info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: July 22, 2017; Published: August 07, 2017
Corresponding author: Denis Landaverde, Medical Oncologist, Department of Hematology and Oncology, Hospital Mexico, University of Costa Rica, Mexico
DOI: 10.26717/BJSTR.2017.01.000257
Alveolar soft-part sarcoma is a rare malignant entity with poor prognosis. Chemotherapy has limited activity in this type of sarcoma, we describe here the outcomes of the first case documented in our Institution with metastatic disease, treated exclusively with sunitinib.
Keywords: Alveolar Sarcoma; Sunitnib; Costa Rica
Soft-tissue sarcomas (STS) constitute an uncommon and heterogeneous group of tumors of mesenchymal origin, they share several clinical and pathological features and are usually considered as a group for diagnostic and therapeutic purposes, with the exception of specific particularities of some subtypes [1]. Alveolar soft‐part sarcoma (ASPS) is a rare, distinctive sarcoma, typically occurring in young patients. Although it displays a relatively indolent clinical course, the ultimate prognosis is poor and is often characterized by late metastases [2]. In advanced cases, with multiple metastatic involvement and recurrent cases, only palliative treatment is preferred due to its bad prognosis [3].We describe our experience treating a patients with ASPS with metastatic disease using tyrosine kinase inhibitor (sunitinib) with an outstanding survival and quality of life.
This 23-year-old man with unremarkable past medical history was seen in our clinic with a history of 2 years of increasing rectal pain associated with swelling in his right leg, and subsequently rectal bleeding with mild diarrhea. On physical examination he was found to have a very important skin in duration besides the anus, and at the digital rectal examination a 5cm mass was found at the anal verge.
Figure 1: Alveolar soft-part sarcoma hematoxilyn-eosin staining. Nest of cells, composed of large polygonal cells.
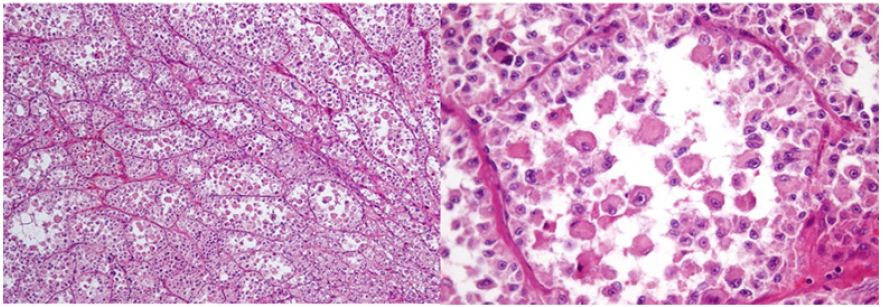
Figure 2:PAS staining, at 40X.
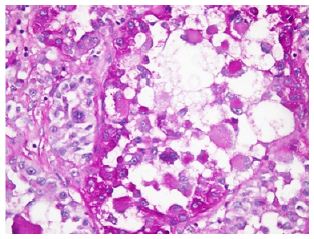
A Thorax-Abdomen and Pelvis CT Scan was performed, and showed: Many pulmonary nodules distributed diffusely with diameters up to 25 mm, compatible with metastatic disease. And also was reported a solid, heterogeneous pelvic mass with well defined borders, approximately 75 mm in maximum diameter, with gas present inside suggesting a fistulous process, with infiltration of the anal canal, as well as the anus elevator muscle in its left portion. Colonoscopy showed an indurated lesion in the perianal region. A biopsy of the lesion was taken in the operating room. The biopsy showed a malignant neoplasm with well defined nests of cells separated by fibrous stroma, composed of large polygonal cells with prominent nucleoli, with alveolar patter tumor cells. Overall features were suggestive of ASPS. Many of the cells were periodic acid Schiff (PAS)–positive. The cells were negative for pancytokeratin, chromogranin, synaptophysin, PLAP, EMA, myoglobin, myogenin, caldesmon, S-100, melan A, CD34, Factor VIII y LCA. The cells were strongly positive for desmin and actin (focally) (Figures 1 & 2).
Because the patient was diagnosed with a stage IV ASPS the case was discussed at the multidisciplinary tumor board, and a tyrosine kinase inhibitor was recommended; in this case, oral sunitinib was started at a dose of 50 mg daily 4 weeks on2 weeks off.
The patient still on sunitinib treatment, he has at this time 3 years and 6 months with no evidence of progression. During the first year of treatment CT Scans showed a reduction of the number and size of the pulmonary nodules, as well as the pelvic disease of about 50% (partial response). At the end of the first year of treatment, a bone scan showed 2 new lesions: Right iliac bone and body of L3 (considered new lesions). Taking into account that the patient had response in lungs and pelvic disease, the new lesions could be considered “oligo-progression” we decided to continue the TKI and give palliative external radiotherapy to bone lesions. (20Gy). Two years after this therapy, the patient continues with stable disease. He has an outstanding quality of life really, with no important side effects and actually he got married recently.
Sunitinib was well tolerated by the patient. The side effects presented were: hair color change and hypothyroidism (the patient is receiving thyroid hormone supplementation).
ASPS is a rare tumor and accounts for 0.5–0.9% of all soft tissue sarcomas [4]. ASPS comprise only 1% of all soft tissue sarcomas [5]. The tumor typically occurs in the deep soft tissues, most often in the buttock and thigh, with a smaller number of cases at other softtissue locations such as the arm, chest and retroperitoneal tissues [6]. Studies on the large series from the MD Anderson Cancer Center, Texas, USA, found a 5‐year disease‐free survival of 71% in patients presenting with localized disease as compared with only 20% in patients presenting with metastases [7]. ASPS are characterized by uniform, organoid nests of polygonal tumor cells, separated by fibro vascular septa and delicate capillary‐sized vascular channels. In these nests there is prominent cellular dyscohesion, leading to the distinctive pseudo alveolar pattern for which it is named. A characteristic finding is the presence of periodic acid‐Schiffpositive [8]. Immuno histo chemical analysis played a limited part in the diagnosis of ASPS. Lung metastasis are very common (42– 65%) but also brain and bone metastasis have been described. The treatment of ASPS is surgery (when the disease is localizaed), but in the metastatic setting, the activity of antiangiogenic agents such as INF-a [9] bevacizumab [10], sunitinib [11], and cediranib [12] have been used in ASPS.

























