 Mini Review
Mini ReviewAbstract
Schwannomas or neurilemmomas are the most common tumors of the peripheral nerves. In this article, the characteristic appearances of schwannoma on high-resolution ultrasonography (US) and magnetic resonance imaging (MRI) were currently reviewed. The author previously mentioned that schwannomas were painful and vascularized superficial tumors of the acronym “ENGLAND” or ”LEND AN EGG”. From a current knowledge, the distinction between Antoni A-dominant and Antoni B-dominant types was suggested on high-resolution US. Antoni A-dominant schwannomas may tend to be a small size on gray-scale US and moderate vascular flow on color Doppler US. While, it is putative that the Antoni B-dominant schwannomas may represent relatively large tumor associated with anechoic lesion reflecting necrosis and/or hemorrhage on gray-scale US and a few vascularity on color Doppler US. It is strongly suggested that when target sign was recognized on MRI, the lesion may be an origin from nerve sheath and benign type.
Keywords: High-Resolution Ultrasound; MRI; Antoni A-Dominant Schwannoma; Antoni B-Dominant Schwannoma; Target Sign
Introduction
Schwannomas or neurilemmomas are the most common tumors of the peripheral nerves [1,2] It has been well known that schwannomas are one of a painful tumors of the skin [3]. The author has previously described the study on schwannomas as the painful cutaneous and subcutaneous tumors accompanied with vascularized appearances using high-resolution ultrasound in dermatology: the acronym “ENGLAND” or “LEND AN EGG” [4]. The author has also mentioned that it is important to differentiate between schwannoma and angioleiomyoma (ALM) [5,6]. It has been suggested that nerve-tumor associations such as nerve-tumor position and neve-tumor transition are significant features to differentiate schwannoma from neuroma [7,8]. Recently, Yang et al. [2] described that the target sign is a prominent feature on highresolution US in peripheral schwannoma. In this article, the current knowledge of the characteristic appearances of schwannoma on high-resolution US and MRI will be reviewed.
Ultrasound in Dermatology
In dermatology, a 15 MHz is the minimum frequency recommended for performing dermatologic examination by the international working group or DERMUS (Dermatologic Ultrasound) [9,10]. Recently, Yang et al. [2] described that the target sign is a prominent feature on US in peripheral schwannoma. The author usually performs US studies for dermatologic fields with a high-resolution, broad-band (5MHz-18MHz) linear transducer (Nobulus Hitachi, Ltd. Tokyo, Japan) and described several studies including schwannoma [4-6,11-22].
Peripheral Schwannoma
Schwannomas, neurofibromas, traumatic neuromas, Morton neuromas, neural fibrolipomas, and nerve sheath ganglion cysts are benign neurogenic tumors affecting the musculoskeletal system [1]. Two major groups of the solitary benign peripheral nerve sheath tumors are regarded as schwannomas (neurilemmomas) and neurofibromas [23]. Schwannomas originate from the Schwann cells and usually well encapsulated without invading the nerves [24]. Clinically, schwannomas may be tender and firm and have a flash- to pale-pink color [3,4]. Pathologically, S-shaped nuclei and Verocay bodies are characteristic appearances. Both Antoni A and Antoni B tissue may be also observed [3,4].
Gray-scale US Appearances
Nerve-Tumor Association: Differentiation between schwannomas and neurofibromas is known to be difficult based on the US features representing well-demarcated margin, a round to oval shape, a homogeneous hypoechoic pattern, through transmission and internal vascularity, the presence of the entering and exiting nerve, and the target sign [8]. Some studies have shown nerve-tumor connection in schwannoma [25-28]. Reynold et al. [25] have described that the presence of intrinsic blood flow signal on color Doppler US and nerve continuity features on grayscale suggest the peripheral nerve sheath tumor. Tsai et al. [7] described that a nerve eccentrically entering a mass was shown in schwannomas. With respect to the features of nerve-tumor position, Ryu et al.[8] proposed that schwannoma can show both eccentric and central positions, whereas an eccentric position can exclude the possibility of neurofibroma. Concerning the appearances of nerve-tumor transition, they mentioned that schwannoma can be clearly defined and neurofibroma shows infiltrative [8].
Target Sign: Several studies of schwannomas show homogeneously hypoechoic mass on gray-scale US. Reynold et al. [25] have reported the US target sign representing hyperechoic center and hypoechoic periphery in schwannoma. Recently, Yang et al. [2] described that the target sign is a prominent feature on US in peripheral schwannoma. They described that the US target sign was defined as the presence of a cluster, cloud, or target-shaped hyperechoic area in the center of the tumor, with the peripheral region representing more than 1mm thick at its thickest point, of the tumor being hypoechoic compared with the adjacent muscle. Pathologically, a schwannoma typically consisted of a highly cellular Antoni A area and a hypocellular myxoid Antoni B area. It has been reported that the target sign is consistent with the presence of hypercellular Antoni A areas in central and myxoid Antoni B areas in periphery. Yang et al. [2] suggested that schwannoma with multiple cystic lesions are often occupied by Antoni B areas, whereas small schwannomas are almost exclusively composed of Antoni A areas. While, it has been described that the large schwannomas showed hyperechoic calcifications, internal degenerative cystic foci, and increased internal hierarchic vascular architecture [26,29].
Color Doppler Appearances
The nerve-tumor associations such as nerve-tumor position and/or nerve-tumor transition and vascularity of the tumors could be useful for the differentiation between schwannoma and neuroma. Ryu et al. [8] noted that schwannoma represents eccentric nerve-tumor position on gray-scale US and vascularity within the tumor on color Doppler US. The report by Tsai et al. [7] showed that hypervascular flow signals were depicted in schwannoma on color Doppler US. Although the variable vascularity status has been described, most schwannoma were more vascular than neurofibromas [8]. It has been noted that Antoni A-dominant schwannoma may represent high blood flow signals, whereas Antoni B-dominant schwannoma may not show. A pathologically confirmed schwannoma in the thigh in a 47-year-old male was represented in Figure 1 and 2. A large well-defined hypoechoic nodule measuring 25 mm in diameter accompanied with cystic change and eccentric nerve-tumor position were depicted on grayscale US. A few blood flow signals were detected on color Doppler US (Figure 1). Pathologically, well-defined ovoid mass associated with degenerative cystic foci and less cellular Antoni type B area consisting of neuronal spindle cells forming Verocay bodies was observed (Figure 2). An Antoni B-dominant schwannoma represents a large tumor with cystic change on gray-scale US and a few flow signals on color Doppler US.
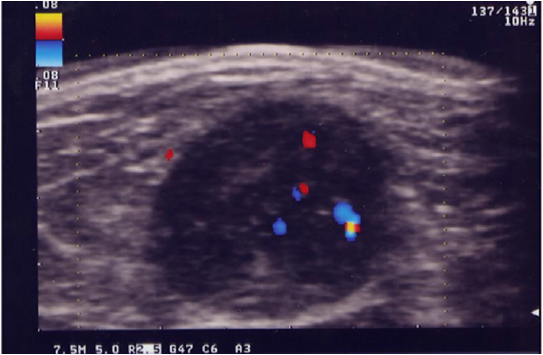
Figure 1: Antoni B-dominant schwannoma in the thigh in a 47-year-old male. A well-defined hypoechoic nodule accompanied with cystic change and eccentric nerve-tumor position was depicted on gray-scale US. Little blood flow signals were observed on color Doppler US.
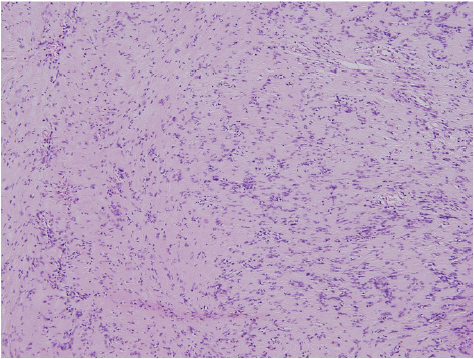
Figure 2: Photomicrograph showed a well-defined ovoid mass associated with degenerative cystic foci and less cellular Antony type B area consisting of neuronal spindle cells forming Verocay bodies (hematoxylin and eosin, original magnification x100).
MRI Appearances
Peripheral nerve sheath tumor (PNST) shows isointense signal intensity (SI) with muscle on T1-weighted image (TIWI) and heterogeneously hyperintense SI than muscle on T2-weighted image (T2WI), and heterogeneous enhancement pattern have been reported in patients with major-nerve PNST [30]. Five classical MRI features including the split-fat sign, target sign, fascicular pattern, entering and exiting nerve, and a thin hyperintense rim have been well known [30-33]. It has been suggested that the target sign was classified when the central hypointense focus comprised less than three-quarters of the lesion’s diameter with a peripheral hyperintense rim on T2-weighted images [30,32]. On histological examination, schwannomas represent a target sign due to a hypercellular, hyporintense center or Antoni A area and a hypocellular periphery rich in marcrophages and collagen fibers or Antoni B area [32,34,35]. The target sign on MRI may suggest not only the tissue of origin from nerve sheath but also typical benign type [32,34]. The previous study indicated the qualitative presence and apparent increased conspicuity of the target sign on apparent diffusion coefficient (ADC) mapping in PNSTs [36]. Ahlawat et al. [34] have studied to evaluate the utility of target sign on diffusion weighted imaging (DWI) and ADC mapping for PNST findings. They concluded that a “target sign” suggests a benign PNST and is more often visible on DWI and ADC maps compared with anatomic sequences [34].
Conclusion
1. The author previously described schwannomas as a painful and vascularized superficial tumor. In addition, the differences of vascular status between Antoni A-dominant and Antoni B-dominant types may be suggested on color Doppler ultrasonography.
2. Antoni A-dominant schwannomas may tend to be a small size on gray-scale ultrasonography and moderate vascular flow on color Doppler ultrasonography.
3. It is putative that Antoni B-dominant schwannomas may represent relatively large tumor associated with anechoic lesion reflecting necrosis and/or hemorrhage on gray-scale US and a few vascularity on color Doppler ultrasonography.
4. It is strongly suggested that when target sign was represented on magnetic resonance imaging, the lesion may be an origin from nerve sheath and benign type.
Acknowledgement
The author appreciates Dr. Akira Fujioka, Dr. Minoru Oishi, Dr. Hikaru Eto, and Dr. Masahiro Okada for their kind support.
References
- Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT, et al. (1999) From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. RradioGraphics 19(5): 1253-1280.
- Yang F, Chen XX, Wu HL, Zhu JF, Chen Y, et al. (2017) Sonographic features and diagnosis of peripheral schwannomas. J Clin Ultrasound 45(3): 127-133.
- Naversen DN, Trask DM, Watson FH, Burket JM (1993) Painful tumors of the skin: “LEND AN EGG” J Am Acad Dermatol 28: 298-300.
- Fujioka K (2019) Painful cutaneous and subcutaneous tumors accompanied with vascularized appearance using high-resolution ultrasound in dermatology: the acronym “ENGLAND” or “LEND AN EGG”. Biomed I Sci & Tech Res 12(4).
- Fujioka K, Fujioka A, Oishi M, Hayashi K, Nakayama T, et al. (2018) High-resolution ultrasound imaging for angioleiomyoma: a painful and vascularized superficial tumor. Biomed J Sci & Tech Res 9(5).
- Fujioka K (2020) Subtypes of subcutaneous angioleiomyoma on high-resolution color Doppler ultrasonography along with MRI appearances. Biomed J Sci & Tech Res 31(1).
- Tsai WC, Chiou HJ, Chou YH, Wang HK, Chiou SY, et al. (2008) Differentiation between schwannomas and neurofibromas in the extremities and superficial body: the role of high-resolution and color Doppler ultrasonography. J Ultrasound Med 27: 161-166.
- Ryu JA, Lee SH, Cha EY, Kim TY, Kim SM, et al. (2015) Sonographic differentiation between schwannomas and neurofibromas in the musculoskeletal system. J Ultrasound Med 34(12): 2253-2260.
- Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Martorell A, et al. (2016) Guidelines for performing dermatologic ultrasound examinations by the DERMUS group. J Ultrasound Med 35(3): 577-580.
- Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Martorell A, et al. (2016) Proposal for an assessment training program in dermatologic ultrasound by the DERMUS group. J Ultrasound Med 35: 2305-2309.
- Fujioka K, Fujioka A, Eto H, Suzuki K, Sanuki E, et al. (2006) Nodular fascitis in the thigh followed up using ultrasonography. J Med Ultrason 33(1): 49-53.
- Fujioka K, Fujioka A, Oishi M, Eto H, Tajima S, et al. (2017) Ultrasonography findings of intradermal nodular fasciitis: a rare case report and review of the literature. Clin Exp Dermatol 42(3):335-336.
- Fujioka K, Fujioka A, Tajima S, Oishi M, Hayashi K, et al. (2018) Characteristic power Doppler sonographic imaging of nodular fasciitis from a dermatological perspective: another case and review of three cases. J Clin Case Rep 8: 9.
- Fujioka K (2018) Presentations of clinical, ultrasonographic and pathological features of nodular fasciitis from an established cytogenetic viewpoint: review of the case series. J Carcinog Mutagen 9: 326.
- Kazumi Fujioka (2018) Usefulness of comprehensive high-resolution ultrasound imaging in dermatologic field: epidermal cyst. Biomed J Sci & Tech Res 12(1).
- Fujioka K (2019) Real- time Tissue elastography in epidermal cyst: along with enhanced MRI and elasticity features of peripheral rim. Biomed J Sci & Tech Res 16(5).
- Fujioka K (2019) A comparison between superficial and deep-seated lipomas on high-resolution ultrasonography: with RTE and MRI appearances. Biomed J Sci & Tech Res 19(2) .2019. BJSTR. MS.ID.003278.
- Fujioka K (2019) Characteristic appearances of nodular fasciitis on high-resolution ultrasonography: with vasculature status from a lesion-located perspective. Biomed J Sci & Tech Res 20(4) .2019. BJSTR. MS.ID.003490.
- Fujioka K. Fujioka A, Oishi M, Okada M (2019) A new application in dermatological ultrasound. Biomed J Sci & Tech Res 22(5) .2019. BJSTR. MS.ID.003809.
- Fujioka K. Fujioka A, Okada M (2019) Utility of high-resolution ultrasonography by using acoustic coupler in dermatology. Biomed J Sci & Tech Res 23(5) .2019. BJSTR. MS.ID.003953.
- Fujioka K. Fujioka A, Okada M (2020) High-resolition ultrasonographic appearances in superficial fibromatoses: palmar and plantar diseases. Biomed J Sci & Tech Res 27(2)-2020. BJSTR. MS. ID. 004462.
- Fujioka K (2020) Relationship between high-resolution ultrasonographic and pathological appearanes in epidermal cyst: an image representation of the plantar type. Journal of Clinical Case Reports Online 1(1) :1004.
- Beaman FD, Kransdorf MJ, Menke DM (2004) Schwannoma: radiologic-pathologic correlation. RadioGrapphics 24(5): 1477-1481.
- King AD, Ahuja AT, King W, Metreweli C (1997) Sonography of peripheral nerve tumors of the neck. AJR Am J Roentgenol. 169: 1695-1698.
- Reynolds DL Jr, Jacobson JA, Inampudi P, Jamadar DA, Ebrahim FS, et al. (2004) Sonographic characteristics of peripheral nerve sheath tumors. AJR Am J Roentgenol 182: 741-744.
- Jin W, Kim GY, Park SY, Chun YS, Nam DH, et al. (2010) The spectrum of vascularized superficial soft-tissue tumors on sonography with a histopathologic correlation: part 1, benign tumors. AJR Am J Roentgenol 195: 439-445.
- Carra BJ, Bui-Mansfield LT, O’Brien SD, Chen DC (2014) Sonography of musculoskeletal soft-tissue masses: techniques, pearls, and pitfalls. AJR Am J Roentgenol 202: 1281-1290.
- Stuart RM, Koh ESC, Breidahl WH (2004) Sonography of peripheral nerve pathology. AJR Am J Roentgenol 182(1): 123-129.
- Gruber H, Glodny B, Bendix N, Tzankov A, Peer S, et al. (2007) High-resolution ultrasound of peripheral neurogenic tumors. Eur Radiol 17: 2880-2888.
- Lee SK, Kim JY, Jeong HS (2020) Benign peripheral nerve sheath tumor of digit versus major-nerve: comparison of MRI findings. PLoS One: 15(3): e0230816.
- Chee DWY, Peh WCG, Shek TWH (2011) Pictorial essay: imaging of peripheral nerve sheath tumors. Can Assoc Radiol J 62(3): 176-182.
- Jee WH, Oh SN, McCauley T, Ryu KN, Suh JS, et al. (2004) Extraaxial neurofibromas versus neurilemmomas: discrimination with MRI. AJR Am J Roentgenol 183(3): 629-633.
- Abreu E, Aubert S, Wavreille G, Gheno R, Canella C, et al. (2013) Peripheral tumor and tumor-like neurogenic lesions. Eur J Radiol 82(1): 38-50.
- Ahlawat S, Fayad LM (2018) Imaging cellularity in benign and malignant peripheral nerve sheath tumors: utility of the “target sign” by diffusion weighted imaging. Eur J Radiol 102: 195-201.
- Rodriguez FJ, Folpe AL, Giannini C, Perry A (2012) Pathology of peripheral nerve sheath tumors: diagnostic overview and update on selected diagnostic problems. Acta Neuropathol 123: 295-319.
- Ahlawat S, Baig A, Blakeley JO, Jacobs MA, Fayad LM, et al. (2016) Multiparametric whole-body anatomic, functional, ans metabolic imaging characteristics of peripheral lesions in patients with schwannomatosis. J Magn Reson Imaging 44(4): 794-803.
