info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: October 27, 2017; Published: November 02, 2017
Corresponding author: Faris Dawood Alaswad, NMC Speciality Hospital, General Surgery, Alnahda, Dubai 7832, United Arab Emirates
DOI: 10.26717/BJSTR.2017.01.000490
Primary malignant tumors of the duodenum represent 0.3% of all Castro-intestinal tract tumors but up to 50% of small bowel malignancies. Primary malignant tumors of the duodenum must be differentiated from malignant tumors of the ampulla, pancreas and common bile duct. The most frequent tumor of the duodenum is Adenocarcinoma [1,2]. Other primary tumors are lymphomas, leiomyosarcomas, carcinoid tumors, gastrinomas, and stromal tumors. Adenocarcinoma of the duodenum may arise from duodenal polyps observed in familial polyposis or Gardener’s syndrome, or be associated with celiac disease [3,4]. The tumor can be located in any part of the duodenum but the most frequent location is the second part. Malignant tumors of the duodenum are observed with the same frequency in men and women. The peak of frequency is the sixth decade, although the disease may develop in younger patients. Signs and symptoms are non specific. The main symptoms are: abdominal pain (15 to 60% of patients), weight loss (30 to 59%), nausea and vomiting (25 to 30%), jaundice (20 to 30%), hemorrhage (10 to 38%). A palpable abdominal mass is found in less than 5% of the patients [5].
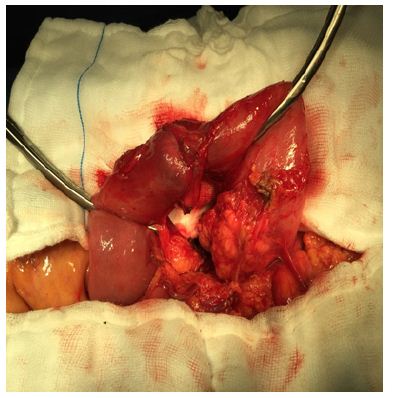
50-year-old women presented with an acute attack of vomiting endoscopy done and the cause was found to be a sub mucosal tumor located in the third part III of the duodenum, 5 cm distal of the papilla of Vater An emergency laparotomy after admission and correction of fluid and electrolyte was done. Ligation of tumor-feeding vessels with primary, definitive surgical therapy was performed by partial resection of the duodenum with a duodenojejunostomy. Feeding jujeunostomy was done also to supply enteral feeding postoperative. Histology revealed an Adenocarcinoma with a diameter of 2.5 cm after that the patient recover smothly and went home after 10 days to be followed on outpatient basis [6-8].
Tumors of the duodenum are a rare cause of upper gastrointestinal obstruction. Partial resection of the duodenum is a warranted alternative to a duodenopancreatectomy, as this procedure has a lower operative morbidity, while providing comparable oncological results [9-12].
Primary malignant tumor of the duodenum is a very rare cancer and is observed with the same frequency in men and womenthe peak of frequency is the sixth decade, although the disease may develop in younger patients. Signs and symptoms are non specific [13,14]. The main symptoms are: abdominal pain (15 to 60% of patients), weight loss (30 to 59%), nausea and vomiting (25 to 30%), jaundice (20 to 30%), hemorrhage (10 to 38%) (Figures 1-5).
Figure 1:

Figure 2:
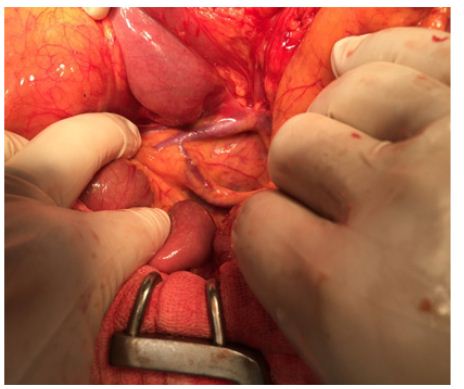
Figure 3:
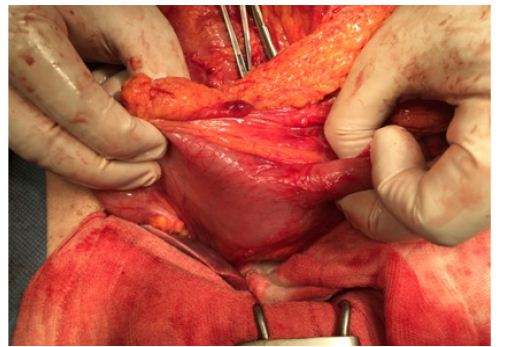
Figure 4:
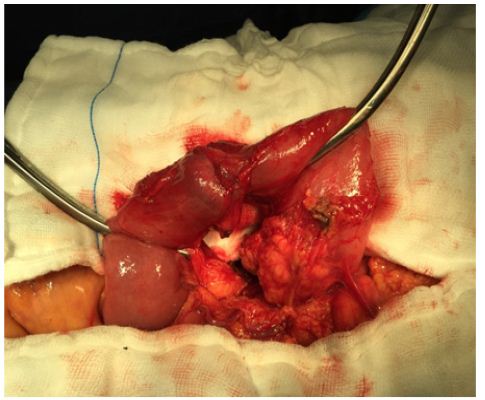
Figure 5:
A palpable abdominal mass is found in less than 5% of the patients .the diagnosis is with many diagnostic methods such as Barium studies of the upper intestinal tract which had been have been replaced by fiber optic endoscopy. Barium examination show in most cases an irregular stricture of the duodenum, but can be normal or misleading. Fiber optic endoscopy allows a precise location of the tumor and endoscopic biopsies which confirm the diagnosis [15-18]. The Preoperative staging is not easy and No study has evaluated the best method of preoperative staging of malignant lesions of the duodenum. Some authors use ultrasonography for the diagnosis of liver metastases; the accuracy of CT scan, MRI and angiography have not been studied. These investigations are not performed routinely, most of the patients being operated on as only for a palliative procedure.
Endoscopic ultrasonography has been reported to be useful for the preoperative staging of ampullary and pancreatic carcinomas. No study reports its accuracy in the preoperative evaluation of malignant duodenal tumors. Five to 40% of the patients have distant metastases or peritoneal seeding at the time of diagnosis [6]. The treatment of such cases is not yet very clear with guidelines and due to the low incidence of the disease there is no randomized study comparing different types of treatment. Complete surgical resection is the only hope for cure. Two types of surgical resection are available: pancreatoduodenectomy associated with various types of lymphadenectomies or segmental resections [7,8]. Pancreatoduodenectomy has been advocated as the surgical procedure of choice because it offers the possibility of regional lymph node resection. Nonetheless good long-term results have been observed with segmental resection, particularly for tumors of the distal part of the duodenum [9]. When local extension or metastatic disease precludes curative resection, palliative procedures such as gastrojejunal anastomosis can be performed [19,20]. Laser photo coagulation has been proposed for patients unfit for surgery with good palliation on hemorrhage and obstructive symptoms.

























