info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: August 24, 2017; Published: September 11, 2017
Corresponding author: Vincent K Mukthar, Deparment of Nursing, Egerton University, P.O. Box 536-20115, Egerton, Kenya
DOI: 10.26717/BJSTR.2017.01.000346
Background: There is general knowledge deficiency on the Standard Precautions that contribute to risky behaviours amongst nurse and that compliance with the Standard Precautions is still not a common practice.
Objective: To analyze the effectiveness of Social Cognitive Theory-based educational Intervention to Registered Nurses in influencing the knowledge and compliance with the Standard Precautions in Selected County Referral Hospitals in Kenya.
Methodology: This was a prospective Quasi Experimental study. The respondents were registered nurses in the selected hospitals. The instruments were self-administered Questionnaires and Observational schedule. Data were analyzed using Statistical Package for Social Sciences version 20. The study has employed both descriptive and inferential statistics to analyze the data. Results have been presented in text, tables and graphically.
Findings: The knowledge on the Standard Precautions increased from 57.7% to 66.2% after the educational intervention. The selfreported compliance on the Standard Precautions improved from 46.3% to 73.8% after the educational intervention. The observed compliance on the Standard Precautions was 62.7%. The observed compliance scores on the Standard Precautions increased from 61.3% to 67.6% after the educational intervention.
Conclusion: It is the submissions of this study that both self-efficacy and collective efficacy of healthcare workers on the standard Precautions is a function of vicarious learning, conducive environment, motivation and robust cognitive understanding. Educational interventions should be rooted in the Social Cognitive Theory, Thorndike’s Principles of Learning and principles of androgogy for greater impacts and desirable outcomes on nurses.
The Standard Precaution is a package of infection prevention and control practice applied in the clinical set up by the health providers to reduce the risk of transmission of blood borne infections. They include guidelines and principles in hand washing, use of gloves and other protective barriers eg aprons, gowns, goggles and masks, proper handling of sharps, disinfection of soiled instruments and linen and proper management of sharp injuries [1]. Most studies documents that generally there is general lack of awareness and limited access to information about the appropriate precautions to prevent exposure which in some way contribute to risky behaviours amongst nurses [2]. However, the general knowledge on the Standard precautions is better than other health professionals [3].
Though it is a fact the compliance with the Standard Precautions prevents infections and protects health care workers during provision of care, the compliance is still not a common practice and thus poses a challenge. Some of the attributes to low compliance includes lack of time, lack of awareness, deficient lifelong learning process, sheer carelessness or guts to engage in risky behaviours, inadequate equipments and protective equipments [2,4,5]. Available literature dwell more on cross-sectional studies on compliance on the Standard Precautions [5], therefore this study aimed to investigate the effectiveness of using an intervention (structured education) to influence the knowledge and compliance with the Standard Precautions. This study had three null hypotheses:-
a. There is no significant difference in self-reported knowledge scores on the Standard Precautions before and after the intervention
b. There is no significant difference in self-reported compliance scores on the Standard Precautions before and after the intervention
c. There is no significant difference in observed compliance scores on the Standard Precautions before and after the intervention
This study was based on the Social Cognitive Theory and borrows the principles from Thorndike Theory of Learning. The above theories are widely used in health and nursing studies in an attempt to predict and/or explain health behaviours. They inform complex human behaviours and unexpected way of doing things [6]. Social Cognitive Theory is a theory developed by Albert Bandura in 1960s and improved in late 1980s.The gist of The Social cognitive Theory according to [6], is that human beings learn by observing others (vicarious learning), within the context of social interactions in a setting herein referred to as the environment but subject to ones cognition which entails ones personality. The learned behaviours are central to ones personality. What makes the Social Cognitive Theory unique is that it proposes that learning considers how people maintain a learned behavior, considers past experiences and is a collective function of Self-Efficacy, goals and Outcome expectancies. Social Learning Theory states that people when people observes a model performing a behavior and the consequence of the behavior, the remember the sequence of events and are likely to the information to guide subsequent behavior and more so, it will prompt them to try out an already learned behavior. The Social Cognitive Theory emphasizes that the dynamic interaction (Triadic Reciprocal Determinism) between people (personal factors), their behaviors and their environment as demonstrated by the following (Figure 1).
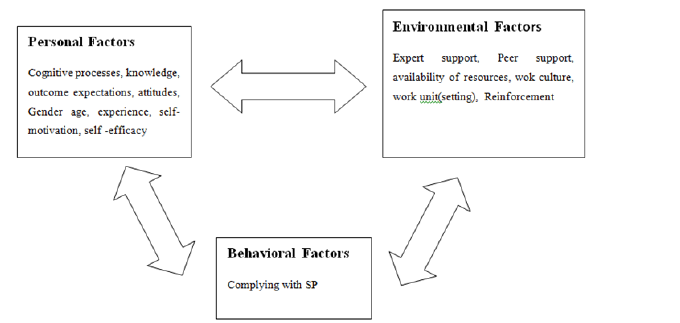
Figure 1: Social Cognitive Theory (Modified) adapted.
This was a prospective Quasi- Experimental study precisely Nonequivalent Control Group study whereby the units of observation (nurses) were not be randomly assigned to either study or control groups. The study groups were all the nurses from Baringo County Referral Hospital (BCRH) while the control groups were all the nurses from Nandi County Referral Hospital (NCRH). The independent variables that were manipulated were the structured education based on Social Cognitive Theory while the dependent variables were knowledge and compliance with the Standard Precautions.
The study was undertaken in two county hospitals in Kenya namely Baringo County Referral Hospital (BCRH) as study group and Nandi County Referral Hospital (NCRH) as control group. The county hospitals are hospitals that provide specialized care, [7].
The study populations were all Registered Nurses from the two health facilities purposively selected for this study, namely Baringo County Referral Hospital and Nandi County Referral Hospital. Baringo County Referral Hospital has Registered Nurses’ population of eighty six (86) unpublished BCRH Records (2015), while Nandi County Referral Hospital has Registered Nurses’ population of seventy four (74) unpublished NCRH Records (2015).
This study applied Total Population Sampling (census) owing to relatively small size of the population.
A quantitative method of data collection was used. The study instruments (tools) were is self- administered Structured Questionnaires and observation Checklist/Schedule. The questionnaires were administered to the respondents in both the study and control groups. Baseline data was collected initially before the intervention(baseline information), then the intervention(structured education) were administered to the study group as a package of six lessons within two months then followed up for a period of a six months and then the final data post-intervention.
The intervention model was based on the Social Cognitive Theory which is commonly used in health education and promotion. Social Cognitive Theory has three constructs namely Personal, environmental and Behavioural constructs that interact in what is referred to as Triadic Reciprocacy to influence learning as a conscious and deliberate effort to improve the dependable variables namely knowledge and compliance of the Standard Precautions. It also borrows from Thorndike’s Principles of Learning as earlier outlined in the Theoretical Framework.
The data collection instruments were reviewed by nursing education experts in the School of Nursing Sciences in the University of Nairobi. All the tools were in English language which is well understood by all the qualified nurses in Kenya. Pretesting was being done in a similar facility. Obtaining of Pretest data, administering of structured education to the study group and obtaining of postintervention data was done by trained enumerators. They delivered their teaching based on an established lesson plans. Two tests were used to test reliability of the instruments. The questions applying Likert Scale were tested using Cronbach Alpha Method which when ran yielded Reliability Coefficient of 0.82 and thus was considered reliable. The other choice questions of the instrument were tested for reliability using Split-Half test which yielded a reliability Spearman-Brown coefficient of 0.86 and thus such tool was considered reliable.
The data collection instruments were self -administered structured questionnaires and observation Schedules. The Preinterventional questionnaires captured the socio-demographic attributes of the respondents, self-reported knowledge of the Standard precautions and self-reported compliance with the Standard Precautions. The observational schedules captured data on observed compliance with the Standard precautions. It was capturing if an item is being done or present always, done sometimes or not done at all. The same observational schedule was used for both pretest and post test. The observation schedules were filled by trained research assistants (BScN Interns) or enumerators to both the study and control groups.
Written informed consent was obtained from all participants. Ethical clearance was obtained from the University of Nairobi / Kenyatta National Hospital Ethics and Research Committee. Confidentiality, dignity, respect and participants rights were respected. Participation was voluntary with participants reserving their right to withdraw participation at any stage of the study. As such, the rights of participants were not compromised.
The data was cleaned, coded and entered into a computer for analysis using Statistical Package for Social Sciences (SPSS version 20). Both descriptive and inferential statistics was used in analysis. This study adopted a Confidence interval of 95% and a significant level of 0.05.
This study was conducted in 2016 to 2017 and the response rate for this study was around 91% (n=160). At the respondents were Registered Nurses. The results in Table 1 shows that majority of the respondents came from Baringo County Referral Hospital (52%), were of Female gender (73%), were married (76%) and professed Christian faith (99%). The general(for both interventional and control groups) mean age of the respondents is at 36.6 years(SD=7.1) while the specific mean age for the Interventional group, the Baringo County Referral Hospital(BCRH), lower (36.4 years, SD 5.8) than that of the control group, Nandi County Referral Hospital (NCRH), (36.8 years, SD=8.4). The general mean number of practice years (experience) is 12.43(SD=7.06) but the specific for the respondents in Interventional group (BCRH) was lower (11.4 years, SD 5.8) than that of control group (NCRH) (13.5 years, SD=8.2).
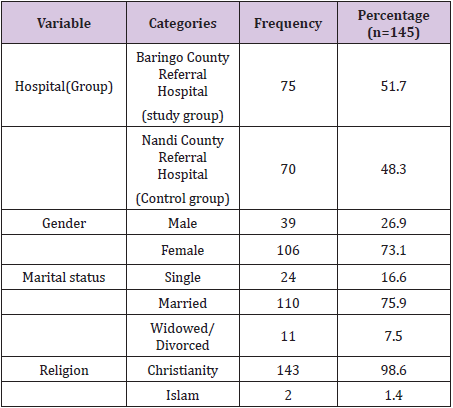
Table 1: The sample of the respondents by some Sociodemographic characteristics.
On the concept of self-reported knowledge of the Standard Precautions, a set of thirteen (13) questionnaire items were presented to the respondents to indicate the best and correct response. The items were later recoded with the correct response getting one (1) point while the incorrect responses were getting zero(0) points. After the recoding we computed new variable that is a sum of all the knowledge scores. The maximum score being thirteen (13) points and the minimum being zero (0) points. The general knowledge score on the Standard Precautions for both study and control groups was 7.6 (SD=1.4) out of the possible 13 or 58.5%.
A paired t-test was conducted to compare the mean knowledge scores in SP in pre-intervention stage and post-intervention stage for the both groups differently. There was a significant difference in the scores for pre-intervention (M=7.5, SD=1.1) and postintervention (M=8.6, SD=0.9); t (74) =-7.686, p < .01 for study group. On the other hand, there was also a significant difference in the scores for pre-intervention (M=7.6, SD=1.7) and postintervention (M=6.4, SD=1.0); t (74) =-5.511, p < .01 for the control group as demonstrated by (Table 2).

Table 2: Knowledge on Standard Precautions before and after the intervention per Group.
An independent t-test was conducted to compare mean scores in knowledge of SP in study group and in control group during the pos-interventional stage. There was a significant differences in the means scores in knowledge for study group (M=8.6, SD=0.9) and control group (M=6.4, SD=1.0), t(143)=13.932, p < 0.01 as shown in (Table 3). The correct knowledge of the Standard Precaution by items was for most items at-least 75% with exception of handling of sharp exceptions(55.9%), correct knowledge on Personal Protective Equipments (55.2%) and the correct procedure of donning of Personal Protective Equipments (28.30%) as shown by (Figure 2).
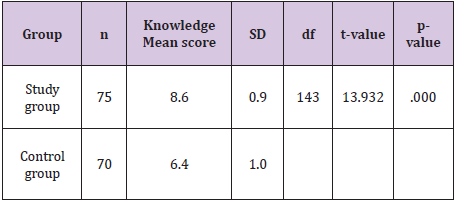
Table 3: Comparison by groups Knowledge of Standard Precautions in post-intervention stage.
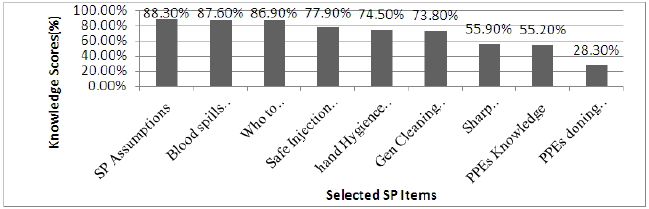
Figure 2: Knowledge Scores (%) of Selected Standard Precautions’ Items.
On the concept of self-reported compliance with the Standard Precautions, a set of eight (8) questionnaire items were presented to the respondents to indicate the best and correct response. The items were later recoded with the correct response getting one(1) point while the incorrect responses were getting zero(0) points. After the recoding we computed new variable that is a sum of all the self-reported compliance scores. The maximum score being eight (8) points and the minimum being zero (0) points. The general self-reported score on the Standard Precautions for both study and control groups was 3.9 (SD=0.9) out of the possible 8 or 48.8%.
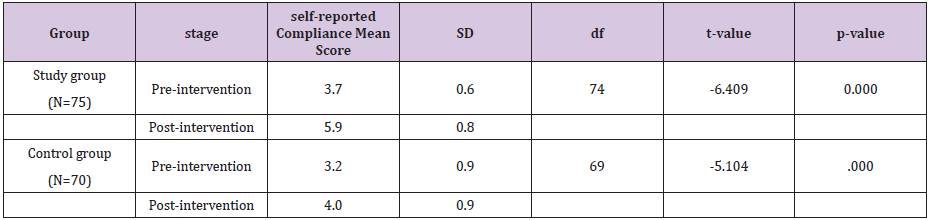
Table 4: Comparison by stage the self-reported Compliance with the Standard Precautions.
A paired t-test was conducted to compare the Mean scores in the self-reported compliance with the Standard Precautions in pre-intervention stage and post-intervention stage. There was a significant difference in the scores for pre-intervention (M=3.7, SD=0.6) and post-intervention (M=5.9, SD=0.8); t (74)=- 6.409, p < .01 in the study group. Comparatively, there was a significant difference in the self-reported compliance scores for pre-intervention (M=3.2, SD=0.9) and post-intervention (M=4.0, SD=0.9); t(69)=-5.104, p < .01 in the control group as shown in (Table 4).
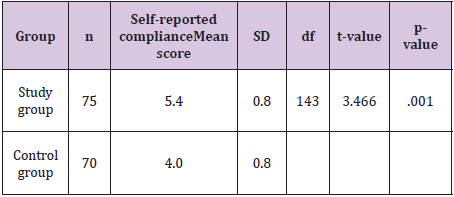
Table 5: Comparison by groups the self- reported compliance with the Standard Precautions in post-intervention stage.
An independent t-test was conducted to compare mean scores in self-reported compliance with the Standard compliance by groups during the pos-interventional stage. There was a significant differences in the means scores in mean scores in self-reported compliance for study group (M=5.4, SD=0.8) and control group (M=4.0, SD=0.8), t(143)=3.466, p < 0.01 as shown in Table 5. The compliance with the Standard Precaution by items was less than 50% in rinsing of sharp injuries with water and soap, hand-washing and gloving when handling sharps as demonstrated by Figure 3. Based on the results of the study on applying Pearson Correlation test, the self-reported knowledge mean scores is not related to Compliance with SP mean scores r=-0.293, p>.05 as shown in Table 6.
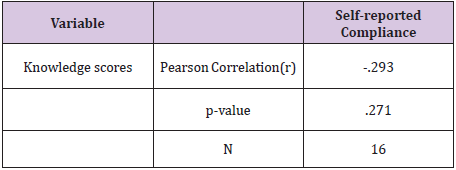
Table 6: The relationship Knowledge and the self reported compliance with the Standard Precautions during the postinterventional stage.
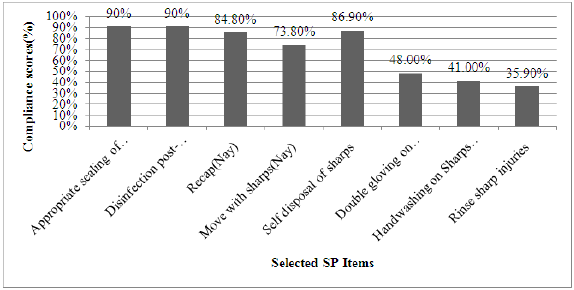
Figure 3: Compliance Scores (%) of Selected SP Items.
Binary Logistic regression was used to determine if knowledge and other socio-demographics predicts compliance with Standard Precautions. This study established that the respondents considered to be knowledgeable in the Standard precautions had higher odds of being compliant with the Standard Precautions compared to those considered not knowledgeable (AOR 1.9, CI1.1-3.6) as shown in Table 7. Other Socio-demographics (such as age, gender, experience, marital status etc) were not significantly associated with compliance with the Standard Precautions (p>0.05).

Table 7: The Self-reported Compliance with the Standard Precautions by Self-reported Knowledge and its Univariate Odds Ratio.
On the concept of observed compliance with the Standard Precautions, a set of ten(10) questionnaire items were presented to the research assistants to indicate whether ‘done always’, ‘done sometimes’ or ‘not done’. The items were later recoded with the correct ‘done always’ being awarded two(2) points, ‘done sometimes’ being awarded one(1) point and ‘not done’ being awarded zero(0) points. After the recoding we computed new variable that is a sum of all the observed Compliance scores. The maximum score being twenty (20). The general observed compliance score on the Standard Precautions for both study and control groups was 12.5 (SD=1.3) out of the possible 20 or 62.7%. A paired t-test was conducted to compare the Mean scores in observed compliance in SP in pre-intervention stage and post-intervention stage for both groups. There was a significant difference in the scores for preintervention (M=12.3, SD=1.4) and post-intervention (M=13.5, SD=0.73); t (29)=-5.286, p < .01 for the study group. Comparatively, there was a significant difference in the scores for pre-intervention (M=11.8, SD=1.1) and post-intervention (M=12.3, SD=1.0); t (29) =-4.267, p < .01 for the control group as demonstrated by Table 8.
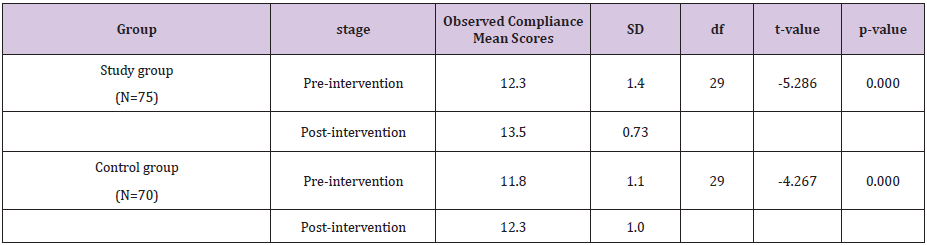
Table 8: Comparison by stage the observed Compliance with the Standard Precaution.
An independent t-test was conducted to compare mean scores in observed compliance with the Standard Compliance in study group and in control group during the pos-interventional stage. There was a significant differences in means scores in self-reported compliance for interventional group (M=13.4, SD=0.7) and control group (M=12.3, SD=0.9), t (58)= 7.350, p < 0.01 as shown in Table 9.
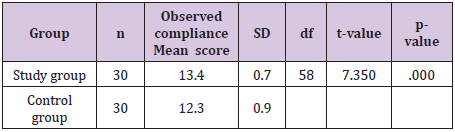
Table 9: Comparison by groups the observed compliance with the Standard Precautions in post-intervention stage.
The general knowledge scores on the Standard Precautions was 58.5% which is lower than knowledge of health workers from Nigeria, Moroco, Jordan, Asia and the United States of America of at-least 75% as documented by several cross-sectional studies on the Standard precautions [3,8-11]. This study also demonstrated a significant positive change of +8.5% in knowledge score after an educational intervention to the study group from 57.7% to 66.2%. This finding corresponds with an interventional study on the subject of the Standard precaution knowledge of both nursing and medical students in Italy [12].
Similar findings of improving knowledge scores (from 79%- 95%) upon an educational intervention to healthcare workers in Zambia were posted by [13]. This may be attributed to the innovative educational intervention applied. On the other hand control group has demonstrated a significant negative change of -9.3% in knowledge after exposure to the baseline questionnaire items only from 58.5% to 49.2%. This finding is worrying and may be related to many un-clarified misconceptions and confusion associated with half-truths arising from the study tool. Thus based on the fore-going, I hereby reject the hypothesis that “There is no significant difference in knowledge scores on the Standard Precautions before and after the intervention”.
The nurses self-reported compliance with the Standard precaution of 48.8% is comparable to that of Nigeria ( around 50%), but grossly lower than of Brazil (around 69%), Asia ( around 80%), Jordan(around 84%) and the United States of America (around 95%), as documented by several cross-sectional studies on the Standard precautions [3,10,11,14-16]. This study demonstrated a significant positive change of +27.5% in compliance scores after an educational intervention to the study group from 46.3% to 73.8%. This finding corresponds with a randomized study done in on the subject of the Standard precaution compliance by the nursing students in China [17]. These attest the fact that knowledge reenforced by this educational intervention enhances compliance and standard practice by mediating on the attitudes.
On the other hand control group has demonstrated a significant positive change of +10.0% in the Standard precautions compliance scores after exposure to the baseline questionnaire items only from 40.0%) to 50.0%. This finding is expected as a study tool post-exposure effect (a confounder) to the study tool. Thus based on the fore-going, I hereby reject the hypothesis that “There is no significant difference in compliance scores on the Standard Precautions before and after the intervention”. This study established that the respondents considered to be knowledgeable in the Standard precautions had higher odds of being compliant with the Standard Precautions compared to those considered not knowledgeable (AOR 1.9, CI1.1-3.6). These findings are in conformity with the results posted by [18] which essentially means the educational program addressed some knowledge gaps identified in the Standard Precautions. However, another study [19] demonstrated a contrary result which infers that there could be other factors other than knowledge that determines of compliance to the Standard Precautions.
The observed compliance score on the Standard Precautions for both study and control groups was 62.7% . This finding are slightly lower than a similar studies applying observational approaches done studying nurses in Italy and reported 65.2% and s similar study in the united States of America that established an observed compliance with the standard precautions of 62% [14,20,21]. This study demonstrated a significant positive change of +6.3% in compliance scores after an educational intervention to the study group from 61.3% to 67.6%. Thus based on the fore-going, I hereby reject the hypothesis that “There is no significant difference in observed compliance scores on the Standard Precautions before and after the intervention”.
The self-reported knowledge scores on the Standard Precautions were 58.5%. The knowledge scores on the Standard Precautions improved from 57.7% to 66.2% in the study group after the educational intervention. The self-reported compliance scores on the Standard Precautions were 48.8%. The self-reported compliance scores on the Standard Precautions improved from 46.3% to 73.8% in the study group after the educational intervention. Compliance was wanting in gloving, hand-washing and management of PIs. The observed compliance scores on the Standard Precautions were 62.7%. The observed compliance scores on the Standard Precautions improved from 61.3% to 67.6% in the study group after the educational intervention. The study also established the knowledge on the Standard precaution was a predictor to its compliance (AOR= 1.9, CI=1.1-3.6).
The study reports increase in the knowledge scores of the Standard Precautions and compliance scores with the Standard Precautions upon application of an educational intervention based on the Social Cognitive Theory together with aspects of Thorndike Principles of Learning. Therefore, it is the submission of this study that both self-efficacy and collective efficacy of healthcare workers on any practical concept are a function of vicarious learning supported with friendly and conducive environment, intrinsic and extrinsic motivation and robust cognitive understanding. Furthermore, appreciating that knowledge not used/practiced decay, it is also the proposal of this study that any educational intervention should be periodic as envisaged by Thorndike Principle of Recency. The healthcare settings should adopt a system whereby in every clinical unit there are credible models (consultants) who was charged with the noble duty of re-enforcing the best practices. This study avers that any concept introduced must also be followed up with clarification of myths/half-truths and re-enforcement of facts to avoid pitfalls of knowledge deficiency and bad practice.

























