 Mini Review
Mini ReviewAbstract
“Music gives a soul to the universe, wings to the mind, flight to the imagination and life to everything” said Plato the great philosopher. In the current time of COVID-19 pandemic encompassing the world, music has lost its stage and has become confined to the virtual sphere. Though many of its connoisseurs are eagerly waiting for musical performances to resume, it poses a greater threat of creating an infection cluster through virus particles emitted from a possibly infected singer. Various experiments have estimated particle emission rates by performers during vocalization activities. Simulations have also measured time course of emitted particles in a closed environment leading to the infection spread. In this mini review we attempt to compile and interpret available information and assess that possible impact a musical performance can play in spreading the infection.
Introduction
COVID-19 disease caused due to infection by a novel form of
beta coronavirus designated as nCov-2019 or SARS-CoV-2 has
brought the world to its knees in the last 7-8 months severely
affecting activities in all spheres of life. High infectivity of the
virus has forced governments world-wide to lay embargo on mass
gatherings which has impacted the social, religious, cultural and
sports lives of humanity. For the musically inclined people this has
taken a devastating effect as all forms of live concerts, choir and
singing performances have come under the ban, forcing music to be
confined to the online world only. Music performances as nucleus
of a COVID-19 infection storm came into highlight from a cluster
of 100+ affected individuals who attended a number of live music
events between February and April 2020 in Osaka, Japan. Rigorous
contact tracing was able to pinpoint source of these infections to a
single individual with symptoms who participated in many of the
events [1,2].
Spread of infections was reported not only amongst audience
of music concert, but also between members of a choir in Skagit
county, Washington who seemed to have passed on the virus to
each other over a couple of practice sessions [3]. However, it is
not clear whether the activity of singing in confined area or just
social interaction between members was the prime contributor in
spreading infection. It is now quite well-known that SARS-CoV-2
primarily infects human through the respiratory epithelial cells.
Spike proteins on the virion surface binds to the Angiotensin-
Converting Enzyme 2 (ACE2) receptor of cells to force its entry and
start the pathogenesis process through replication by fooling the
host genome. Virus particles are typically transmitted from infected
persons as droplets in air or fomites on various surfaces that
commonly come in human contact. Thus, to assess the potential of
music performance or singing in particular as a key mechanism for
spread of COVID-19, it will be important to understand formation
of the droplets during vocal activities.
Impact of COVID-19 on singing was reviewed in detail by
Naunheim and co-workers [4] mostly in qualitative terms. As
pointed out in this review, phonation during talking and singing
generates larger quantities of droplets and aerosol. In the
background of a large number of asymptomatic COVID-19 positive
patients worldwide, such vocal activities may have the potential
to nucleate large clusters of infection. In this mini-review, we aim
to gather available quantitative information on droplet generation
during vocal activities and assess their potential in spreading
COVID-19.
Generation of Infective Particles from Respiratory Tract
Droplet and Aerosol Generation
Droplets emerging through nose and mouth during breath, speech or other vocal activities can be traced to three anatomic components as their source - bronchiolar fluid film in the lungs, trachea and larynx and the oral cavity (Figure 1). Mechanisms of droplet generation from each of these body parts and their further spread, extensively reviewed by Wei & Li [5] are summarized in (Table 1). Extensive studies on respiratory droplets generated through pre-set inhale-exhale patterns revealed largest droplet size < 2 μm [6]. Though such droplets have possibility of aerosol formation, their sub-micron size restrict them to contain very few SARS-CoV-2 virions that are of ~ 0.1 μm diameter itself [7]. On the other hand, large millimetre-sized droplets generated from oral cavity have limited potential of airborne spread since their large size causes deposition within short distances due to gravitational domination.
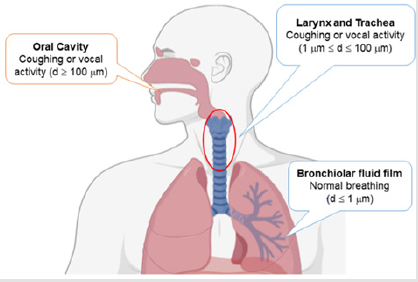
Figure 1: Sources of droplet generation in human respiratory system.
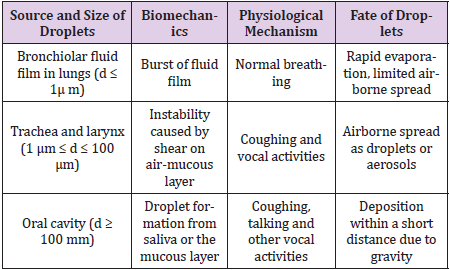
Table 1: Source and characteristics of respiratory droplets.
Intermediate size droplets typically formed at rear of oral cavity are the most likely culprits for airborne spread since they can pack a larger quantity of virions and at the same time are less susceptible to gravitational pull. Experiments done with voluntary coughing of subjects from different age groups have shown droplets sizes in the range of 5-10 μm with a concentration of ~ 1000 droplets/cm3 and mean flow rates 0.1 – 0.9 L/s [8] leading to emission rates of 105- 106 droplets/s. With an initial release velocity of around 8.5 m/s [9], a cough can generate a shower of 10 -100 million of virions within a few meters of radius.
Droplet Formation Through Vocal Activities
Though coughing and sneezing can generate high load of
virus-carrying particles, such conditions are mostly applicable for
patients with symptoms, who under the present circumstances
will either be in isolation or equipped with face mask or other
protective gears. Meanwhile vocal activities including speech and
singing by infected but asymptomatic individuals are likely to pose
greater threat of airborne spread in public spaces.
In a recent but pre-COVID-19 era research, Asadi et al. [10].
studied emission of droplets by making a set of volunteers to
pronounce /ɑ/ (the vowel sound in ‘saw’) or to read an English text
at varying amplitudes. This study was an important landmark as its
results indicated – (i) the particle emission rate is linearly correlated
with amplitude of vocalization, but (ii) particle size distribution is
independent of amplitude. In the specific context of singing, another
study [11] measured particle emissions for a cohort of 12 singers
that included both professional opera singers and amateurs who
performed a 2-minute item of various categories including talking,
soft singing, loud singing, and singing with exaggerated diction or
at high pitch.
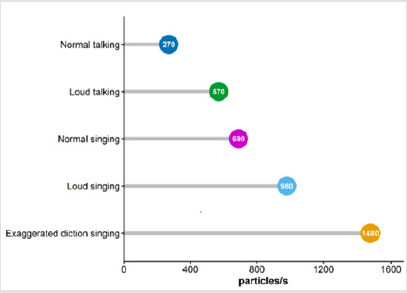
Figure 2: Median droplet emission rates during vocal activities summarized fromAlsved et al. [11].
The results showed a gradual increase in emitted particle rate from talking to soft singing to loud singing with singing at high pitch emitting the greatest number of particles. Though both experiments described above used an aerodynamic particle sizer for recording emissions, the emission rates (6-53 particles/s for vocalization) recorded by Asadi et al. [10] was order of magnitude lower than the rates (median rate 570 particles/s for loud talking) recorded by Alsved et al. [11] most likely due to presence of additional filters in the experimental setup of former. Nevertheless, both experiments were important to demonstrate that singing, an in particular loud singing that generate more air pressure in the vocal chord can generate significantly larger number of particles than normal talking between individuals (Figure 2). Peak emission rate recorded by Alsved et al. [11] for loud singing with exaggerated diction was nearly 3000 particles/s. Assuming a 10 μm particle size as discussed before, this would mean an outflow of nearly 3×105 virions/s, which is probably 0.001 times the particles emitted in coughing, but still significant in spreading infection.
Role of Air Flow System
Emission rates mentioned above are derived from purely
experimental setups that are far from public space environments
having air flow or HVAC system that may enhance travel distance of
emitted particles. Simulation studies [9] have shown that while at
zero ambient air speed, saliva droplets emitted by a person may hit
the ground within a 2-metre distance (something which is advised
by most governments and public health agencies as the social
distancing norm), presence of a modest background air flow at 4
km/h can extend the “safe distance” to 6 metres. Further, presence
of air flow also appears to reduce the droplet size by evaporation at
a faster rate, thereby heightening aerosol formation of the particles.
Another simulation study by Riediker et al. [12] assessed the effect
of air change of HVAC systems on temporal course of virions emitted
by breathing or coughing in a closed room of 50m3 size.
Though, this data does not include emissions from vocal
activities, but taking emission due to coughing of a typical person
as standard shows that with around 10 air changes/h (typical rates
in a public auditorium or a meeting room), the viral load attains a
plateau in less than 30 minutes with a steady-state concentration
of virions ~ 10/m3 volume. This number is rather low as a person
in the audience who typically breathes 0.5 m3/h air volume would
probably be exposed to < 10 copies of virus during a 2-hour
performance. However, the number would increase significantly
for an infected singer performing at high pitch in a smaller room.
This could possibly increase the breathing viral loads of person in
audience to 100 copies or more that are sufficient to cause infection
Discussion
With no end of the pandemic in sight, many reports are
emerging on spread of disease by asymptomatic individuals [13,14].
Absence of detectable symptoms like hypothermia, coughing,
sneezing or dyspnea makes it difficult to isolate and contain such
individuals. Moreover, with normal activities resuming at most part
of the world, it is likely that music and other performances will
also revive soon. Number of audiences may be curtailed in such
events, but an asymptomatic COVID-19 positive performer herself
can be a greater risk factor. Limited available data on music and
COVID-19 presented in this mini-review vindicates the heightened
potential of generating significant number of droplets during loud
speeches or high-pitch singing. As music involves exercising vocal
cords, such performance produces intermediate size droplets that
are less affected by gravity and are more likely to turn as aerosols.
Both studies with vocal activities reported in this review [15] have
recorded particles sizes mostly in 5-10 μm range, which did not
depend on the loudness or pitch of the vocal activity.
From the perspective of a singer, COVID-19 infection can have
long-term deleterious effects on the respiratory system affecting
their professional lives. For earlier forms of coronaviruses (SARS
and MERS), several studies have observed long-term respiratory
changes even after recovery [15]. For SARS-CoV-2, follow-up of a
large pool of patients from Italy for a period of 60 days post onset
of initial symptoms showed that ~ 88% still reported one of the
symptoms at the end of follow-up period, including 43.4% patients
presenting dyspnea. Also, several studies reported abnormalities
in chest CT image even for asymptomatic patients. A recent metaanalysis
synthesizing 7 such studies estimated around 63% patients
(95% CI: 44% - 78%) presenting chest CT findings including
ground-glass opacity though asymptomatic initially [16]. Perhaps
it will take a few more years to conclusively understand long-term
adverse effects of COVID-19 on respiratory system, but for now it
may be prudent to assume that SARS-CoV-2 may affect a musician
for some months even after recovery.
Overall, findings presented and summarized in this minireview
points to an emergent realization that practice of music,
in particular in confined areas can create an infection cluster –
not only due to social interaction between the audience but due
to particles emitted from an infected asymptomatic singer. Being
of intermediate size range, these particles have greater potential
towards aerosol formation aided by possible air-flow systems.
Under such situations, the 2-meter social distancing norms may
not be of relevance. Experiments [11] show that use of masks can
bring down the particle emission rate by two-third, but it is surely
not practical for a vocalist to deliver serene performance wearing
a mask. Though music performance in the time of COVID-19 may
soothe many souls but can also create new infection clusters among
practitioners and audience. Till the pandemic subsides, it would
be a safer option to contain musical performances in the realm of
online world.
Conflict of Interest
Authors declare no conflicts of interest.
Acknowledgement
Authors acknowledge the help of Ushnaa Kuri in preparation of (Figure 1).
References
- Koizumi N, Siddique AB, Andalibi A (2020) Assessment of SARS-CoV-2 transmission among attendees of live concert events in Japan using contact-tracing data. J Travel Med 27(5): taaa096.
- Sugano N, Ando W, Fukushima W (2020) Cluster of Severe Acute Respiratory Syndrome Coronavirus 2 Infections Linked to Music Clubs in Osaka, Japan. J Infect Dis 222(5): 1635-1640.
- Hamner L, Dubbel P, Capron I, Ross A, Jordan A, et al. (2020) High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep 69(19): 606-610.
- Naunheim MR, Bock J, Doucette PA, Hoch M, Howell I, et al. (2020) Safer Singing During the SARS-CoV-2 Pandemic: What We Know and What We Don’t. J Voice.
- Wei J, Li Y (2016) Airborne spread of infectious agents in the indoor environment. Am J Infect Control 44(9): S102-S108.
- Morawska L, Johnson GR, Ristovski ZD, Hargreaves M, Mengersen K, et al. (2009) Size distribution and sites of origin of droplets expelled from the human respiratory tract during expiratory activities. J Aerosol Sci 40(3): 256-269.
- Bar On YM, Flamholz A, Phillips R, Milo R (2007) Sars-cov-2 (Covid-19) by the numbers.
- Yang S, Lee GWM, Chen CM, Wu CC, Yu KP (2007) The size and concentration of droplets generated by coughing in human subjects. J Aerosol Med Depos Clear Eff Lung 20(4): 484-494.
- Dbouk T, Drikakis D (2020) On coughing and airborne droplet transmission to humans. Phys Fluids 32(5): 53310.
- Asadi S, Wexler AS, Cappa CD, Barreda S, Bouvier NM (2019) Aerosol emission and superemission during human speech increase with voice loudness. Sci Rep 9(1): 1-10.
- Alsved M, Matamis A, Bohlin R, Richter M, Bengtsson PE, et al. (2020) Exhaled respiratory particles during singing and talking. Aerosol Sci Technol 54(11): 145-1248.
- Riediker M, Tsai DH (2020) Estimation of Viral Aerosol Emissions from Simulated Individuals with Asymptomatic to Moderate Coronavirus Disease 2019. JAMA Netw open 3(7): e2013807.
- Liu J, Huang J, Xiang D (2020) Large SARS-CoV-2 Outbreak Caused by Asymptomatic Traveler, China Emerging infectious diseases. NLM (Medline).
- Rivera F, Safdar N, Ledeboer N, Schaack G, Chen DJ, et al. (20202) Prevalence of SARS-CoV-2 asymptomatic infections in two large academic health systems in Wisconsin. Clin Infect Dis.
- Helding L, Carroll TL, Nix J, Johns MM, LeBorgne WD, et al. (2020) COVID-19 After Effects: Concerns for Singers. J Voice.
- Tsikala Vafea M, Atalla E, Kalligeros M, Mylona EK, Shehadeh F (2020) Chest CT findings in asymptomatic cases with COVID-19: a systematic review and meta-analysis. Clin Radiol 75(11): 876.
