info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: January 17, 2018; Published: January 24, 2018
*Corresponding author: Lisa Marie Portugal, American College of Education, IN, USA
DOI: 10.26717/BJSTR.2018.02.000690
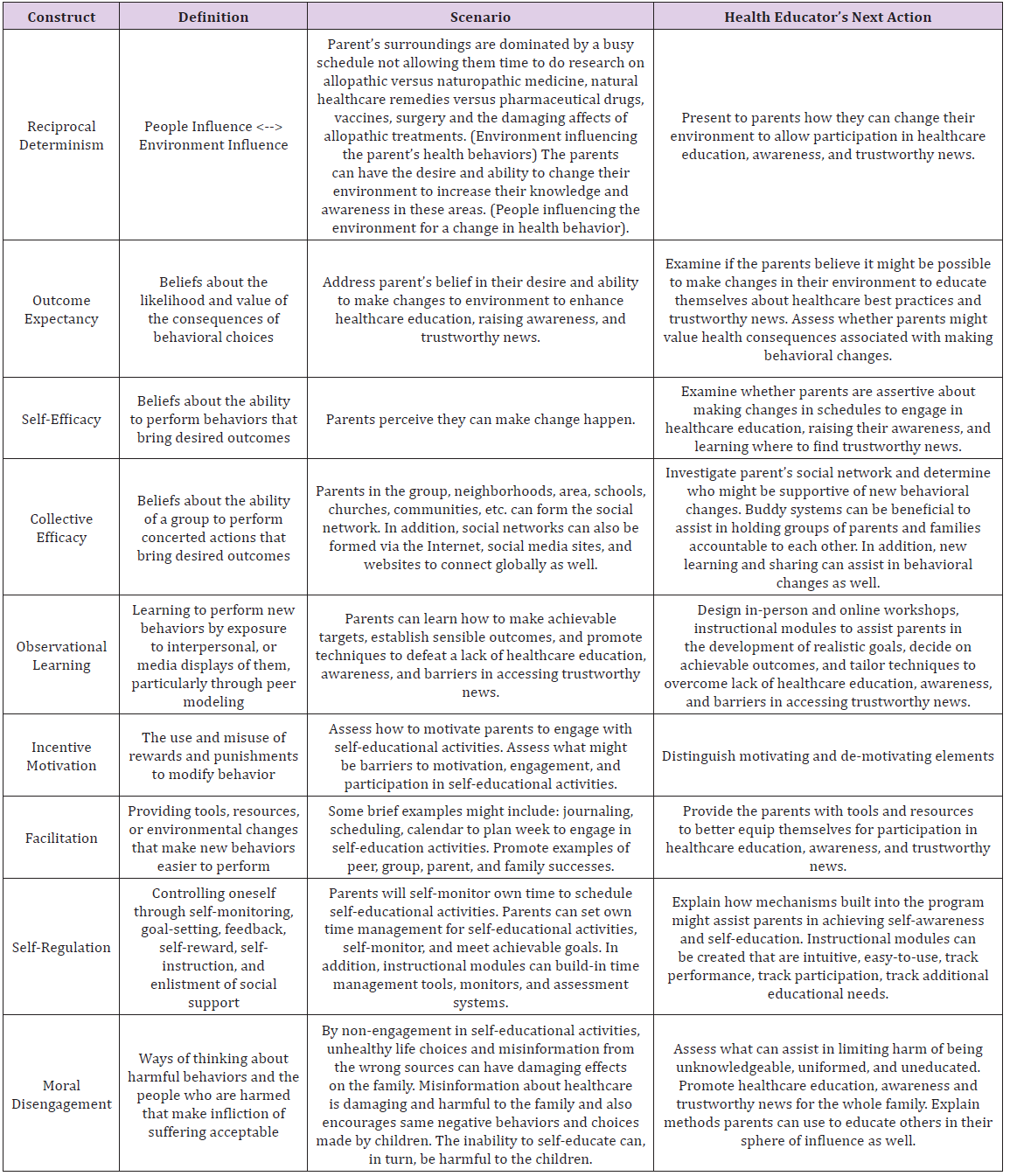
Social Cognitive Theory can address appropriate health and wellness change initiatives via the education of groups. Individualized and group action plans can be created and developed to address the overall health and wellness needs of families. This model and theory can assist in the education of preventing disease through health promotion and education and from a naturopathy perspective [1,2]. In addition, this model can assist in the development of health educational programs to understand and explain health behaviors and choices families make. The model can guide useful strategies and educational tools with in-person or online instructional modules.
Social Cognitive Theory constructs can be applied to health behaviors by addressing health needs of families and parents in any group and in any region or country. The instructional tools can be created in any language once the basics of the curriculum have been written. The program can be taught in person via workshops, in clinics, or can be accessed online globally. The curriculum can be taught individually or in groups as well. Individualized learning styles, culture, and environment on the target population can be addressed using adult learning theories, scaffolding instructional techniques, differentiated instructional strategies, and technology integration to meet the needs of parents and families where they are at cognitively. These methods can assist in raising parent’s and family’s awareness in an interactive, intuitive manner regarding health and wellness education [3].
A holistic, qualitative approach can be used to address specific needs, ailments, health challenges, cultural background, and ability levels of groups and families. In addition, cognitive dissonance theory must be taken into account when developing this type of health and wellness program to address misinformation the public has been indoctrinated with over many years. The key is to address families and parents with a holistic, individualized, naturopathy perspective over a Big Pharma, prescription-driven, one-size-fitsall system emblematic of allopathic practitioners [3,4]. The goal is to self-empower, educate, change negative habits, and assist in the development of lifelong healthy habits. Furthermore, the plan can address the value of whole body healing from a naturopathy medicinal perspective. A compare and contrast of allopathic versus naturopathic practices can be examined and built into the curriculum.
This example involves a group of parents. The parents have children of all ages and they tend to take family members to allopathic doctors mainly when someone is sick for vaccines, pharmaceutical drugs, antibiotics, and surgery. The goal is to educate parents and family members about
i. preventative healthcare / self-care in the home,
ii. natural remedies found in nature,
iii. natural nonGMO, Paleolithic diet or Paleo diet, and
iv. Using naturopathy doctors, providers, and services rather than allopathic and pharmaceutical services for healthcare needs (Table 1).
Table 1:
This plan addresses the existing health behaviors to help parents and families make a behavioral change by
i. educating them with appropriate tools according to their needs,
ii. informing them with current news
iii. supporting them with multiple resources, services, providers, and alternatives,
iv. providing support group access, and
v. providing follow-up, check-in or touch-base services, and on-going educational tools
This Social Cognitive Theory Mapping template is merely the vision or mapping out of overall goals and objectives. The specifics and details are created in a health and wellness educational plan and change initiative. Within a health and wellness educational plan, theories, principals, goals, objectives, strategies, techniques, instructional modules, workshops, services, providers, and program development tools are explained in further detail and depth.
PRECEDE-PROCEED Implementation Model is applied in the example Social Cognitive Theory Mapping involving a group of parents [1,2]. The example is provided for parents with children of all ages who tend to take family members to allopathic doctors most often for vaccines, pharmaceutical drugs, antibiotics, and surgery. The goal of this PRECEDE-PROCEED model is to educate and inform parents and family members about:
i. preventative healthcare / self-care in the home,
ii. natural remedies found in nature,
iii. natural nonGMO, Paleolithic diet or Paleo diet, and
iv. Using naturopathy doctors, providers, and services rather than allopathic and corporate pharmaceutical services for healthcare needs.
I. Phase 1:
The program’s desired result is to educate parents and families about naturopathy doctors, services, providers, and healing remedies versus allopathic and Big Pharma services. The main goals of this PRECEDE-PROCEED Implementation Model are to:
a. educate and inform with specific tools, resources, curriculum, and real news / studies,
b. change health behaviors,
c. change how individuals view allopathic versus naturopathy medicine, doctors, services, and providers,
d. offer new healthcare alternatives, choices, services, and resources, and
e. Help parents and families spread newly learned knowledge to others within the target population’s sphere of influence [5].
Changed negative behaviors into positive health choices are expected as well as newly gained information about how to be more proactive in healthcare education for the whole family using naturopathy services rather than allopathic, corporate pharmaceuticals.
II. Phase 2
The following priorities for the health behavior issue include:
a. The environmental and behavioral determinants impeding the actualization of the desired results are fake news, fake studies written by agenda-driven, big money agencies, false indoctrination, media brainwashing on television, magazines, radio, Internet, billboards (basically all media in Western nations), false medical information disseminated to the public via allopathic medical system and pharmaceutical companies
b. The conditions that need to be addressed to achieve the desired results include:
i. an openness and wiliness on the part or families and parents to learn new healthcare information,
ii. time in busy lifestyles,
iii. space such as in-person and/or online assessment, curriculum modules, resources, and
iv. access to service providers willing to participate and educate in the change agenda
The environmental factors, lifestyles, and/or behaviors that influence the conditions or issues include messaging from all Western culture systems that bombard the target population with incorrect information about healthcare, healthcare choices, and the real causes of illness and disease. In addition, busy lifestyles do not help parents and families understand (or even know the importance of) how to filter out inaccurate information they are bombarded with daily and where to seek accurate healthcare information. Finally, unhealthy behaviors regarding diet and eating habits are reinforced in Western nations and the target population does not have the full awareness about their poor choices.
III. Phase 3:
a. Predisposing circumstances affecting environmental, attitudes, and behavioral factors having influence in Phase 2 include false indoctrination within the culture about healthcare education, healthcare / self-care, and naturopathy medical services versus allopathic, corporate pharmaceutical indoctrination.
b. Enabling circumstances affecting environmental, attitudes, and behavioral factors having influence in Phase 2 include easy access to toxic prescription pharmaceutical drugs, toxic over-the-counter drugs, vaccines, surgery, fast food restaurants, and unhealthy pre-made brand grocery store foods rather than choosing natural foods that can take more time to prepare. Other enabling factors include all Western media avenues that bombard families with false information daily.
c. Reinforcing circumstances affecting environmental, attitudes, and behavioral factors having influence in Phase 2 include everyone in the target population’s lifestyle and sphere of influence are mostly likely indoctrinated with false information as well. All corporate big media avenues and the allopathic, pharmaceutical medical system serve as reinforcing agents disseminating false healthcare information and enabling dependency rather than fostering self-advocacy, self-efficacy, and the ability to self-educate or self-inform.
IV. Phase 4:
The policy and administrative factors influencing what can be implemented include building a coalition of naturopathy doctors, clinics, services providers, and educators. In addition, building a database of resources, tools, services, and curriculum modules must be provided to the target population. Finally, training needs to be provided to the target population on how to use and access the tools [5,6].
I. Phase 5: The Implementation Design: Social Cognitive Theory constructs will be applied to health behaviors of the target population. The design involves “creating in-person and online workshops and instructional modules to assist parents in the development of realistic goals, decide on achievable outcomes, and tailor techniques to overcome lack of healthcare education, awareness, and barriers in accessing trustworthy news” . The intervention will be conducted by addressing the healthcare needs of parents and families in a comprehensive naturopathy manner with before, during, and after medical and curriculum assessment.
II. Phase 6: The Process Evaluation: Medical and curriculum assessment will be on-going, tracked, monitored, and reported at the beginning, during, and end of the change initiative. Data will be compiled to address gaps, changes, revisions, alterations, individualized, and personalized needs of the target population. This will be done by on-going surveys, interviews, testing, and tracking of involvement in the curriculum.
III. Phase 7: The Impact Evaluation: The impact evaluation involves the monitoring and reporting aspects of
a. how well the target population learned the new information,
b. how much time was spent involved in the learning activities,
c. Whether the new information was actually applied in the daily choices, behaviors, and actions taken by the target population.
The desired impact of this intervention on the target population will be real and evident behavioral changes in the lives of parents, families, children, and individuals in their sphere of influence by way of improved health, less illness and ability to overcome illness faster, elevated self-efficacy levels, changes made in healthcare advisors and service providers (i.e. switch from allopathic to naturopathy), and changes made in diet [5,6]. The impact evaluative process will include direct observations, surveys, interviews, curriculum assessments, and before, during, and after medical assessments. All of the reporting and monitoring aspects listed can be done in a variety of ways such as in-person, telephone, email, online, and via curriculum module completion testing, and tracking.
IV. Phase 8: The Outcome Evaluation: The outcome evaluative process will be the same as the impact evaluation process which includes direct observations, surveys, interviews, curriculum assessments, and before, during, and after medical assessments. All of the reporting and monitoring aspects listed can be done in a variety of ways such as in-person, telephone, email, online, and via curriculum module completion testing, and tracking. Both quantitative and qualitative measures will be used throughout the program to assess, measure, track, and report findings [7].
The most beneficial aspects of this material includes the ability to learn new ways of thinking, applying theory in one’s best practices when educating others about healthcare, and interlinking theory with practical application. Practitioners, health educators, students, researchers, and community members should feel more prepared and confident choosing applicable models of evaluation as they study, practice, and apply various theoretical concepts when incorporated into their own program’s evaluation needs and complexity (Frye & Hemmer, 2012). The materials presented here can help health educators:
i. Understand frameworks for building capacity,
ii. Understand the role of health programs and policies,
iii. Understand the role of evaluation and assessment, and
iv. Apply theory-based health practices to any community health education program or agenda [8-10]. The skills and knowledge learned can be applied in both personal and professional life using theory, strategies, and intervention models to educate self, family, friends, neighbors, community, and professional associations. In addition, one can educate others in a professional capacity by understanding positive and negative influencing factors in the lives of others. Theory can be applied in personal, individualized, meaningful ways to capture the attention of others and help raise self-advocacy and selfefficacy levels for better health conditions and better health choices [11-14].
As a result of the materials presented here, one can feel confident in his or her abilities to effectively teach others how to improve health circumstances in a professional, theory-based manner. The tools presented in this paper can help health educators, practitioners, students, researchers, and community members feel more confident in having the ability to reach individuals and groups where they are at cognitively and work toward raising those abilities to higher levels of thinking, awareness, and proactive selfcare / healthcare [15-17]. Important goals to consider are to:
i. learn new ways of thinking, researching, and healing,
ii. teach others, and
iii. Pass the knowledge on within spheres of influence.
In closing, this healthcare educational program seeks to instruct parents and families about the choices they have in seeking out and providing naturopathy healthcare to their family and children. The program uses a Social Cognitive Theory Mapping template which maps out the overall objectives and goals of the program. In addition, the PRECEDE-PROCEED Implementation Model explains how the program will be most effective when mapped out by the expected end results anticipated by the program’s goals. Finally, information technology will be used when interpreting educational interventions from theory into practice by mapping out the PRECEDE/PROCEED model to analyze expected outcomes of the program with quantitative and qualitative measures [7,18,19].


























