info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map
Received: June 30, 2017; Published: July 12, 2017
Corresponding author: MJ Adeniyi, Department of Physiology, University of Benin, Benin City, Nigeria
DOI: 10.26717/BJSTR.2017.01.000182
Numerous studies have documented the adverse effects of occupational hazards on respiratory functions. The present study hypothesized that: Peak Expiratory Flow Rate (PEFR) of Nigerian premenopausal sanitary workers was neither affected by standing nor sitting: and that neither standing nor sitting PEFR had relationship with Systolic Blood pressure (SBP), Diastolic Blood Pressure (DBP), Mean Arterial Pressure, Body Mass Index (BMI), weight, height and age. In order to test these hypotheses, a population of 48 premenopausal professionals consisting of 24 sanitary workers and 24 teachers were selected after satisfying the inclusion criteria. Measurements were obtained using Wright Flow Meter, Meter Rule, Weighing scale and Sphygmomanometer. The result of the study indicated that the PEFR of the sanitary workers were significantly reduced (P< 0.05) during standing and sitting. Moreover, despite the significant decrease (P<0.05) in SBP, DBP, MAP, BMI and Weight of sanitary workers, only sitting PEFR showed a correlation (r= -0.478, P<0.05) with BMI. Therefore, we concluded that there was postural difference in PEFR of Nigerian female sanitary workers and sitting PEFR related inversely with BMI.
Keywords: Peak Expiratory Flow Rate; Sanitary workers; Mean Arterial Pressure; Body Mass Index
Abbreviations: PEFR: Peak Expiratory Flow Rate; SBP: Systolic Blood pressure; DBP: Diastolic Blood Pressure; BMI: Body Mass Index; FEV: Forced Expiratory Volume; MAP: Mean Arterial Pressure; PEFR: Peak Expiratory Flow Rate
Report from Information Nigeria (2012) revealed that about 200 Nigerians suffer occupational hazard daily. Sanitary work is one of the occupations involving exposure to environmental pollutants. Dusts, fumes and other air borne pollutants are known in scientific consensus to affect physiological functions. For instance, Praveen et al. [1] indicated that people exposed to different dose and frequency of dust exhibited increased amplitudes of QRS and T waves, longer PR and ST segments and high Systolic Blood Pressure, Diastolic Blood Pressure and Mean Arterial Blood Pressure. The reports of American Heart Association [2] also corroborated Praveen’s findings. Also, body weight and Body Mass Index were reported to be affected by exposure to airborne pollutants [3,4]. The introduction of Flow meter by Martin Wright eased the determination of the effect of exposure to airborne pollutants on respiratory function and Peak Expiratory Flow Rate [5]. Studies have documented that Peak Expiratory Flow Rate, a measure of speed of expiration, is decreased by doses and frequency of dust exposure (Meo 2004) [6]. Studies showed that wood workers were characterized by low Peak Expiratory Flow Rate (Meo 2004) [6,7]. Noor et al. [8] found that Timed forced expiratory volume (FEV1) which is often considered a surrogate of Peak Expiratory Flow Rate was low in people exposed to dust. In a similar vein, Zedeke et al. [9] and Shobana et al. [10] reported low Peak Expiratory Flow Rate in workers exposed to dust. Abou-Taleb et al. [11] and Rafnsson et al. [12] stated that prolonged exposure to cement dust can lead to impairment of lung function. In Nigeria, cement factory workers were shown to have low Peak Expiratory Flow Rate (Douglas and Alasia 2012).
Besides airborne pollutants, the position of the body can affect Peak Expiratory Flow Rate in healthy individuals. PEFR taken in adult female during standing was higher than the lying measurement [13-16]. On the contrary, at least a study has shown posture does not affect Peak Expiratory Flow Rate in healthy individuals [17]. Preponderance of evidence suggests that dust exposure affects cardiovascular and respiratory functions (Douglas and Alasia 2012) [1,10]. Also, there are reports on the effect of posture on respiratory function (Silva and Kumar 2015) [16]. However, there is no specific study in which the effect of posture on Peak Expiratory Flow Rate and how the postural Peak Expiratory Flow Rate relates with cardiovascular and anthropometric parameters of Nigerian premenopausal sanitary workers have been done. Therefore, the study was designed to investigate the effect of posture on Peak Expiratory Flow Rate and how the postural Peak Expiratory Flow Rate relates with cardiovascular and anthropometric parameters of Nigerian premenopausal sanitary workers.
The study was conducted on professional premenopausal women. They were categorized into control and experimental groups. While the control group comprised of 24 teachers with at least 7 years work experience, the experimental group consisted of 24 sanitary workers with at least 7 years of work experience. Both the sanitary workers and teachers work five times in a week.
The work was carried out in Ilorin west local government area, Ilorin, Nigeria in February. The area was chosen based on its large population density and the fact that no similar study has been done in the area.
100 female teachers and sanitary workers between 35-50years of age were accommodated into control and experimental groups respectively. Written consent was gotten from each participant and a well-structured questionnaire was administered to rule out those with medical history of respiratory diseases, cardiovascular diseases, metabolic diseases or anatomical deformities. Physical examinations were also done and those that were not medically fit were disqualified. After the screening, 48 women consisting of 24 teachers and 24 sanitary workers technically qualified for the study.
Blood Pressure was measured using digital blood pressure monitor. In sitting position, an occluding cuff was wrapped around the arm and both systolic and diastolic blood pressure was obtained respectively as an average of three consecutive readings. Mean Arterial Pressure (MAP) was gotten using the formulary MAP= 1/3(Systolic pressure-Diastolic pressure) + Diastolic pressure Peak Expiratory Flow Rate (PEFR) was measured using Wright Peak Flow Meter. Each subject was instructed to take a deep inhalation. With the nostrils closed to avoid escape of air and the mouthpiece of the flow meter in the mouth, each subject was asked to exhale forcefully. The procedure was done thrice and the highest recording was chosen. PEFR was done for each subject in sitting position and then (after 1 hour) in standing position.
Weighing scale (Hanson China) was used to measure the body weight in Kg. Each subject was asked to stand upright with no shoes nor scarf. Height was measured in cm using meter rule.
Body Mass Index = body weight (kg)/height (m2).
Data are expressed as mean ± standard error of mean and significant difference was analyzed using unpaired T-test. Significant level was accepted at P<0.05. Linear Regression Lines were used to show the relationships between the parameters.
(Table 1) (Figures 1-3).
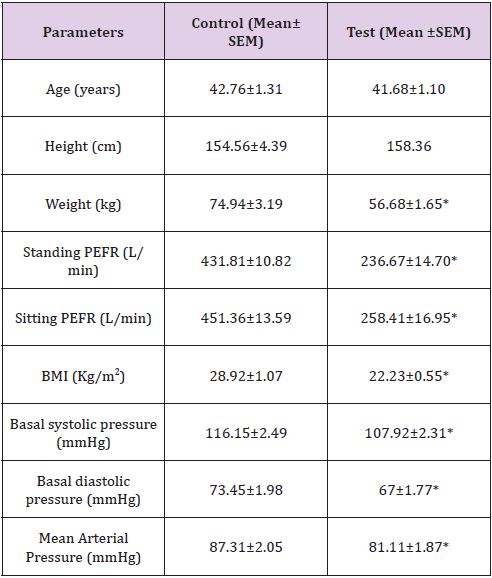
Table 1: Comparison of Parameters.
*significant difference (P<0.05) from control
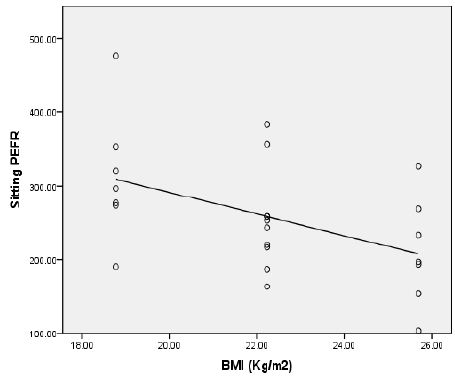
Figure 1: Relationship between sitting PEFR and BMI of sanitary workers (r= -0.478, P<0.05).
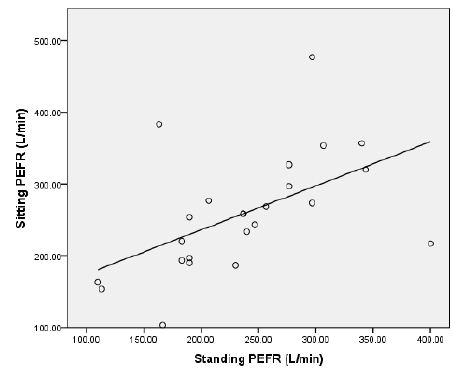
Figure 2: Relationship between standing PEFR and sitting PEFR of sanitary workers (r= 0.533, P<0.05).
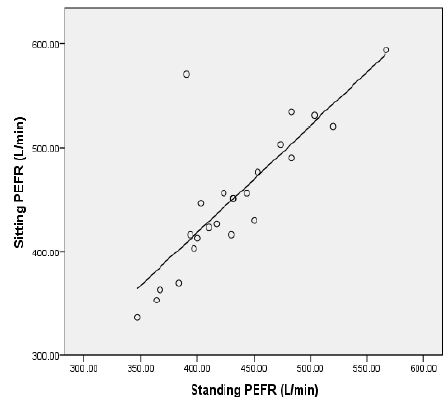
Figure 3: Relationship between standing PEFR and sitting PEFR of teachers (r= 0.813, P<0.05).
Apart from age, sex, height, menstrual cycle and pregnancy, exposure to dust and posture affect cardio-respiratory indices [13,18-20]. The present study investigated the effect of posture on Peak Expiratory Flow Rate of some professional premenopausal women exposed regularly to environmental pollutants and how their postural Peak Expiratory Flow Rate related with cardiovascular and anthropometric indices. The low PEFR observed in sanitary workers during standing and sitting positions in this study concurred with the findings of most studies [9,16] (Jyoth and Kumar 2015). During upright position, due to gravity, the diaphragm and abdominal contents are lowered, resulting in increased superior inferior diameter of the thoracic cavity and increased lung volume. Since the higher the lung volume, the more the PEFR, in sanitary worker, the reduction in PEFR may be due to decrease in lung volume.
Although, the respiratory system is fortified with mechanisms that help in clearing the airway [21], long term exposure to dust may also increase resistance of airway thereby limiting the speed of airflow. We observed a strong positive correlation between sitting and standing PEFR of sanitary workers and teachers. Gravity may be responsible for this association. During standing and sitting (without leaning against chair), despite the fact that gravitational effect is reduced in the latter, the lungs share the same anatomical position [21]. Contrary to the findings of most studies [1,2], the systolic blood pressure, diastolic blood pressure and mean arterial blood pressure were lower in sanitary workers than teachers. Although, there are no sufficient convincing physiological mechanisms that justify rise in blood pressure in people exposed to dust, we suggest that decrease in compliance of the lungs may limit venous return and cardiac output. Decreased venous return and cardiac output decrease systolic blood pressure and diastolic blood pressure [21].
The sanitary workers that participated in this study had over 7 years experience. The effect of such long experience on cardiovascular function is not well understood. We are aware that in both animal and human studies, exposure to airborne pollutants may raise blood pressure probably by blunting baroreflex sensitivity [22,23], we are not sure increase in baroreflex sensitivity was responsible for this low blood pressure. Furthermore, in this study, there was insignificant correlation between postural PEFR of sanitary workers and their blood pressure. Body weight is an index of the socio-economic class of people and socioeconomic class is known to affect dietary status and health [24]. Studies have reported that dust exposure caused an increase in body weight and body mass index (Ani et al., 2012: Manjula et al., 2015). In our own case, we obtained a low body mass index in sanitary workers. The low body mass index invariably was due to low body weight. We are convinced that the low body weight may reflect more of the socioeconomic class of the sanitary workers [24,25]. In Nigeria, sanitary work is often performed by semi-illiterate and low income earners [26-32].
We discovered that only sitting PEFR of sanitary workers correlated negatively with their BMI. There was no significant correlation between postural PEFR and either weight or height or age of sanitary workers. The relationship between sitting PEFR of sanitary workers and their BMI indicates that the BMI of the sanitary workers may be used to predict their sitting PEFR In conclusion, the results of this study indicated that there was postural difference in PEFR of Nigerian premenopausal sanitary women and that there was an inverse relationship between their sitting PEFR and their body mass index.

























