J Clin Path 10: 40-49.
