 Mini Review
Mini ReviewMini Review
A 73-year-old woman was referred to us for endoscopic biliary drainage of obstructive jaundice due to a pancreatic mass diagnosed by abdominal computed tomography (CT) scan (Figure 1A). Endoscopic Retrograde CholangioPancreatography (ERCP) was performed with CO2 insufflation under general anesthesia. Wire-guided cannulation of the papilla was gently attempted with the long route because of the distorted anatomy of the descending duodenum (Figure 1B) and was suddenly stopped by the anesthesiologist when blood came from the aspiration tube. Withdrawing the duodenoscope, petechial lesions and deep longitudinal actively oozing mucosal tears were seen in the lesser curvature of the stomach from the angulus (Figure 1C) to the gastroesophageal junction, consistent with gastric barotrauma. This gastric “cat scratch” is a rare phenomenon that, following LaPlace’s law, arises when sudden high gaseous pressure leads to increased wall tensions. It occurs in the lesser gastric curvature probably because this part of the stomach has a lower capacity for distension, owing to the lack of mucosal folds and the presence of the gastrohepatic ligament [1]. At the end of the procedure the patient immediately experienced epigastric pain and abdominal distention without any sign of perforation. This is the first case report showing gastric barotrauma during ERCP.
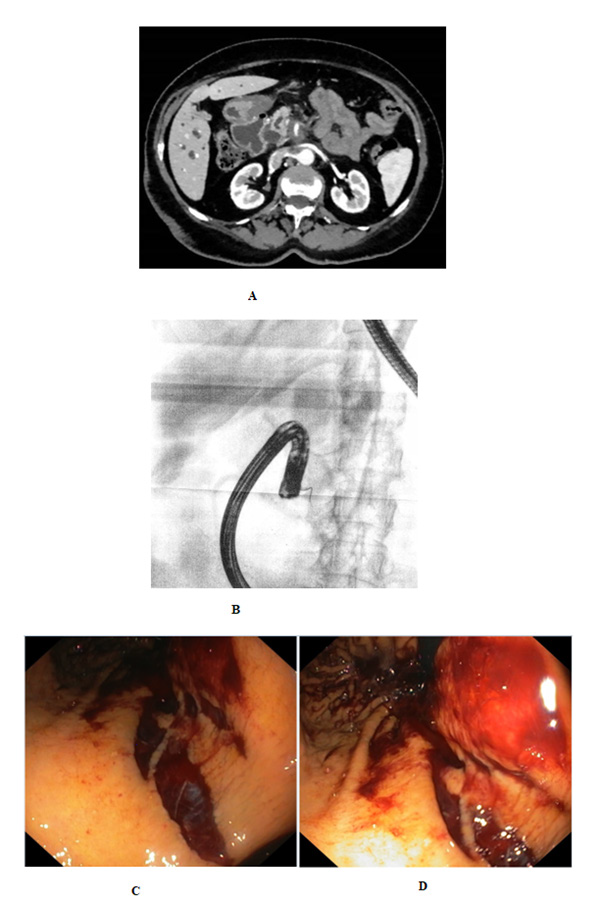
Figure 1:
A. Abdominal computed tomography showing double-duct sign: the combined dilatation of the common bile duct and pancreatic duct, caused by pancreatic mass.
B. Wire-guided cannulation of the papilla with the long route at x-rays.
C. Petechial lesions and deep longitudinal actively oozing mucosal tears in the lesser curvature of the stomach at the angulus and the gastroesophageal junction (Figure D).
Disclosure
All authors disclosed no financial relationships.
References
- Datta S, Adlakha N, Ivanina EA (2016) When the Trauma Comes from Within. American Journal of Gastroenterology 111: 1375.
