 Research Article
Research ArticleAbstract
Background: The COVID-19 has put global health institutions on alert. Organizations such as the CDC and WHO have developed preparedness and prevention checklist of 2019-nCoV infection to be used by public and healthcare professionals. Since COVID 19 pandemic is unexpected and no country aware of it prior to outbreak, there is limited information on the overall preparations of healthcare providers in Ethiopia. Therefore, the aim of this study was to assess early healthcare professionals’ preparedness and response to COVID 19 Pandemic in Oromia regional state, Ethiopia.
Methods: The study was conducted on healthcare professionals working in public hospitals of Oromia regional state. The study was carried out by online questionnaire prepared using SurveyMonkey©. The collected data was analyzed, and One-way ANOVA was used to determine the significant differences between health professionals working in different hospitals. The statistical significance associations of variables of interest was determined at 95% confidence intervals.
Results: Healthcare professionals in the public hospitals of Oromia regional state, Ethiopia perceived that they are not yet well prepared and may not respond to the pandemic quickly and efficiently. Even though, they have positive response towards identifying signs and symptoms, provide education and utilization of PPE, they are still lacking in practical responses like managing cases, implementing emergency plans and isolation procedures from many others.
Conclusion: As the Federal Ministry of Health, Ethiopia Public health institute and Oromia health bureau are vigilant and continually conducting preventive measures programs, extensive and maximum effort should be done to improve healthcare providers’ preparedness and response towards any emergency related to COVID-19 pandemic.
Keywords: Preparedness; Response; COVID-19; Ethiopia; Oromia
Abbreviations: CDC: Communicative Disease Control Center; COVID-19: Corona Virus Disease- 19; FMoH: Federal Ministry of Health; MERS: Middle East Respiratory Syndrome; nCov: Novel Corona Virus; PPE: Personal Protective Equipment; SARS: Severe Acute Respiratory Syndrome; SPSS: Statistical Program for Social Sciences; WHO: World Health Organization
Background
The current flare-up of respiratory sickness caused by a novel
coronavirus (named “COVID-2019”) has bolted down the world and
has been recognized as a danger by US Centers for Disease Control
(CDC) and pronounced pandemic by World Wellbeing Organization
(WHO). The primary case was identified in Wuhan City, Hubei Area,
China and since at that point, the infection has spread in disturbing
rate [1]. It is one of the worldwide pandemics with colossal wellbeing,
financial and psychosocial emergencies influencing the citizens of
any countries. Coronaviruses are a huge family of encompassed
RNA infections found in a many of creatures like camels, cattle, cats,
and bats. In moderately uncommon occasions, vectors can transmit
coronaviruses to people with proceeded circulation coming about from human-to-human exposure. Examples include severe acute
respiratory syndrome coronavirus (SARS-CoV), Middle East
Respiratory Syndrome Coronavirus (MERS-CoV), COVID-2019, like
MERS-CoV, and SARS-CoV, all of them have originated in bats [2].
Taking after the WHO COVID 19 crisis affirmation, local and
national governments and universal bodies have forced public
health and social measures on people, educate and communities
to contain the illness. These measures incorporate identifying and
confining cases, contact-tracing and isolate, social and physical
separating counting mass get-togethers and travel confinements
[3]. Accordingly, in any nation, particular areas or administrations
can be the central point of the episode. In spite of the fact that
healthcare is given exterior clinics (such as crisis clinics, nursing
homes, community wellbeing centers), hospital-based experts
stay the bunch at amazingly tall chance of exposure to the diseases
and may contract or transmit it in like manner [4]. In any case,
data around the wellbeing frameworks and health professionals’
readiness for combating the 2019-nCoV isn’t known. Subsequently,
their mindfulness and readiness in overseeing the 2019-nCoV
contamination are vital to prevent the further spread of the
disease. Our study will be conducted to assess the preparedness
of healthcare personnel against the 2019-nCoV outbreak and how
well they respond in an outbreak [5].
Healthcare workers are extremely exposed to the
contaminations, more than any other people, as they are in contact
with the infected people. Particularly, amid any flare-up, they may
have to be work with a healthcare team [6] as their response to
manage novel Corona infection which may put them under the most
elevated chance of contracting the virus. Their behavior, mental
set up and material readiness in overseeing the responding to the
COVID-19 is exceptionally vital to avoid spread of this amazingly
communicable illness [7]. The readiness includes from fabric
accessibility such as sufficient N-95 masks for health care staff
and its use according to its guidance to mental readiness to supply
fundamental administrations without any fear [8-11].
Since COVID 19 pandemic is unexpected and no country aware
of it prior to outbreak, there is limited or no studies and surveys all
over the world and it is extremely lacking in Ethiopia. Consequently,
the preparedness and awareness level of health care providers in
Oromia regional state is unknown. Therefore, this study assessed
healthcare professionals’ preparedness and response towards
COVID 19 Pandemic in the region. The finding helps to understand
how healthcare professionals’ readiness to protect themselves and
contain the pandemic.
Methods and Material
Study Setting and Design
This study was conducted in Oromia National regional state public hospitals. Oromia region is one of nine constitutionally established states and largest and populous of all. There are 82 functional public hospitals in the region of which 44 are primary hospitals and 34 are general hospitals and 4 are comprehensive specialized hospitals. During the survey, a cumulative of 273 anesthesia professionals, 213 biomedical engineers,4051 Health Officers, 1391 medical doctors, 193 specialists, 19 public health specialists, 2359 laboratory technologists, 4632 midwifery professionals, 15401 Nurse professionals, 2664 pharmacy professionals, and 997 environmental health professionals were serving in those hospitals. Data was collected from April 01 to April 30, 2020 G.C and cross-sectional study design was employed [12].
Study Population, Sample Size and Sampling Technique
All health care workers in Oromia region’s Public hospitals were included as study population. The survey was conducted in all functional public hospitals in Oromia Regional state, Ethiopia. There was no restriction on the number of participants per hospital and convenient sampling technique was used. All Healthcare providers in the hospitals including physicians, nurses, pharmacists, and others were included. We enrolled staff members who are or were handling suspected cases in settings in their respective hospitals [13,14].
Data Collection Tool
The study was carried out using a structured questionnaire adapted from the CDC checklist and the previous questionnaire on the recent outbreak. The questionnaire included different types of questions in the questionnaire including (Yes/No) questions, open-ended questions, and multiple-choice questions as well. The original questionnaire was developed in English and the study team collaborators at hospital level were responsible support for its translation into Afan Oromo when there was need. To gather information about the health care provider’s preparedness in the participants’ hospitals, we developed an online questionnaire using SurveyMonkey© that limits one-time participation per unique IP address and the link was sent to participants via Email, Telegram, WhatsApp, Facebook and LinkedIn for easy accessibility [15].
Data Analysis and Management
The collected data was organized by Google Sheets and collected in an Excel spreadsheet. The survey was completely anonymous. Only the study team had access to all data. Data entered into Google Sheets were quality-checked by to ensure accuracy. The statistical computer package, IBM SPSS, Version 22 was used to perform quantitative analysis on the collected data. In order to perform analysis of data, it was necessary to code the response variables, i.e., yes = 1, no = 0. Data cleaning were carried out throughout the data entry process. The analysis of the data was performed through descriptive statistics, such as frequencies for each of the variables. One-way ANOVA was used to determine the significant differences of each variable between the groups. The threshold for statistical significance was p≤0.05 [16].
Results
A total of 340 healthcare professionals completed the survey, more than 72% of the respondents were male. The majority of the respondents were in the age range between 21 and 30 years. In terms of experience, 80.8% of the respondents had up to 5 years during the study period. Concerning their profession, majority were physicians 120(35.29%) followed by nurses 90(26.47%) and majority of them 160(48.48%) are working in primary hospital (Table 1).
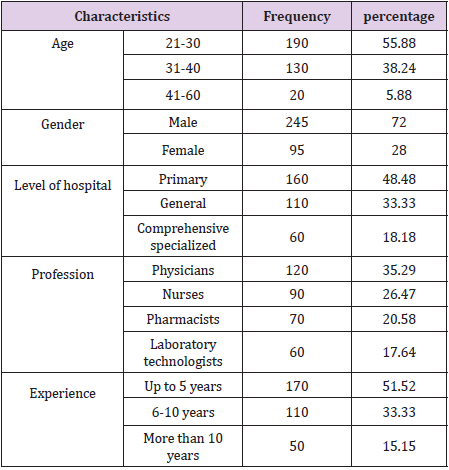
Table 1: Usociodemographic details of the respondents.
Table 2 presented the health care professionals’ preparedness
towards COVI-19 Pandemic. The mean scores were obtained by
calculating the total response for each item in the questionnaire
and the total sample participated in each category. The data showed
that most of the respondents were not prepared for the COVID-19
Pandemic. There were significant differences between healthcare
professionals on most of the items asked in the questionnaire.
Pharmacists felt they have no sufficient information about
COVID-19 preparedness [0.46(±0.35)], didn’t aware for guidelines
and recommendations from WHO and FMoH [0.27(±0.39)], were
not reading journals and articles about COVID-19 [0.44 (±0.15)],
felt that there is low support from local officials during emergency
situation. The nurses found it difficult to access educational ways
about COVID-19 management [0.46 (±0.35)], low support from
local officials [0.27(±0.39)], didn’t know who to contact during
emergency [0.44(±0.15)], difficult to get update and literatures
about COVID-19 [0.40 (±0.23)], low participation in educational
practices about COVID-19 [0.43 (±0.33)], low participation during
planning [0.43(±0.33)], low understanding about history taking
[0.43 (±0.28), not familiar with local emergency response system
[0.36 (±0.18)] and most of them didn’t consider themselves ready
for management of COVID-19 [0.43 (±0.24)] [17].
Laboratory technologists felt low understanding about
obstacles regarding COVID-19 preparedness [0.30 (±0.31)],
challenging to access educational ways about COVID-19 [0.48
(±0.11)], insufficient awareness about recommendations from
WHO and FMoH [0.42(±0.28)], most of them didn’t read journals
and articles about COVID-19 [0.42 (±0.23)], felt low support from
local officials [0.39 (±0.34)], didn’t know who to contact when got
emergency [0.45 (±0.31)], not familiar with triage system [0.30
(±0.31)], didn’t know isolation procedures [0.48 (±0.11)], not
familiar with local emergency response system [0.42 (±0.28)] and
most of them didn’t consider themselves ready for management
of COVID-19 [0.43 (±0.24)]. Physicians felt low support from local
officials [0.30(±0.31)], didn’t know who to contact in emergency
situation [0.48 (±0.11)], didn’t participate in educational activities
about COVID-19 pandemic [0.42 (±0.23)], most of them didn’t
participate in planning [0.39 (±0.34)], and were not familiar with
local response system [0.39 (±0.26)] (Table 2).
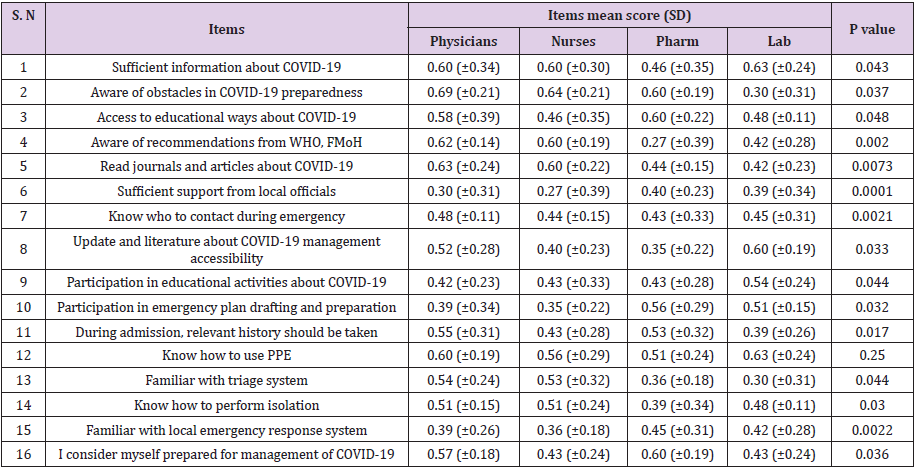
Table 2: Preparedness of health care professional towards COVID-19 Pandemic.
Table 3 reveals that the health care professionals’ perceived responses to the COVID-19 Pandemic. The data showed that most of the respondents perceived positive responses towards Confidence in providing patient education, ability to identify sign and symptoms of COVID-19 and readiness to participate in peer evaluation skills on COVID-19. However, most of them perceived negative towards other items like ability to care for COVID-19 patient without supervision, managing the common symptoms and reactions of COVID-19, and confidence in implementing emergency plan, and isolation procedure Yet, there were significant differences found between health care professionals’ perceived response towards COVID-19 on some of the items asked in the questionnaire. Nurses [0.46(±0.35)] and laboratory technologists [0.48 (±0.11)] were not sure of their scope in their role against COVID-19, and physicians perceived positive to most of items included in the questionnaire with highest mean scores for those statements (Table 3).
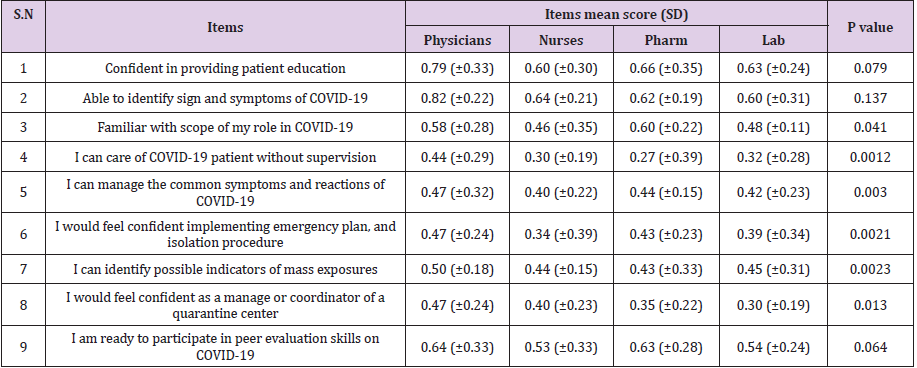
Table 3: perceived response of health care professionals towards COVID-19 pandemic.
Discussion
The COVID-19 outbreak, which was first detected in Wuhan,
China, in December 2019, has been evolving rapidly. On 30 January
2020, the WHO Director-General declared that the current outbreak
constituted a public health emergency of international concern, and
on 12 March 2020 the COVID-19 outbreak was declared a pandemic
[3]. Ethiopia has been doing widespread efforts in containing this
pandemic, whose cases are increasing slowly but the worst is
feared in coming weeks or months, as pattern of COVID-19 effect
being observed in many countries [18]. For this purpose, extensive
media and physical campaigns about preventive mechanisms of the
disease, increasing number of functional laboratories to test for the
infection, tracing contacts, and others are being undergone.
Federal ministry of health and Ethiopian public health institute
released a checklist to check for preparedness and response of
health facilities in the country and little is included about the health
care providers in that specific document [18]. Therefore, the status
of preparedness and perceived response of health professionals
in the country is largely unknown and this study, with its own
limitations, revealed the current readiness of health professionals
in Oromia regional state, Ethiopia. Regarding the sociodemographic
data of study participants, majority of them were male: and it
may be due to presence of more male work forces in medical and
health sector in the country due to low number of females in the
profession. And most of them were in age range of 21-30 and this
may be due to more social media utilization by this age group and
also it can be because Ethiopian population is young making the
public servants fall in young age group [19].
According to result of this online survey, healthcare
professionals in Oromia public hospitals are not prepared for a
COVID-19 infection outbreak and they had difficulty in accessing
the research literature, felt they have no sufficient information
about COVID-19 preparedness, didn’t aware for guidelines and
recommendations from WHO and FMoH, were not reading journals
and articles about COVID-19 which shows that either they were too busy with patients or they must have limited access to literatures.
They also felt that there is low support from local officials during
emergency situation which may be poor communication and
collaboration between different stakeholders.
Handful of respondents were also not sure who to contact
during emergency situation which may be due to absence or
functionality of reporting channels. Majority of participants didn’t
participate in educational activities about COVID-19 pandemic and
this can be also due to absence of such educational opportunities
or professionals busy time to take such activities seriously. Most of
them didn’t participate in emergency planning ad it may be because
of perceiving planning something administrative and not their scope
and were not familiar with local response system which can be due
to absence of stressful outbreaks in their community recently. Our
findings, therefore, advocate that existing systems of preparedness
and response to of COVID-19 Pandemic may not be an effective way
to reach, prepare and convince health care providers, which would
otherwise not respond to this pandemic timely and effectively.
Healthcare professionals perceived a positive response towards
some of items included in the questionnaire like Confidence in
providing patient education, ability to identify sign and symptoms
of COVID-19 and readiness to participate in peer evaluation skills
on COVID-19. Tis may be due to extensive media campaign on sign,
symptoms and prevention methods of COVID-19 pandemic so
that respondents could easily know it and be confident to provide
education. However, most of them perceived negative towards
ability to care for COVID-19 patient without supervision, managing
the common symptoms and reactions of COVID-19, and confidence
in implementing emergency plan, and isolation procedure of
COVID-19 which indicates low behavioral and psychological
preparedness due to fear from reports from other countries
regarding the disease and professionals’ eminent exposure and
absence of much real experiences about COVID 19 outbreak.
The total mean score for preparedness and responses to
COVID-19 was negative among the health care professionals,
although there was a range of variance in scores. Probable reasons
may be the fact that the preparedness and response program
have not been comprehensive. There may be behavioral, social
and psychological factors which should be assessed in addition to
absence of compulsory trainings, sufficient modules, documents
and guidelines available for all at all levels including remote areas,
friendly relationship with local authorities, functional and effective
communication in the health system and so on [18]. Therefore,
health care providers should be ready for response to COVID-19
pandemic by materials, behavior and psychology as recommended
by international and national health institutions [20]. Every
responsible bodies, governmental and/or non-governmental,
should work hand in hand to avert this problem by equipping
health care providers in all dimensions to help them respond to the
pandemic quickly, effectively and successfully.
Conclusion
Healthcare professionals in the public hospitals of Oromia regional state, Ethiopia perceived that they are not yet well prepared and may not respond to the pandemic quickly and efficiently. Even though, they have positive response towards identifying signs and symptoms, provide education and utilization of PPE, they are still lacking in practical responses like managing cases. As the Federal Ministry of Health, Ethiopia Public health institute and Oromia health bureau are vigilant and continually conducting preventive measures programs, extensive and maximum effort should be done to improve their preparedness and response towards any emergency related to COVID-19 pandemic.
Limitation
This survey was carried out via online and didn’t represent many of health care providers who didn’t appear and access the questionnaire during study period. It also analyzed responses of only four groups of health professionals due to few responses from other professional groups. This study also didn’t show preparedness and response of health professionals working frontline at health centers, private clinics and hospitals.
References
- Singhal T (2020) A review of coronavirus disease-2019 (COVID-19). The Indian Journal of Pediatrics 87(10223): 1-6.
- Lu R, Zhao X, Li J, Niu P, Yang B, et al. (2020) Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. The Lancet 395(10224): 565-574.
- World Health Organization (WHO) (2020) Coronavirus disease 2019 (COVID-19): situation report 72.
- Wang C, Horby PW, Hayden FG, Gao GF (2020) A novel coronavirus outbreak of global health concern. The Lancet 395(10223): 470-473.
- Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Eng J Med 382(8): 727-733.
- Paules CI, HD Marston, AS Fauci (2020) Coronavirus infections—more than just the common cold. Jama 323(8): 707-708.
- Chan JFW, Yuan S, Kok KH, Wang To KK, Chu H, et al. (2020) A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. The Lancet 395(10223): 514-523.
- Hays JN (2005) Epidemics and pandemics: their impacts on human history.
- Yu SH, Wang LT, SzuTu WJ, Huang LC, Shen CC, et al. (2020) The caregivers’ dilemma: Care burden, rejection, and caregiving behaviors among the caregivers of patients with depressive disorders. Psychiatry Research 287: 112916.
- Emanuel EJ, Persad G, Upshur R, Thome B, Parker M, et al. (2020) Fair allocation of scarce medical resources in the time of Covid-19. Mass Medical Soc 382: 2049-2055.
- Kapata N, Ihekweazu C, Ntoumi F, Raji T, Kapata PC, et al. (2020) Is Africa prepared for tackling the COVID-19 (SARS-CoV-2) epidemic. Lessons from past outbreaks, ongoing pan-African public health efforts, and implications for the future. International Journal of Infectious Diseases 93: 233-236.
- Davies SE, B Bennett (2016) A gendered human rights analysis of Ebola and Zika: locating gender in global health emergencies. International Affairs 92(5): 1041-1060.
- Alon T, Doepke M, Rumsey JO, Tertilt M (2020) The impact of COVID-19 on gender equality. National Bureau of Economic Research.
- Cross P (2020) Impact of COVID-19 policies on jobs much more terrible than forecast and bound to get worse.
- Kitenge SY (2020) Globalization and the COVID-19 Pandemic: How is Africa’s Economy Impacted?
- (2020) FMOH, Ethiopia, COVID 19 response. 2020: Addis Ababa.
- (2020) CDC, Preparedness Tools for Healthcare Professionals and Facilities Responding to Coronavirus (COVID-19).
- Lovibond LP (1995) Manual for the Depression Anxiety Stress Scales. 2d ed. Sydney: Psychology Foundation of Australia.
- (1999) Central Statitical Auhority. Ethiopian National Census, Addis Ababa, Ethiopia.
- Gilbert M, Pullano G, Pinotti F, Valdano E, Poletto C, et al. (2020) Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. The Lancet 395(10227): 871-877.
