Research Article
Parental Partnership Program to Improve Resources
for Pediatric Sickle Cell Care
Krystle Stone and Betty S Pace*
Author Affiliations
Department of Pediatrics, Augusta University, Augusta, GA
Received: October 08, 2020 | Published: December 11, 2020
Corresponding author:Betty S Pace, Department of Pediatrics, Augusta University, Augusta, Georgia
DOI: 10.26717/BJSTR.2020.32.005265
Objective: The organization Parent to Parent (P2P) of Georgia is a community
organization that offers parental support as a core resource for families with children
who have special health care needs, disability, and mental health diagnoses. This study
was conducted to launch a P2P program at Children’s Hospital of Georgia.
Methods:
A Parent Partner was assigned to the Pediatric Sickle Cell Clinic at CHOG
to collect information during routine visits. The Parent Partner identified resources
such as social security administration, school forms, and resources in local community.
Information was provided to the families during clinic visits and/or by mail, telephone,
and email.
Results: During the 3-year observation period, there were 545 cases completed
at Children’s Hospital of Georgia and 635 referrals by the Parent Partners to different
services. The most common request was social security administrative resources for
supplemental security income. We proved services at: Level 1 (0-10 minutes), n=61
(11.9%); Level 2 (11-15 minutes), n=183 (33.58%); Level 3 (16-30 minutes) n=245
(44.95%); Level 4 (31-45 minutes), n=49 (9.00%); and Level 5 (>45 minutes) n=7
(1.28%). There were 104 follow up calls, which confirmed the families were becoming
more independent following up resources leads. In additional, three Supporting Parents
were certified and trained in communication and providing resources to other families
and a Parent/Patient Support Group was established.
Conclusion: This is the first P2P program for sickle cell disease. The program was
highly accepted by families and they acknowledged the importance of self-awareness
and education, and independence with providing care of their children. The P2P program
improved the quality of care, and health for families and children with sickle cell disease.
Parent to Parent of Georgia (P2P) is a national nonprofit
organization that promotes excellence in P2P programs across
the nation. P2P programs have been providing information and
referral support for families of children with special health care
needs, disabilities, or mental health diagnoses since the 1970s. P2P
believes that strength and power come when connecting parents
of children with any illness. Their mission and vision are built
from quality support, fully-functioning, and integrity [1]. Sickle cell
anemia is an autosomal recessive inherited blood disorder caused
by a single point mutation in the β-globin gene on chromosome
11. There are approximately 100,000 people living with sickle
cell disease (SCD) in the United States and millions worldwide.
Individuals with homozygous SCD make abnormal hemoglobin S
protein, which undergoes polymerization under hypoxia conditions
producing long rod-like structures in red blood cells, i.e. sickle cells.
This sickled shape leads to vaso-occlusion by blocking small blood
vessels to deprive vital organs of oxygen causing periodic acute
pain episodes, other clinical complications and early death [2]. Due
to the chronic nature of SCD and the demands required of families,
which impacts quality of life, some parents become overwhelmed
after receiving newborn screening test results. To help caregivers,
we identified community resources to improve medical outcomes.
The objective of this quality improvement evaluation was to
determine if face-to-face education using Parent Partners would improve health care delivery to children with SCD. We observed
improved compliance based on information the parents and care
givers submitted during clinic visits.
Parent Partner Collaboration: A partnership
was established between the Augusta University Pediatric
Comprehensive Sickle Cell Program at Children’s Hospital of Georgia
(CHOG) and the Parent to Parent (P2P) of Georgia. This work did
not require IRB approval since it falls under quality improvement of
care. All patient information was handle under HIPPA requirements.
After intense training by P2P for ~6 weeks, two certified Parent
Partners were assigned to CHOG during the evaluation period from
October 2014 to September 2017. The P2P organization provided
additional onsite training for CHOG hematology faculty and staff.
P2P Intake Interview: During the clinic visit, the Parent
Partner met with patient and caregiver to complete the P2P
of Georgia Referral Form and specific needs of the family was
recorded during the interview. These data were entered into a
secure database maintained by P2P; information related to social
security administration, school forms, and community resources
were identified. Information was provided to families during visits
and/or by mail, telephone, and email. Insurance and employment
status, and social services needed were established.
Database Access: After information was collected, the
Parent Partner entered into a secured database: parent(s) name,
address, phone number, email, child’s Name, gender, date of birth,
and diagnosis; also noted family needs, total time spent with family
and how information was provided to families.
Parent Partner Service Referrals: After the initial
interview, patient and care givers were follow-up by phone or
during a second visit at CHOG to ensure families received the
information requested, determine if they followed through with
service referrals, and provide additional services if needed.
Subsequently, the Parent Partner decided whether to close the case
or if additional follow-up was needed.
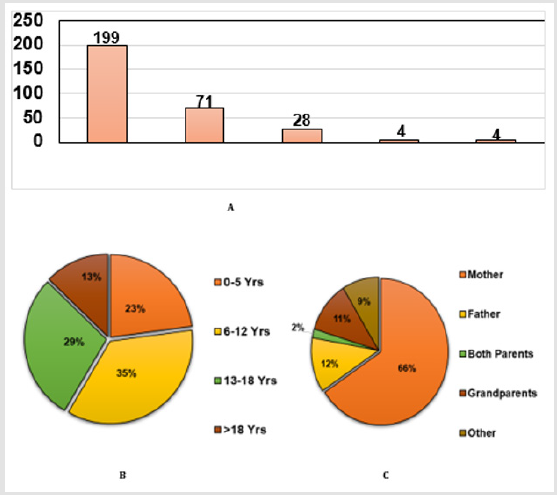
Characterization of clinic population
The Parent to Parent Program of Georgia was piloted in the
Comprehensive Sickle Cell Program (CSCP) at the CHOG where
hematology subspecialty services are provided for ~300 children
with SCD. Shown in (Figure 1A) is the breakdown of the different
SCD genotypes in our population; 199 patients with homozygous
hemoglobin SS disease (HbSS); double heterozygotes included 71
hemoglobin S and C (HbSC) and 28 hemoglobin Sβ+-Thalassemia
(HbSβ+-Thal). There were 4 patients each with HbSβ0-Thal or other
category (HbCC or α-Thalassemia). As shown in (Figure 1B), our
age distribution included 0-5 years (23%), 6-12 years (35%), 13-
18 years (29%) and >18 years (13%). The primary caregivers of
the patients were 66% mothers, 12% fathers, 11% grandparents,
and 9% others (Figure 1C). The P2P services was highly utilized by
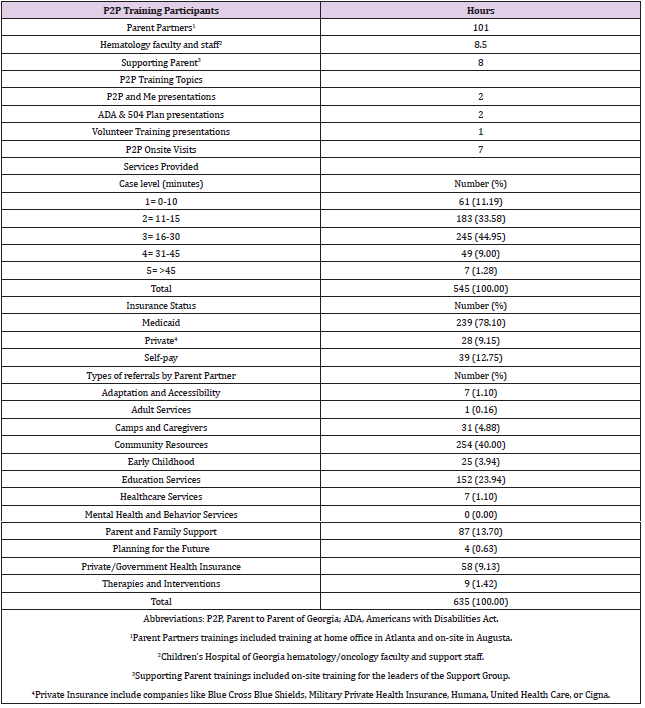
caretakers. To establish a viable P2P partnership at CHOG initial onsite
training consisting of 101 hours for Parent Partners, 8.5 hours
for hematology faculty and staff and 8 hours of parent training was
completed (Table 1). The topics covered during training included
P2P and Me, which is an overview of the programs and services
such as Special Needs Database, Roadmap to Success, Supporting
Parents, Americans with Disabilities Act, 504 Plans, among others
[3]. To introduce the program to the faculty and staff a program
description was distributed and the Parent Partner interview
occurred after medical service by the physicians in clinic.
P2P of Georgia categorize case levels by how many minutes
the Parent Partner spend with the family, gathering demographics,
social service needs, responding to the need and follow-up
interview. During the study period 545 interviews were conducted
of which 104 were follow up visits. The majority of our cases were
levels 2 and 3 requiring 15 to 30 minutes (78%) as shown in Table 1.
A few families with significant social services need required initial
interviews ~45 minutes. During the intake interview we collected
data on insurance status; the majority of families had State or
Federal Assistance program mainly Medicaid (78.1%), while 9.15%
had private insurance and 12.75% were self-pay (Table 1).
Types of Referrals Requested by Families
We identified a wide range of services requested by families as
shown in Table 1. The most common request from families included
P2P of Georgia direct contact information for Community Resources
(40%), Education Services - 504 Plans (23.94%), Parent and Family
Support (13.70%), and 9.13% requested Private/Government
Health Insurance assistance (Medicaid and SSI issues). The various
other referrals made by the Parent Partner are summarized in
Table 1.
Due to Sickle Cell Disease being a lifelong disease with no
cure as of current date, we in the Augusta University Pediatric
Comprehensive Sickle Cell Program found that the P2P program
was invaluable to the families. Most families are overwhelmed after
getting the diagnosis results that their child has Sickle Cell Disease. It
has been bought to our attention, that an understanding of parents’
reactions to a newborn infant’s diagnosis of sickle cell anemia how
they acquire knowledge can identify parent beliefs and preferences
about the process of sickle cell education [4]. With that in mind,
some families take on the fight-or-flight response. Some parents
immediately jump in and fight and do whatever it takes to take of
their child. But on the other hand, some parents fall into the flight
response. This percent just happens to be higher than we would
like. Even though we didn’t take a percentage of show rate before
this program started, we know it to be common knowledge that it
was higher than the healthcare providers/Hematologist would have
liked it. One study shows that parents of infants with SCD expressed
a high level of fear at the time of notification of a positive screen
[4]. Which brings more confirmation that P2P of Georgia services
are needed. This was alarming to the Hematologist because when
parents decide to take the flight response, there are some basic and
specialty care that this vulnerable population needs. When patients
miss out on this care, we see more Emergency Department visits,
hospital stays, and even mortality.
It is vital for parents of an infant with newly detected Sickle Cell
Disease to quickly acquire accurate health information about their
child’s condition. When parents first learn their infant has Sickle Cell
Disease, they may overcome with anxiety; accurate information can
help allay their concerns as well as motivate them to taken actions
to improve their child’s health. In particular, for Sickle Cell Anemia,
parents need to begin to learn about the importance of adhering
to recommended prophylaxis, including penicillin, vaccinations,
signs, and symptoms of acute exacerbation that require immediate
medical attention, and option for therapies such as hydroxyurea
[4]. With this pilot study with P2P of Georgia and their services, we
have seen the clinical show rates increased, families have become
more compliant, and their overall attitude has become positive.
Even though in the beginning the Parent Partners had to meet the
families where they were in their life and this is why there would be
more cases for one family. Because some families needed more help
and resources than other families. The highest percentage of cases
were needing help with State or Federal Assistance. Mainly, how to
start Medicaid and SSI applications.
Or to restart because they had been dropped for numerous
reasons. Putting these Parent Partners in place help take some of
the tension and stress out of the family’s daily life of dealing the
SCD. The Parent Partners were someone who worked between
the doctors and the families. A liaison between the families and
the many program that were in place to help and make their life
easier. Parents/caregivers most frequently reported having used
the Internet, Sickle Cell pamphlets provided by their primary care
physician, and family members as sources of health information
[4]. And in this case, what’s greater than having an accountable and
trained person to contact. The Parent Partners not only have had
several hours of training by P2P of Georgia, but they are either a
SCD patient or have a child that’s diagnosed with Sickle Cell Disease
and have accomplished great milestones. Another study revealed
that when people with chronic illness learn self-management, their
clinic outcome and quality of life improves; and they show lower
dependence on healthcare services [5]. This pilot study with P2P of
Georgia was a way to show and intervene by putting someone in the
family’s life to learn and gain skills at an early age. Before this pilot
study, there were not any identifying programs that work directly
with the families and Hematologist. One other review identifies
the important positive effects of educational interventions on improving patient’s knowledge of Sickle Cell Disease and depression
[6]. And individuals who receive higher levels of social support and
are more likely to feel as though they have the ability to perform
self-care and actually do so to maintain health [B].
With P2P of Georgia it runs very parallel, because it allows
and help both parent and child to become more independent and
learn what they should do to maintain a healthy life. We do have
to keep in mind that children with SCD becomes adults with SCD.
And to make the transition as smooth as possible we should make
sure that they also learn the skills and resources that is available to
maintain good health after transition. The Parent Partners becomes
a motivation team for both the parents and caregivers and patients.
Many studies and reviews have made it known that various types
of social support that could play a role in resiliency in children
with SCD (parents, teacher, classmate, and close friend support)
to identify the most effective subtype of social support that is
associated with resiliency in children with SCD [7]. This pilot study
has an actual person (the Parent Partner), in the clinic as a social
service support worker to work on cases and observe the inclining
of independency and compliant. Once Parent Partners helped the
families take care of the basic needs, the parents/caregivers started
asking in depth questions. This reflects in the types of referrals by
the Parent Partners (Table 1). For an example, inquiring information
about planning for the future and adult services. This happened for
two reasons. First reason, the majority of the clinic’s population
was at that time from ages 6 to 12 years. And second reason, was
because working with age group showed that they were turning 9
or 10 and the families were showing improvement on doing their
own research and showing signs of their independency.
In conclusion, with all resources being available to patients
and their families will continue to be independent and be better
equipped to deal to sickle cell disease on a day to day basics. With a
full team, we can also may sure every child has every appointment
scheduled, necessary test and scans scheduled, and the resources
needed for home. Most of the time a family is overwhelmed with the
basic information to help take care of their child. With the assistant
of a program like P2P of Georgia in a full partnership with the
Pediatric Sickle Cell Program, most families will be independent by
the time their child with Sickle Cell becomes a teenager.
First, we thank the children and families that receive care in
our program. We thank Natasha Alford, Judi Schweitzer and Ann
Sapp for administrative assistance. We acknowledge the Georgia
Department of Public Health for support of Telemedicine Program.
- Parent to Parent USA provides emotional & informational support for families of children who have special needs.
- Sickle Cell Disease.
- gadoe.org.
- Lebensburger JD, Grosse SD, Altice JL, Thierry JM, Ivankova NV (2015) Understanding and improving health education among first-time parents of infants with sickle cell anemia in Alabama: a mixed methods approach, J Pediatr Hematol Oncol 37(1): 35-42.
- Asnani MR, Quimby KR, Bennett NR, Francis DK (2016) Interventions for patients and caregivers to improve knowledge of sickle cell disease and recognition of its related complications. Cochrane Database Syst Rev 10(10): CD011175.
- Matthie N, Jenerette C, Mc Millan S (2015) Role of self-care in sickle cell disease. Pain Manag Nurs 16(3): 257-266.
- Sehlo MG, Kamfar HZ (2015) Depression and quality of life in children with sickle cell disease: the effect of social support. BMC Psychiatry 15: 78.
 Research Article
Research Article