info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: November 16, 2017; Published: November 29, 2017
Corresponding author: Tribhuwan Narayan Singh Gaur, Associate Professor Orthopedics, People’s College of Medical Sciences And Research Centre, Bhanpur, Bhopal, Madhya Pradesh 462037, India
DOI: 10.26717/BJSTR.2017.01.000547
Introduction: Most common fracture in elderly patients is distal radius fracture. The most common method of management is closed reduction and immobilization. The aim of the study is to evaluate the analgesic effects of hematoma block for closed reduction of distal radius fracture.
Materials and Methods: A prospective study was carried out among 50 patients of age >60 years of either sex who had fracture distal radius between 2015-2016. The patients having multiple fractures, pathological fractures were excluded from the study. After taking informed written consent, reduction of fracture was done following after infiltration with 2% lignocaine into fracture hematoma site. Pain score was compared by VAS before, during and after manipulation. Time taken from presentation at emergency department to reduction and discharge from hospital was also recorded.
Results: 50 patients of mean age 65.1 years, male: female 22:28 with fracture distal radius were studied. Mean time from admission to fracture reduction was 2.05 hours. Discharge time from hospital after reduction of fracture 2.0 hours .Average VAS during reduction was 0.94. 10 minutes after reduction VAS was 0.20.
Conclusion: For closed reduction of distal radius fracture, hematoma block with lignocaine is safe and effective alternative to other form of anaesthesia.
Keywords: Eldely Patient; Distal Radius Fracture; Haematoma Block; Close Reduction
Abbreviations: PR: Pulse Rate; RR: Respiratory Rate; BP: Blood Pressure; SO: Oxygen Saturation
Distal radius fracture is most common fracture of musculoskeletal system. It accounts for about 16% of all fractures treated at emergency department [1-4]. Fracture distal radius is most common in elderly and more in females than males [5- 7]. It usually occurs due to minor fall than severe trauma [8,9]. Various methods are used to decrease the pain during closed reduction of fracture radius like brachial plexus block, intravenous regional anaesthesia, general anaesthesia, conscious sedation and haematoma block. Each of these methods has certain merits and demerits [7]. The aim of the study was to evaluate the result of hematoma block for closed reduction of distal radius fracture.
This was a prospective study done in 50 patients of age >60 years of either sex at PCMS&RC, Bhopal, M.p in department of orthopaedics and Anesthesia, between 2015-2016.cases were posted for closed reduction of distal radius fracture at orthopaedic OT. After taking and informed written consent, the patients were taken for manipulation under hematoma block. The following parameters were recorded for study:
a. Demographic data
b. Pain score by VAS before, during and 10 minutes after reduction (VAS on scale of 0-10, zero no pain and ten being intense pain).
c. Time from presentation to hospital to reduction of fracture and time taken for discharge from hospital following reduction.
Patients having multiple fractures and pathological fractures were excluded from the study.
Preanaesthetic evaluation was done in all the patients of study. Inside OT, suitable intravenous line was secured and multipart monitor connected for continuous monitoring of Pulse Rate (PR), Respiratory Rate (RR), Blood Pressure (BP) and Oxygen saturation (SpO2). Following proper sterilization of the affected part, hematoma was confirmed by aspiration of 1-2mL of old hematoma blood. 10mL of 2% lignocaine was injected into the hematoma at the dorsal aspect of wrist and also into the adjacent periosteum in an aseptic manner. Massaging was not done after lignocaine injection. Reduction of fracture was allowed 10-15 minutes after injection of the drug. Immobilization was done following reduction by plaster of paris cast. Patients were not given any other analgesic before the procedure. Pain score by VAS was recorded before, during and 10 minutes after reduction of fracture. Total time in presentation at emergency department to reduction and discharge from hospital after reduction of fracture was recorded.
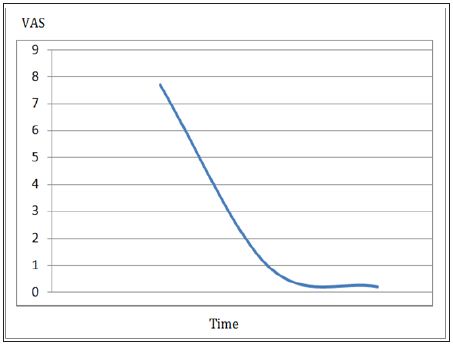
Demographic data like age and sex were comparable in both the groups in Table 1. The above table shows demographic characteristics of the study population. The mean age in years was 65.01 years. The ratio of male: female was 22:28. Table 2 shows time taken from admission to reduction and also reduction to discharge from hospital. Average time taken for admission to reduction was in our study was 2.05 hrs, and average time taken from reduction to discharge from hospital is 2.0 hrs. Table 3 shows the VAS Score 10 minutes before reduction, during reduction and 10 minutes after reduction. The average VAS score 10 minutes before reduction was 7.68, during reduction was 0.94 and 10 minutes after reduction was 0.2 recorded. The graphical representations VAS score with tme given in Figure 1.
Table 1: Demographic data like age and sex were comparable in both the groups.
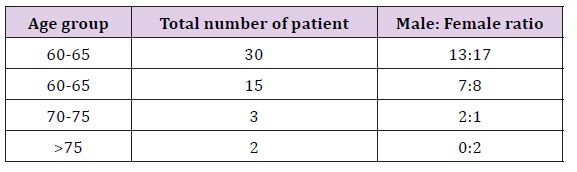
Table 2: Shows time taken from admission to reduction and also reduction to discharge from hospital.
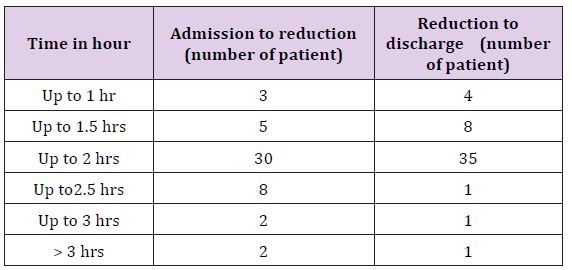
Table 3: Shows the VAS Score 10 minutes before reduction, during reduction and 10 minutes after reduction.
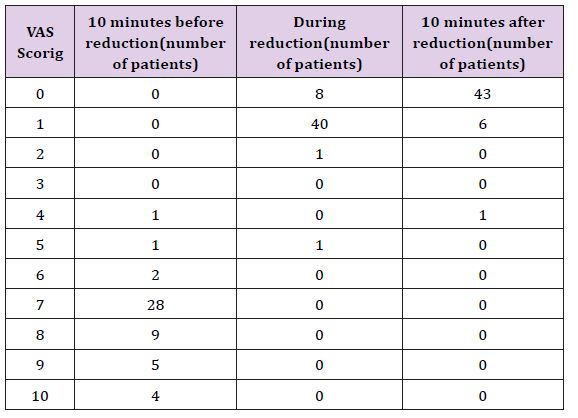
Figure 1: The graphical representation of VAS scores with time.
There are different methods to relieve pain during reduction of fracture of distal radius as described by different authors each having its own merits and demerits. Haematoma block has been studied as a procedure for fracture reduction by various authors. Kendal et al. [5] studied hematoma block in 1995. The increasing cost and time taken for general anaesthesia in comparison to hematoma block for reduction of distal radius made hematoma block more popular. Singh et al. [4] did a comparative study between haematoma block and conventional sedation in 1992 and found that pain score in hematoma block was significantly low in comparison to sedation group [10]. Compared results of brachial plexus block and haematoma block for reduction of fracture radius in 2008. He found no difference in analgesic effect between the study groups. Funk [7] in a study compared the VAS during reduction of fracture radius between IV general anaesthesia and hematoma block and found that VAS in general anaesthesia group was zero and hematoma block was 3.7.
Demographic data in our study is comparable to other studies showing mostly elderly and females affected by this fracture [5]. In our study, VAS during reduction was 0.94. This is different from the result obtained by Funk. This might be due to waiting for 10 minutes after giving lignocaine into the hematoma for the block to be effective - the procedure followed in our study.
Post reduction pain score in our study is comparable to study by Funk. We obtained a score of 0.20. This could be explained by the fact drug administered was lignocaine- a local anesthetic, which also contributed to post procedure analgesia. In our study, we found a significant reduction in mean time from admission to reduction of fracture and discharge from hospital in compare to other modality of anesthesia; this is similar to the study of Funk. Usually, other modality of anaesthesia requires an operation theatre, anaesthesia machine, a source of oxygen, fasting protocol of at least 6 hours and continuous monitoring, which is time consuming and costlier. Haematoma block for reduction of distal fracture radius can be done as Non-Operating Room Anaesthesia - NORA, at emergency department itself. Moreover, it can be done in a set up where a skilled anesthetist is absent or proper OT set up is not available.
During hematoma block by infiltration, the close fracture maybe converted to an open fracture giving way for the entry of microorganisms thereby causing infection [11]. However, in our study, we did not witness any such complication, which could be because of strict aseptic protocol being followed.
Thus, we conclude that hematoma block for reduction of distal fracture radius is a safe, simple and effective alternative to other type of anesthesia. It is also safe procedure in compare to other modality of anesthesia but should be given in the presence of qualified anesthetic.

























