 Opinion
OpinionABSTRACT
Abbreviations: AD: Alzheimer’s Disease; EOAD: Early-Onset AD; LOAD: Late-Onset AD; ADL: Activities of Daily Living; MMSE: Mini-Mental State Examination; GDS: Global Deterioration Scale; ICF: International Classification of Functioning
Opinion
Alzheimer’s disease (AD) corresponds to a complex neurodegenerative disorder that leads to a progressive decrease in brain metabolism functionally and morphologically (Deture, et al. [1-3]). Their presentation is progressive and chronic, with a subsequent loss of cognitive function (Justin M Long [3]). AD is the most common form of dementia and may contribute to 60- 70% of cases (WHO [4]). The majority of cases occur after age 65, comprising late-onset AD (LOAD), while cases occurring earlier than age 65 are considerably rarer, constituting less than 5% of all cases and are termed early-onset AD (EOAD) (Alzheimer’s, Long [3,5]). In addition, the risk of AD is 60% to 80% dependent on hereditary factors, with more than 40 genetic risk loci associated with AD already identified (Tanzi [6]). Also, the APOE alleles have the strongest association with the disease (Scheltens, et al. [7,8]). Moreover, in recent years, it is fast becoming one of the most costly, deadly, and burdensome diseases of this century (Scheltens, et al. [5,7]). The most recent data indicate that, by 2050, the prevalence of dementia will double in Europe and triple worldwide, and that estimate is three times higher when based on a biological definition of the disease (Scheltens, et al. [7]). Functionality is conceptualized as the ability of a person to carry out the activities necessary to achieve wellbeing through the interrelation of their fields: biological, psychological (cognitive and affective) and social (Hopper [9]).
Under this definition, the International Classification of Functioning, Disability and Health (ICF) proposes a conceptual framework that establishes a standard language to describe health and its different dimensions (WHO [10]). It was approved by the (WHO [10]), and since then, it has had high applicability in the field of health rehabilitation (Hopper [9]). (Figure 1) lists the three components of this model: body functions and structures, activity and participation. The first component is related to physiological and psychological functions and anatomical elements; the second component refers to the individual execution of tasks and activities; the third component is related to the development of social situations (WHO [10]). Functional impairment is a core symptom of AD (Arrighi, et al. [11,12]). The most precise indicator of functional deterioration is the decrease in the performance of activities of daily living (ADL) (Arrighi, et al. [11,13,14]). A report using ICF has pointed out that activity and participation are restricted to domestic life, self-care and mobility, communication, interaction, and social relations (Muò, et al. [13]). In addition, subjects who appeared more compromised on the Mini-Mental State Examination (MMSE) and Global Deterioration Scale (GDS) showed more significant function impairment, activity limitation, and participation restriction (Muò, et al. [13]).
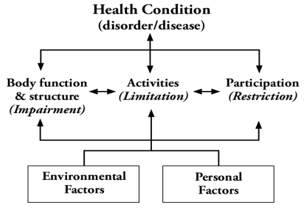
Figure 1: International Classification of Functioning, Disability, and Health (ICF) (WHO 2001).
Executive dysfunction and decreased general measures of cognitive functioning have also been reported to be associated with decreased ability to perform instrumental ADLs (Pereira, et al. [15]). ADLs are affected progressively and hierarchically associated with cognitive decline, but substantial variability persists between individuals and the relative order of affected items (Arrighi, et al. [11]). It has also been pointed out that there are disability profiles with restricted patterns of time use in a variety of domains encompassing both compulsory and discretionary activity, accompanied by a significant increase in a passive activity, such as sleeping during the day or sitting in front of the television (Lomax, et al. [16]). Also, restrictions in the social and environmental contexts of the patient’s life and diminished levels of subjective enjoyment have been associated with their pattern of daily use of time (Hopper, et al. [9,16]). Currently, the ICF consists of 1,424 mutually exclusive categories that, taken together, cover a complete and comprehensive spectrum of human experience and are organized as a hierarchical structure of 4 levels differentiated from least to greatest precision (WHO [17]). The ICF categories are indicated using alphanumeric codes with which it is possible to classify functioning and disability, both at the individual and population levels.
According to this hierarchical structure, the highest-level category (4th) shares the attributes of the lowest level category (1st) to which it belongs. In addition, ICF qualifiers are used to quantify the magnitude of a problem in the different ICF categories, which are mathematically weighted quality descriptors that record the presence or severity of a problem at the bodily, personal, or social level (WHO [10]). Thus, a problem can suppose a deterioration, a limitation or a restriction that can be qualified from 0 (no problem: 0-4%), 1 (slight problem: 5-24%), 2 (moderate problem: 25-49%) , 3 (severe problem: 50-95%) to 4 (total problem: 96- 100%). For their part, environmental factors are quantified with a negative or positive scale that indicates the extent to which an environmental factor acts as a barrier or facilitator (WHO [17]). The ICF is a helpful tool for describing health status in patients with AD since it highlights important aspects of daily life that are not usually considered in activities of daily living scales, such as communication, social relationships, and recreation and leisure (Badarunisa, et al. [9,12,18]).
References
- Deture M A, Dickson D W (2019) The neuropathological diagnosis of Alzheimer’s disease. Molecular Neurodegeneration 14(1): 1-18.
- Dugger B N, Dickson D W (2017) Pathology of Neurodegenerative Diseases. Cold Spring Harbor Perspectives in Biology 9(7).
- Justin M Long, David M Holtzman (2019) Alzheimer Disease: An Update on Pathobiology and Treatment Strategies. Cell 179(2): 312-339.
- (2017) World Health Organization (WHO). Global action plan on the public health response to dementia 2017-2025. Geneva: World Health Organization, p. 27.
- (2020) 2020 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia : The Journal of the Alzheimer’s Association 16(3): 391-460.
- Tanzi R E (2012) The Genetics of Alzheimer Disease. Cold Spring Harbor Perspectives in Medicine 2(10).
- Scheltens P, De Strooper B, Kivipelto M, Holstege H, Chételat G, et al. (2021) Alzheimer’s disease. The Lancet 397(10284): 1577-1590.
- Serrano Pozo A, Das S, Hyman B T (2021) APOE and Alzheimer’s Disease: Advances in Genetics, Pathophysiology, and Therapeutic Approaches. The Lancet Neurology 20(1): 68.
- Hopper T (2007) The ICF and dementia. Seminars in Speech and Language 28(4): 273-282.
- (2001) International Classification of Functioning, Disability and Health (ICF).
- Arrighi H M, Gélinas I, McLaughlin T P, Buchanan J, Gauthier S, et al. (2013) Longitudinal changes in functional disability in Alzheimer’s disease patients 25(6): 929-937.
- Gauthier S, Gélinas I, Gauthier L (1997) Functional disability in Alzheimer’s disease. International Psychogeriatrics 9: 163-165.
- Muò R, Schindler A, Vernero I, Schindler O, Ferrario E, et al. (2009) Alzheimer’s disease-associated disability: An ICF approach 27(23): 1405-1413.
- Yeh Y C, Lin K N, Chen W T, Lin C Y, Chen T Bin, et al. (2011) 31(3): 225-232.
- Pereira F S, Yassuda M S, Oliveira A M, Forlenza O V (2008) Executive dysfunction correlates with impaired functional status in older adults with varying degrees of cognitive impairment. International Psychogeriatrics 20(6): 1104-1115.
- Lomax C L, Brown R G, Howard R J (2004) Measuring disability in patients with neurodegenerative disease using the “Yesterday Interview”. International Journal of Geriatric Psychiatry 19(11): 1058-1064.
- (2013) How to use the ICF A Practical Manual for using the International Classification of Functioning, Disability and Health (ICF) How to use the ICF A Practical Manual for using the International Classification of Functioning, Disability and Health (ICF) Exposure draft for comment.
- Badarunisa M B, Sebastian D, Rangasayee R R, Kala B (2015) ICF-Based Analysis of Communication Disorders in Dementia of Alzheimer’s Type. Dementia and Geriatric Cognitive Disorders Extra 5(3): 459-469.
