info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: August 18, 2017; Published: August 29, 2017
Corresponding author: Marcos E Fernández Cuadros, Rehabilitación y Medicina Física, Hospital Universitario Santa Cristina, Spain
DOI: 10.26717/BJSTR.2017.01.000299
We present the case of a 62 years old man who suffered from a fracture of the astragals ten years ago. Since then he complained of pain while walking and at night. He used to be a taxi driver. The pain has led him to search for any other options since rehabilitation and NSAIDs did not improve his symptoms. He went under a total ankle arthroplasty replacement (Figure 1). After surgery, he was provided a foot ankle orthosis and remained not weight bearing for 6 weeks. After that time, he was let to initiate active exercises of the ankle, progressive weight bearing load and walking with canes. Electromagnetic pulsed fields were provided because of pain and edema. Articular balance was recovered by the second month post-surgery (dorsal flexion of 10º, and plantar flexion of 30º); but pain remained during walking and at night. He was referred to his orthopedic surgeon and anterior-posterior and lateral radiographies of the ankle were ordered. A slight radiolucent sign in anterior-posterior radiography of the tibia component was seen (Figure 2). He continued with Electromagnetic pulsed fields in order to reinforce bone adhesion, and to diminished pain and edema [1,2]. Active exercises were prescribed to maintain articular range of movement. He began to walk again with canes.
Figure 1: Radiographic evaluation at 3 days post-surgery.
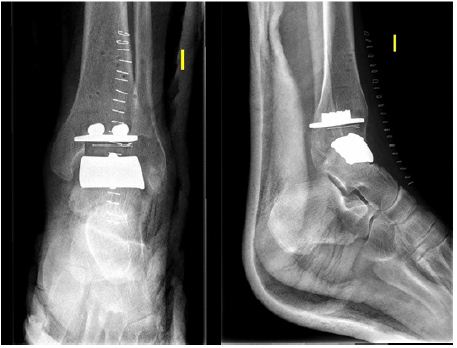
Figure 2: Radiographic evaluation at 3 months postsurgery.

Figure 3: Radiographic evaluation at 6 months postsurgery.
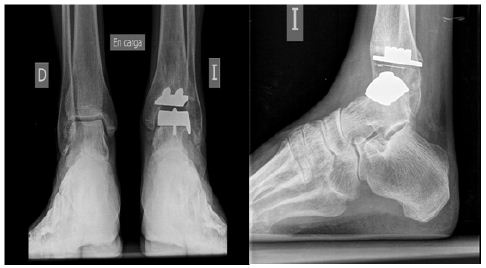
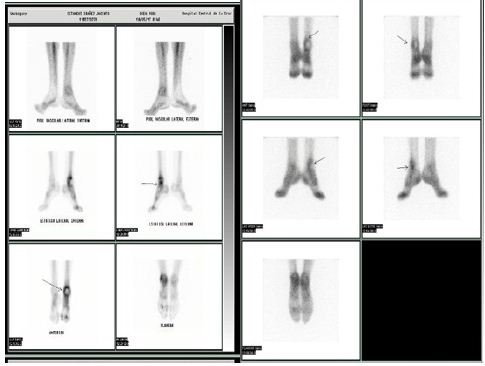
Despite the referred treatment, he continued with pain and diminished active range of movement. At 6 months postsurgery, blood analyses were performed in order to discard a prosthetic infection. Haemogram, CRP and rate of sedimentation were strictly normal. Then a gammagraphy and new weight bearing anterior-posterior radiographies were ordered. A more noticeable radiolucent sign around the tibia component was observed (Figure 3). Gammagraphy with Tecnecium also demonstrated hypercaptation of the tibia component in early and in late phases of the exam (Figure 4); all those evaluations confirmed an aseptic loosening of the arthroplasty.
Figure 4: Gammagraphic evaluation at 6 months postsurgery.
The patient will go through a revision surgery and arthrodesis of the ankle is the suggested treatment option to solve pain.

























