info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: October 25, 2017; Published: November 02, 2017
Corresponding author: Fazal Rehman Babar, Lecturer Preventive and Public Health Dentistry Bolan Medical College, House: #594 A-1, City Brewery Road, Quetta, Balochistan, Pakistan
DOI: 10.26717/BJSTR.2017.01.000488
Viral hepatitis B and C are a major health concern worldwide, with 170 million people chronically infected and at risk of liver cancer, cirrhosis or liver failure. The modes of transmission include intravenous drug use, blood products, body fluids, tattooing, surgical procedures and sexual intercourse. Thus Health Care Professionals have a high exposure to HBV and HCV infection and are at risk to it. A cross-sectional quantitative survey on 84 House Officers was conducted in Dental Surgeons of Khyber College of Dentistry and Bolan Medical College through a semi-structured questionnaire. Out of total 84 subjects 44 were male and 40 were female, with mean age 24.7+ 1.44. The subjects had good level of knowledge regarding disease transmission, prevention and treatment, which was from 85-90%, generally positive attitudes toward patient care was 67.9% and 59.5% consider doctors at risk of infection. Over all.53% consider media as most convenient source of information. Needle prick was high as 48.3%. 91.7% candidates were vaccinated and some of them attained few lectures regarding hepatitis. Good knowledge which can be improves by formal training and follow of the preventive measures in dental care procedures.
Keywords: Hepatitis B and C; Dental House Officers; Knowledge; Attitudes; Practices
Abbrevation: HIV: Human Immunodeficiency Virus; HCV: Hepatitis C Virus, HBV: Hepatitis B Virus; PPE: Personal Protective Equipment; KCD: Khyber College of Dentistry; BMC: Bolan Medical College
Medical and dental health care professional are more vulnerable to various infections like hepatitis B and hepatitis C viruses, staphylococci, streptococci, herpes simplex virus types 1, human immunodeficiency virus (HIV), mumps, influenza, rubella and other prevalent infectious agents [1]. Hepatitis has become one of the major health care problem of the world with about 170 million patients are chronically infected with hepatitis C (HCV) with 3-4 million new infections each year and 8000-10000 death occur each year. About 3% of the world population is affected by hepatitis C virus [2]. Worldwide, an estimated two billion people have been infected with the hepatitis B virus (HBV), and more than 350 million have chronic liver infections [3]. World Hepatitis Day observed May 19th aims to raise global awareness of hepatitis B and hepatitis C and encourage prevention, diagnosis and treatment [4].
Pakistan is also facing the brunt of this disease and reported prevalence of HCV about 4-7% and that of HBV is about 3-4% by different surveys reported from country [5,6]. The incidence of new cases of HBV is decreasing worldwide after universal vaccination [7]. Lack of education and awareness regarding its spread are the main factors contributing to this disease [8]. An estimated 100 million individuals worldwide are chronically infected with HCV. High prevalence rates have been found in Southeast Asian countries, such as Thailand, Malaysia and India. In Pakistan, the sero-prevalence of HCV is 6.7% in women and 1.3% in children [9]. The virus is mainly transmitted through transfusion of contaminated blood and blood products, sexual contacts, intravenous drug users, traditional health practice is also common in the region. It is an occupational hazard for health care providers and require adherence to universal precautions [10]. The objective of the study was to assess the knowledge, attitude, and practices regarding Hepatitis B and C among Dental surgeons and to compare the Knowledge, attitudes and practices among house officers of the two different public Sector Medical/Dental colleges.
The study design was Cross Sectional Descriptive Study-KAP Survey. Structured self-administered questionnaire which was pilot test in KCD only before was used for knowledge, attitudes andpractices of Dental house officers regarding the Hepatitis B and C. The survey was conduct from October 2011 to December 2011 on all the House Officers of both colleges. A Purposive sampling technique with size of 84 was used, 40 house officers were from Khyber College of Dentistry and 44 from Bolan Medical College, Dental Section. Data were analyzed using SPSS version 16.0. Mainly Descriptive statistics were used. Categorical variables like gender and questions about knowledge and practices were described as frequencies and percentages while Continuous variables were described as means and range. Chi square tests were used for significance.
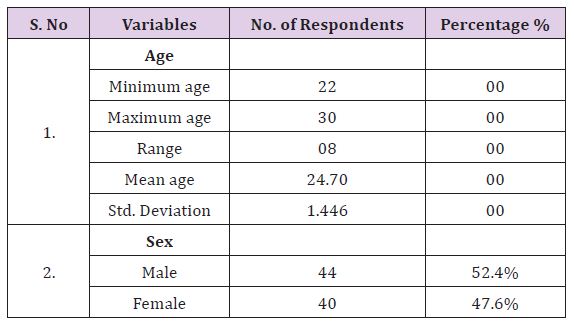
With a response rate of 87.5% (84), where 47.6% (40) house officers were from Khyber College of Dentistry and 52.4% (44) house officers participated from Bolan Medical College, Dental Section. Table 1 show the mean age and sex wise participant of study.
Table 1: Socio demographic characteristics of the study population (n = 84).
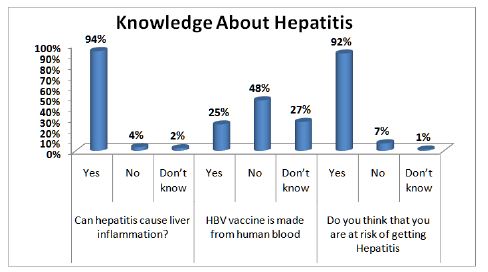
About 99% answered that hepatitis cannot be caused through casual contact, such as holding hands or hugging. Regarding the knowledge of the disease, 100% (n=84) of the house officers knew that a HBV and HCV positive person carrier are having the risk to infect others and spread it. About the dangerous route of infection of hepatitis was very good and mainly all house officers identify the prick from a contaminated instruments/syringe (81) 96.4%, while small percent 1.2% mark the Oro-fecal route. The best preventive method for it was marked 100% respondents that using the sterilize instrument/syringes (Figure 1) While some dentists also specify the blood product and the use of disposable instruments. Knowledge about treatment was (62)73.8% answer that the treatment of hepatitis is possible and its cure partially from it, while (12)14.3% answer that from treatment the patients cure totally and (10)11.9% answer in negative that treatment do not cure from HBV and HCV. Mass media was reported mainly by respondents (52.4%) as the main source of information about HBV and HCV, Medical institute (26.2 %) as shown in (Table 2).
Table 2: More convenient way for information about HBV and HCV.
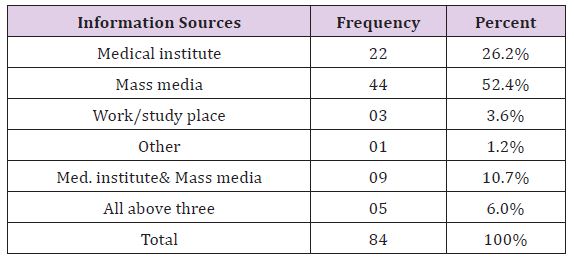
Figure 1: General Knowledge about Hepatitis.
The most important question about Vaccination of Hepatitis B was positive and 77 (91.7%) students are been vaccinated against it and 8.3% has not done the vaccination. The attitude toward the believe in vaccination protection against Hepatitis B was up to the mark, 92.9% answer in positive and 4.8% was not believe in the vaccination. As shown in the Table 3, the changing of gloves was also taken positive by many house officers and 96.4% said it’s not wastage of time and it important for their protection. The interesting question about the attitude was that if you personally get infected with hepatitis B or C whom will you tell about it, the answer mostly answer was doctor which show their trust and the right person for their problem, 51.2% trust in doctor and secondly 16.7% said that they would tell their parents about the infection of hepatitis.
Table 3: Answers about Attitude questions asked from house officers (n = 84).

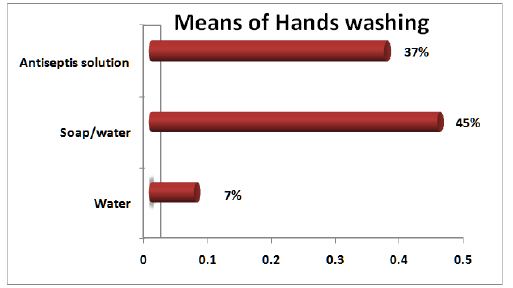
Hand washing with Plain water was reported 7.1% of the times, soap/water 45.2% and the use of antiseptic solution 36.9 %. At the same question about 8% said they do not wash hand after every patient and the reasons they show was the shortage of time and interrupted or short supplies of soap or anti-septic solution. The use of personal protective equipment (PPE) masks and apron or overall were reported 41.7% (35) of the times, the protective goggles in OT or MOS were marked less 3.6% while the 59.2% of the respondents reported. Forty one House Officers (48.8%) reported needle pricks during the last one year whereas 1.2% said they didn’t remember about the pricks. Of those 41 House Officer about 76 % of the sample responded with 1-3 pricks in their last year career, while 19% (08) show the results of 4-5 times of pricks and the alarming results was more than 5 times prick in the last year, (Figure 2) and it was 05% of the all (Table 4 ).
Table 4: Answers about Attitude questions asked from house officers (n = 84).
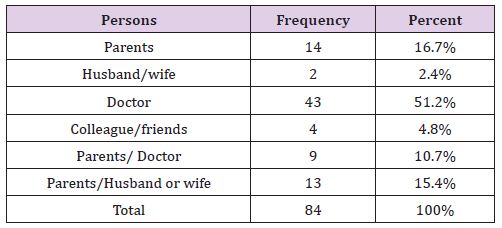
Figure 2: Bar chart showing different means of hands washing by house officers.
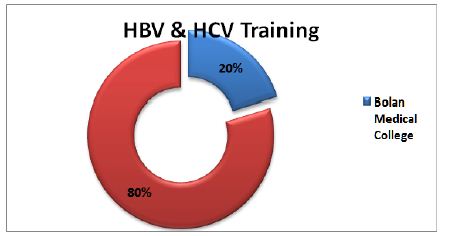
The knowledge about Hepatitis of both colleges was of good level, all house officers of both colleges were aware of Hepatitis and its risk from carrier. Protection through Vaccination in KCD dental house surgeons was 97.5% as compare to 87.6% of BMC which is significance with p-value 0.003. Changing of gloves for was masked by 97% of both institute house officer as not the wastage of time, which shown their behaviour to gloves changing and protection. Needle prick in the last one year was more and was alarming one, and was more about 61.5% in KCD and 36.4% in BMC house officers. (Figure 3) and (Figure 4) Exposure to HBV & HCV patients was high as about 82% in both hospitals house officer and they treated and expose to hepatitis positive patients from 1 to 20 or more than 20 no of patients. Screening policy of KCD was good and each and every patient was screen before any dental treatment and for minor or major oral surgeries, whereas in BMC there was no such screening policy for every patient (Table 5).
Table 5: KAP of Khyber college of Dentistry Vs Bolan Medical College.
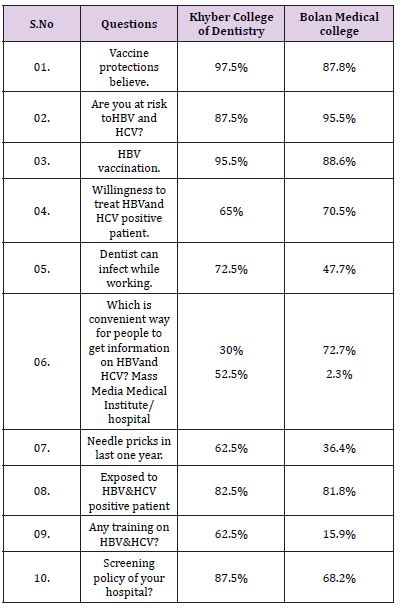
Figure 3: House Officers exposed to No. of pricks in past one year.
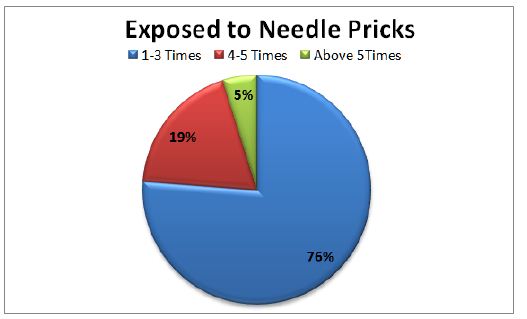
Figure 4: Training on HBV and HCV at Khyber College of Dentistry and Bolan Medical College.
There have been studies regarding the knowledge, awareness and practices of hepatitis B & C. However, the majority of these have reported a different level of knowledge and attitude, depending on their study population education and awareness, which limits the generalize ability of their results to the general population. On the other hand, cultural diversity in the different cities of Pakistan also necessitates the performing separate population-based studies in the various regions.
There have been studies [11-13]. Regarding the knowledge/ awareness, attitude and Practice or believes hepatitis B and C in Pakistan. The objective of this study was to determine level of knowledge and attitude about HCV and HBV in dental surgeons and practices with patients reporting for dental treatment. Regarding the availability of a successful treatment of HBV or HCV 15.4 % were aware about patients cure completely from it, where about 73.8% responses that they cure partially from treatment and 11.9% response that no such treatment exists for disease. This is much better than a study done among medical students of Karachi; their response was 48.2% [14]. Use of Sterilize instruments was chosen by 100% of working house officers and some also identified the use of disposable instruments.
Figure 5: Needle pricks in Khyber College of Dentistry Vs Bolan Medical College.
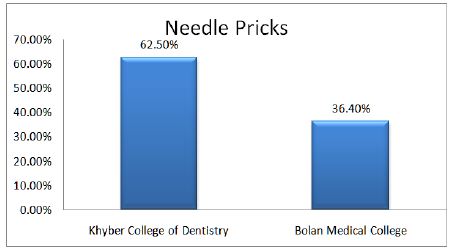
About 96.4% identified the prick from contaminated instruments as the dangerous risk for dentist (Figure 5). The knowledge about the route of transmission was almost 100% know the blood transfusion. The results of our study was even more knowledge then the study done by Abbasi Shaheed hospital on five dental institutes of Karachi as their knowledge about route of transmission was 86.16% [15]. 91.7% of the house officers were vaccinated against Hepatitis B and they believe that through vaccination the prevention is possible and respond was 92.9%, which can be comparing with study done on medical students in Bangladesh where 85% was aware of vaccination and 65.5% were vaccinated [16] and 63% was in south Korea dentist [17] which is less than our study. Similarly 96.4% don’t consider the changing of gloves as wastage of time and resources. About the doctor risk of infection while working at hospital/clinic was much positive as 59.5% said yes to the question and 29.8% responded that they are not at risk at all.
The use of personal protective equipment was good in practices; Gloves were used almost while treating patients but at same short supplies were reported by 5.7%. In study on dental care workers in Japan 25% deny to change gloves for every patient while 17% don’t wear it [18]. Mask and overall used in surgical procedures was 59.6%, while the remaining percent mark all the protective equipment’s i.e. gloves, mask, overall, goggles and rubber boots. The use of protective and barrier method in dentist of Durban, South Africa was also high as it were reported by our study respondents [19]. Quite a big percentage (82.1%) of our respondents was exposed to HBV and HCV patient/s in their professional career. About 1-30 patients with HBV and HCV positive are been exposed or treated by house officers. Mostly used mask, double gloves, goggles, sterilize/disposable instrument and apron, while masks, gloves and apron was used the most. This was in contrast with study done on Iranian surgeons who use double gloves only 24%.
A study was conducted to evaluate the magnitude of awareness regarding transmission of Hepatitis B and C amongst the Dental house surgeon. This study also focused on the practice of dental health care professionals regarding the protective and preventive measures to prevent the transmission of hepatitis and infection control. “Safe practices” would decrease the diseases burden and will save resources for the Public and Govt. Our health care planners need to understand it and our teaching and training programs need complete re-orientation to achieve this goal [20-25].


























{kind=link}