info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: July 22, 2017; Published: August 07, 2017
Corresponding author: Andre Wilson Machado, DDS, MS, PhD, Associate Professor, Section of Orthodontics, School of Dentistry, Av. Araújo Pinho, 62, 7ºandar, Federal University of Bahia (UFBA), Salvador/BA, Cep: 40.110-040, Brazil
DOI: 10.26717/BJSTR.2017.01.000256
The terminology “serial extraction” in Orthodontics was first described in the late 1920’s when Kjellgren [1] decided to plan the extraction of certain deciduous and permanent teeth at early stages of the dentition development. Since the extractions are under taken at the transitional dentition. This type of treatment is defined as “Early Treatment” in Orthodontics [2]. The main indication for this treatment approach is for patients with severe crowding caused by tooth size arch discrepancies [3,4]. In other words, when maxillary and/or mandibular arches cannot accommodate teeth, extraction becomes an interesting option.
Although this treatment option has been used for almost a century in the contemporary orthodontics it’s indication is very specific. Since it’s an irreversible approach (permanent teeth are early extracted) the clinician should carefully diagnosis the case before selecting this option. In addition, as time passed by, orthodontics specialty has dramatically evolved and developed several options to gain space instead of extracting teeth. On the other hand, the idea to early extract permanent teeth continues to be an interesting treatment option in clinical orthodontics mainly in severely crowded patients. The aim of this paper is to present a case report of a ten-year-old male patient who presented severe crowding and treatment option was to extract four first premolars at early stages of the dentition development.
A ten-year-old female with no notable medical history presented to my orthodontic clinic with the chief complaint, as reported by her mother that she “I have some spacing in my front teeth”. The intraoral examination showed that the patient was in the final phase of the transitional dentition with a Class I molar relationship, over jet and over jet bite within normal limits and a tooth-size discrepancy of 11 mm in the mandibular arch and 13 mm in the maxillary arch (Figure 1).
Figure 1: Transitional dentition with a Class I molar relationship, over jet and over jet bite within normal limits and a tooth-size discrepancy of 11 mm in the mandibular arch and 13 mm in the maxillary arch.

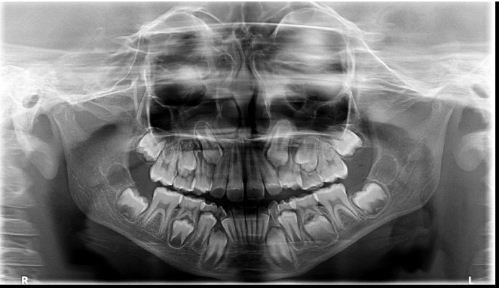
An analysis of the panoramic radiograph indicated the presence of all permanent teeth and the most important finding was that the maxillary canines were positioned very high in the alveolar bone close the lateral incisors apexes (Figure 2). Interceptive orthodontic treatment was planned to correct the crowding by means of permanent teeth extraction. After discussing the advantages and disadvantages of this treatment with the parents, patient was referred for extraction of four first premolars.
Figure 2:The maxillary canines were positioned very high in the alveolar bone close the lateral incisors apexes.
After 11 months, favorable results were achieved but the maxillary right canine and mandibular left second premolar were still erupting (Figure 3). After another 19 months all permanent teeth have erupted and occlusion was very acceptable. Both canines and molars were in Class I, over jet and overbite were within normal limits and dental alignment and leveling were also very acceptable (Figure 4). In this case report a second phase with fixed appliance was not necessary. Although the results achieved in the early treatment undertaken did not fulfill all ideal occlusal standards,function was found to be adequate and aesthetics was considered satisfactory by both the parents and the patient, who chose not to undergo the second treatment phase. Some authors claim that only a small percentage of cases are actually solved with interceptive orthodontics alone, while the majority require a second phase treatment [5]. Ultimately, when diagnosis and early treatment are properly carried out excellent results can be achieved, which corroborates this case report [6].
Figure 3:The maxillary right canine and mandibular left second premolar were still erupting.

Figure 4:Overjet and overbite were within normal limits and dental alignment and leveling were also very acceptable.
Finally an interesting question arises: why extract premolars at early stages? Why not wait until the permanent dentition to take this decision? A recent systematic review [7] comparing the early and late time for premolar extraction in order to correct dental crowding has brought interesting results. It seems that early treatment displays two favorable outcomes such as less relapse and reduced active treatment time when comparing to late treatment. In addition to those advantages, a second phase may not be even necessary as demonstrated in our case report.
Although early premolar extraction in Orthodontics is not a common treatment option when very well indicated it can renders acceptable clinical results.

























