info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: July 23, 2017; Published: August 17, 2017
Corresponding author: Dr. ED Odai, Department of Oral and Maxillofacial Surgery, Room 11, Second Floor, Professor Ejide Dental Complex, University of Benin teaching hospital, Benin-City, Nigeria
DOI: 10.26717/BJSTR.2017.01.000275
Aims and Objectives: To study the prevalence of jaw swellings among maxillofacial surgery patients, the demographics of the patients with jaw swellings and the radiological characteristics of these jaw swellings seen over a period of fifteen years.
Methods: Descriptive retrospective-prospective study. (A retrospective review of cases seen in a ten year period between 1996 and 2005 and a prospective study of cases seen in a five year period between 2006 and 2010). Data of interest were age, gender, anatomic location of the lesions; radiographic characteristics of the lesions- radiolucent, radio-opaque or mixed radiolucent/radio-opaque lesions and the nature of the borders on plain radiographic films.
Results: There were 38,220 attendances to the clinic within the period studied and 1,513 of these presented with maxillofacial swellings, made up of 660 males and 853 females. This is an incidence of 4.0% of maxillofacial swellings among attendants of the maxillofacial clinic. Age range (median) of patients with maxillofacial swelling is 1-87 (30) years. Radiolucency was the most presented radiographic form 1067, radiopaque lesions were 228 and mixed forms were 218 of all the cases of swellings included in the study. Most, 1182 of the lesions are located in the mandible. There were 505 of these lesions in the posterior mandible.
Conclusion: This study concludes that a sizeable number of patients attending to see a maxillofacial surgeon present with a facial swelling, with a slight female predilection and most of the lesions occur in the posterior mandible. Advocacy for purposeful preventive measures and a more equitable distribution of available human and material resources is recommended.
Different pathologies in the maxillofacial region present with swelling. Swellings of the jaw are signs of inflammatory, cystic and neoplastic disorders of the jaw caused by hypertrophy, hyperplasia, neoplasia and pooling of fluids [1]. These may or may not be associated with pain or ulcerations. These swellings have similar clinical features and require further evaluation to differentiate them. Many diagnostic tools exist for diagnostic and therapeutic guidance for surgeons to precisely diagnose types as well as delineate the extent, and location of maxillofacial swellings [2,3]. Among the myriads of cross-sectional imaging modalities developed to evaluation and diagnosis, radiological modality is a first-line and the most important evaluation [4,5] of maxillofacial swellings.
The intra oral radiographs provide very high details of hard tissues (bone and teeth) in the exposed area, but because of the film size lesions larger than 3cm become a challenge to the intra-oral radiography. Extra-oral radiograph therefore are used to evaluate larger lesions and visualize the skull and facial structures [4,5]. The intra-oral and extra-oral radiographic techniques therefore provide useful information in most cases of the lesion is within bone, but this is not so for soft tissue lesions [2,6-8].
Maxillofacial swellings may appear radiolucent, radiopaque or show a mixed radiolucent/radiopaque pattern [4,9]. Unilocular radiolucent lesions with well-defined borders are usually indicative of slow proliferating benign processes. The multilocular lesions with well-defined borders indicate benign but aggressive processes. A radio paque lesion that is well defined represents a benign or inflammatory etiology. In general, lesions with welldefined borders are usually benign, whereas lesions with ill-defined borders invariably are suggestive of aggressive, inflammatory or neo plastic processes. Mixed radiolucent-radiopaque lesions can be due to inflammatory, metabolic conditions, fibro-osseous lesions, or less commonly, malignant processes [1,3,4,9].
The patients’ demographics, history, chair side findings and an analytical approach to plain radiographic investigations will help the surgeon to narrow down their differential diagnosis [2,7,8]. Records of pattern of the clinico-radiological presentations of maxillofacial swellings are not readily available this study therefore presents a documentation of the prevalence of maxillofacial swellings among maxillofacial surgery patients, the demographics of the patients with maxillofacial swellings and the radiological characteristics of these swellings encountered in a Maxillofacial Surgery outpatient clinic located in Benin-City over a fifteen year period.
This study was designed as a descriptive retrospectiveprospective study.
All patients presenting with maxillofacial swellings within the study period whose radiographs and case history would be retrieved from 1996 to 2005 were studied retrospectively. Those seen and evaluated in the out-patient clinic from 2006 to 2010 with appropriate plain extra-oral radiographs were included in the study prospectively.
Case histories and particulars were extracted from case notes, radiographic films and log books over a ten-year period 1996- 2010 (for those studied retrospectively). Oral interview, chair-side evaluation and examination of plain extra oral radiographs were the methods of data collection prospectively from 2006-2010. Data of interest were age, sex, sites of lesions, clinical and radiological presentations of jaw swellings seen. The nature and site of the lesion on a plain radiograph were studied by a Radiologist and a Maxillofacial Surgeon, using plain radiographs and viewing box. The findings were agreed upon, by both examiners. Availability of all data of interest in the case notes and agreement on the nature and site of the lesion on a plain radiograph was a criteria for inclusion. All cases with incomplete data of interest in the case notes and/ or any disagreement on the nature and site of the lesion on a plain radiograph by a specialist Maxillofacial Surgeon and a Radiologist were excluded from the study.
Classification of the lesion were based on the relative density of the lesion with the adjacent bone and recorded as radiolucent, radiopaque or a mixed appearance. The locations of the swellings were recorded as mandibular or maxillary. These were further divided into anterior segment (incisors and canine region), posterior segment (premolar and molar region, or spanning anterio-posterior (involving the incisors, canine, premolar and molar regions). The findings were subjected to simple descriptive analysis and presented as cross-tabulations, frequency distributions and percentages. The study was approved by the ethics committee of the College of Medical Sciences, University of Benin, Benin-City, Edo State.
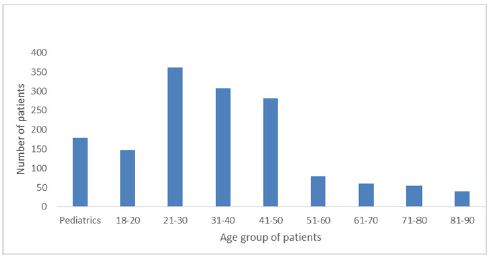
The Maxillofacial Surgical clinic has a total of 38,220 attendances during the period studied. There were 1,513 persons presenting with maxillofacial swellings, which is an incidence of 4.0% for maxillofacial swellings. Age range (median) of patients with maxillofacial swelling is 1-87 (30) years. There were 853 (56.4%) females and 660 (43.6%) males (Figure 1). Whereas 740 presented with swelling alone, 327 presented with swelling and pain while 245 presented with swelling, pain and ulceration. The mandible was the site of 1,182 (78.1%) of these swellings while 331 (21.9%) were located in the maxilla/mid face. The most affected segment was the posterior mandible, with 505 (33.4%) of the swellings and the least affected segment was the anterior maxilla with 68 (4.5%) of all the swellings. There were 358 (25.5%) swellings spanning through the anterior and posterior aspects of the mandible (Figure 2).
Figure 1: Distribution of patient from 1996 to 2010.
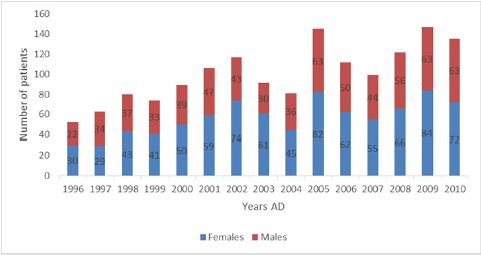
Figure 2: Age distribution of patients.
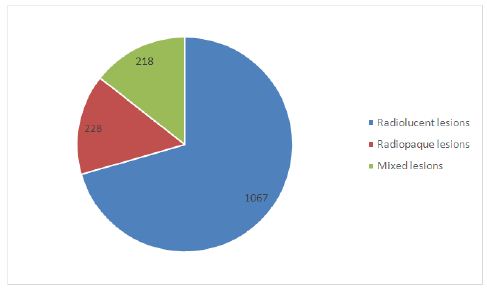
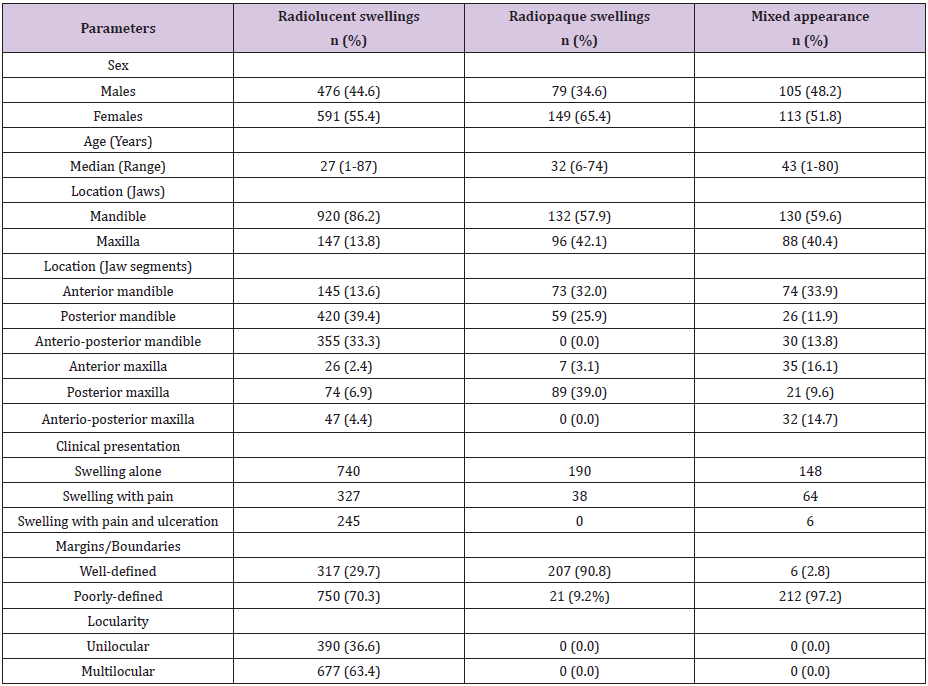
Radiolucent lesions were the commonest radiologic pattern, representing 1067 (70.5%) of all the swellings. The next were mixed radiolucent-radiopaque lesions 228 (15.1%) and the least were radiopaque lesions 218 (14.4%) almost equaling the radiolucentradiopaque lesions. Regards locularity of the radiolucent swellings, 390 (36.6%) were unilocular while 677 (63.4%) were multilocular. Considering the margins of the radiolucent swellings, 317 (29.7%) were well defined whereas while 750 (70.3%) were poorly defined. Whereas 207 (90.8%) of radiopaque lesions had well-defined margins, 21 (9.2%) presented with margins that were not well defined (Figure 3). The mixed radiolucent-radiopaque lesions presented 212 (97.2%) poorly defined margins and only 6 (9.2%) were said to have well-defined margins.
Figure 3:Radiographic presentation of the maxillofacial lesions.
The importance of obtaining relevant case history, undertaking sound physical examinations at the chair-side and correlation with radiological findings to making a diagnosis can-not be over emphasized. This has been stressed from time immemorial to generations of clinicians. This study described the clinic-radiologic findings in patients presenting with hard tissue swellings in a tertiary center. The total number of hard tissue swelling in this study was 1,513. This is higher 638 jaw swellings were recorded in a 22-year study period by Lasisi et al. [10] in 2013 at the University College Hospital, Ibadan. But like the study of Lasisi et al. [10] the incidence peaked in the third decade and deceased till the ninth decade [10]. Whereas in this study there were more female involvement, Lasisi and coworkers found a slightly higher male involvement.
Whereas the peak incidence of swelling in this present study is in the third decade of life, Monterio et al. [11], in 2005 working on odonto genic cyst, in Brazil discovered a peak in the fourth decade [11]. Further comparison with the work of Lasisi et al showed a similarity of most swelling occurring in the posterior mandible. Mullapudi et al. [12] found 77 cases over a study period of nine years with a slight male predilection, most of the swellings occurred in the posterior mandible like in this present study. The grossly higher number of swelling may not necessarily represent a higher incidence of swelling within the population, but likely due to the face that few centers are available in the West African suburb are endowed with the facility and expertise to manage these swellings. Until recently, the center of this present study was the only center with specialist Maxillofacial Surgeons in the South-South and South-East geopolitical zones of Nigeria, therefore there tends to be ‘crowding’ of cases around this study center and the other few centers elsewhere in the country where the manpower and facilities are available following referrals from the scanty and poorly equipped primary healthcare and secondary health facilities. These referrals almost always come late and contain scanty information [13], further slowing down the process of initiation of appropriate definitive care. Swelling pain and ulceration noted may be evidence of these late referrals resulting from pressure effects and declining nutritional status of the affected individuals.
In terms of lucency, boundary definitions and locularity; most of the lesions were radiolucent, presented poorly defined boundaries and showed multilocularity (Table 1). Acute osteomyelitis, primary bone neoplasm, lytic metastasis and direct tumor extensions will be appropriate differentials. Ameloblastoma, odontogenic myxoma and pindborg tumor are further considerations following the involvement of posterior mandible, while odontogenic keratocyst, central hemangiomas are considered when there is no site predilection [14].
Table 1: Clinical-radiological characteristic distribution of maxillofacial hard tissue swellings.
The authors conclude from findings that most swellings seen in West African suburb are in the advanced stage and massive. This in conjunction with the associated nutritional challenges are predictors of poor treatment outcome following intervention. Therefore advocacy for purposeful preventive measures and a more equitable distribution of available human and material resources is recommended.
This manuscript was presented at the first annual scientific conference of the School of Dentistry, College of Medical Sciences, University of Benin, Benin-City Edo State, Nigeria.

























