 Research Article
Research ArticleSUMMARY
Purpose of the Study: Explore the role of MRI in the diagnosis of Charcot foot in patients with early-stage diabetic osteoarthropathy.
Material and Methods Research: 45 patients (prospectively) with type 2 diabetes and Charcot’s foot were examined in the period 2021-2022 at the RSNPMC of Endocrinology named after Academician Y.Kh. Turakulova, in the department of diabetic foot. All observed patients were divided into 2 groups:
• gr - patients with acute stage of Charcot’s foot with type 2 diabetes - 25 patients,
• gr- patients with subacute Charcot foot - 20 patients,
The control group consisted of 20 individuals with DM 2 without diabetic foot syndrome of the 45 patients, there were 37 men and 8 women. Average age: men was 69.12 years, women - 68.15 years. The duration of type 2 diabetes ranged from 17 to 25 years. Research methods included: biochemical (bilirubin, direct, indirect, lipid spectrum, ALT, AST, PTI, coagulogram, blood sugar, glycated hemoglobin, urea, creatinine, calcium, alkaline phosphatase, parathormone, vitamin D3, blood and instrumental: ECG, MRI foots, dopplerography of the main vessels of the legs, ultrasound of the internal organs, DEXA, fundus.
Research Results
On MRI we found location of bone marrow abnormality (edema shown in fluid sensitive sequences, and reduction of fatty bone marrow shown in T1 sequences). Pattern tends to be periarticular. In all patients were involved several joints and bones (mostly tarso-metatarsal joints and metatarsophalangeal joints). During early-stage Charcot foot, CT does not play an important role for imaging since bone marrow and soft tissue changes can be better visualized using MRI. CT may be used in later-stage Charcot foot for better visualization of bony proliferations and consolidation. Recognizing this disease in early stages prevents a delayed onset of an appropriate therapy and helps minimizing the disability of these patients.
Background
As is known, Charcot neuroarthropathy (CN) is a condition affecting the bones, joints, and soft tissues of the foot and ankle, characterized by inflammation at its earliest stage [1]. The pathogenesis of this condition is not fully understood, but autoantibodies against oxidative post-translational modified collagen have recently been found in NS and diabetic neuropathy, suggesting a possible involvement of autoimmunity [2]. In its most severe form, NS can lead to deformity, ulceration, infection, and amputation. This contributes to significant morbidity and premature mortality and worsens the quality of life of patients [1]. If you start unloading the foot at an early stage, it can prevent the progression of the disease and reduce the frequency of foot deformity [3,4]. A characteristic early manifestation of diabetes is a hot, swollen foot, often with normal radiographs. This is the generally recognized Charcot foot of stage 0 [5-7]. However, the pathology at this stage is not well understood, although magnetic resonance imaging (MRI) has proven useful in detecting reactive, inflammatory bone marrow with or without microfractures before radiological changes become evident [4,8]. If SPECT/CT is not available, CT alone can detect a bone fracture in 59% of patients. Stage 0 Charcot foot has a distinct bone pathology that requires urgent treatment to prevent the progression of stage 1 Eichengoltz Charcot foot [9]. MRI is the best method of diagnosis of suspected early active Charcot disease [10]. This may be crucial, since conventional radiographs can appear normal during very early stage of Charcot disease (Eichenholtz stage 0). Early signs of a Charcot foot in MRI are bone marrow edema and soft tissue edema, joint effusion, and eventually microfractures (subchondral) [11]. During the early stage of Charcot foot, there are no cortical fractures and no gross deformity seen [12]. https://www.ncbi.nlm. nih.gov/pmc/articles/PMC6682845/ - CR2.
Purpose of the Study
Explore the role of MRI in the diagnosis of Charcot foot in patients with early-stage diabetic osteoarthropathy.
Material and Methods Research
45 patients (prospectively) with type 2 diabetes and Charcot’s foot were examined in the period 2021-2022 at the RSNPMC of Endocrinology named after Academician Y.Kh. Turakulova, in the department of diabetic foot. All observed patients were divided into 2 groups:
gr - patients with acute stage of Charcot’s foot with type 2 diabetes - 25 patients.
gr - patients with subacute Charcot foot - 20 patients.
The control group consisted of 20 individuals with DM 2 without diabetic foot syndrome of the 45 patients, there were 37 men and 8 women. Average age: men was 69.12 years, women - 68.15 years. The duration of type 2 diabetes ranged from 17 to 25 years. Research methods included: biochemical (bilirubin, direct, indirect, lipid spectrum, ALT, AST, PTI, coagulogram, blood sugar, glycated hemoglobin, urea, creatinine, calcium, alkaline phosphatase, parathormone, vitamin D3, blood and instrumental: ECG, MRI foots, dopplerography of the main vessels of the legs, ultrasound of the internal organs, DEXA, fundus. Statistical calculations were carried out in the Microsoft Windows software environment using the Microsoft Excel-2007 and Statistica version 6.0, 2003 software packages. The obtained data are shown as M±m, where M is the mean value of the variation series, m is the standard error of the mean value. The significance of differences between independent samples was determined by the method of Mann-Whitney and Student.
Research Results
(Table 1) shows the distribution of patients by sex and age. As can be seen from Table 1, most of the patients were aged 60 to 74 years - 36 (80%), while the number of men was 5 times more. The next step in our research was to study the parameters of carbohydrate metabolism and markers of bone metabolism (Table 2). As can be seen from Table 2, there were significant violations of carbohydrate metabolism in all groups, which indicates the state of decompensation in these patients. 25-hydroxyvitamin D3 levels were lower (12.6±3.3 ng/mL, p<0.001, 11.2±4.2 ng/mL, p<0.001, 10.5±4.1 ng/mL, p <0.001, 11.3±4.8 ng/ml, p<0.001) in sick groups than in the control group (27.2±6.2 ng/ml). The next stage of our work was the study of MRI of the feet in the studied groups of patients (Table 3). On MRI we found location of bone marrow abnormality (edema shown in fluid sensitive sequences, and reduction of fatty bone marrow shown in T1 sequences). Pattern tends to be periarticular. In all patients were involved several joints and bones (mostly tarso-metatarsal joints and metatarsophalangeal joints). During early-stage Charcot foot, CT does not play an important role for imaging since bone marrow and soft tissue changes can be better visualized using MRI. CT may be used in later-stage Charcot foot for better visualization of bony proliferations and consolidation. Recognizing this disease in early stages prevents a delayed onset of an appropriate therapy and helps minimizing the disability of these patients.

Table 1: Distribution of patients by sex and age.

Table 2: Comparative characteristics of parameters of carbohydrate metabolism in patients and markers of bone metabolism by groups.
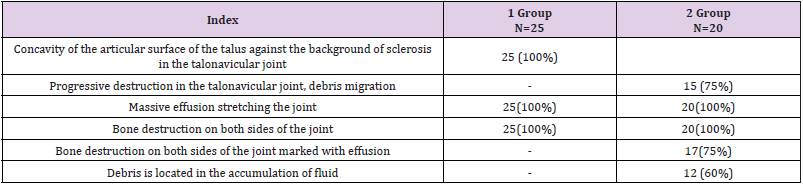
Table 3: Comparative characteristics of foot MRI indicators by groups.
Conclusion
Patients with diabetic foot syndrome complicated by Charcot’s foot are at high risk of 25-hydroxyvitamin D3 and calcium deficiency.
An early symptom on MRI with Charcot foot was the presence of concavity of the articular surface of the talus against the background of sclerosis in the talonavicular joint.
References
- Rogers L C, Frykberg R G, Armstrong D G, Boulton A J M, Edmonds M, et al. (2011) The Charcot Foot in Diabetes. Diabetes Care 34(9): 2123-2129.
- Rizzo P, Pitocco D, Zaccardi F, Di Stasio E, Strollo R, et al. (2016) Autoantibodies to post-translationally modified type I and II 9. collagen in Charcot neuroarthropathy in subjects with type 2 diabetes mellitus. Diabetes Metabolism Res Rev 33(1): e2839.
- Chantelau E (2005) The perils of procrastination: Effects of early vs. delayed detection and treatment of incipient Charcot fracture. Diabetes. Med 22(12): 1707-1712.
- Chantelau E, Poll L W (2006) Evaluation of the Diabetic Charcot Foot by MR Imaging or Plain Radiography - an Observational Study. Exp. Clin. Endocrinol. Diabetes 114(8): 428-431.
- Shibata T, Tada K, Hashizume C (1990) The results of arthrodesis of the ankle for leprotic neuroarthropathy. J Bone Jt Surg Am 72(5): 749-756.
- Sella E J, Barrette C (1999) Staging of Charcot neuroarthropathy along the medial column of the foot in the diabetic patient. J Foot Ankle Surg 38(1): 34-40.
- Ruotolo V, Di Pietro B, Giurato L, Masala S, Meloni M, et al. (2013) A New Natural History of Charcot Foot. Clin Nucl Med 38(7): 506-509.
- Edmonds M E, Petrova N L, Elias D (2005) The earliest magnetic resonance imaging sign of mid-foot Charcot osteoarthropathy is oedema of subchondral (subarticular) bone marrow which needs prompt therapeutic offloading. Diabetes Med 22: 93.
- Raju Ahluwalia, Ahmad Bilal, Nina Petrova, Chris Manu, Prashanth, et al. (2020) The Role of Bone Scintigraphy with SPECT/CT in the Characterization and Early Diagnosis of Stage 0 Charcot Neuroarthropathy. J Clinic Med 9(12): 4123.
- Mautone M, Naidoo P (2015) What the radiologist needs to know about Charcot foot. J Med Imaging Radiat Oncol 59(4): 395-402.
- Ahmadi M E, Morrison W B, Carrino J A, Schweitzer M E, Raikin S M, et al. (2006) Neuropathic arthropathy of the foot with and without superimposed osteomyelitis: MR imaging characteristics. Radiology 238(2): 622-631.
- Ledermann H P, Morrison W B (2005) Differential diagnosis of pedal osteomyelitis and diabetic neuroarthropathy: MR imaging. Semin Musculoskeletal Radiol 9(3): 272-283.
