 Research Article
Research ArticleABSTRACT
In total hip arthroplasty (THA), orthopedic surgeons can determine the stability of the fixed hip stem based on the changes in the hammering sound, which is not a myth. It has been observed through Fourier analysis that the hammering sound changes. This study aimed to check whether it is possible to determine how stable the hip stem is fixed in real-time by collecting hammering sounds in operating rooms. First, a hammering sound analysis system was built, and an application was developed. Next, the analysis system was used to measure the frequencies and levels of hammering sounds along with ambient sounds to review the ideal position for collecting sounds. In all 12 analyzed cases, stem stability was successfully determined in real-time. It was revealed that the analysis system was less likely to fail to detect sounds when sounds were collected at a position near the patient’s head. It is possible to distinguish the voices of the medical staff, a major ambient sound in the operating room, from the hammering sounds. However, it is difficult to distinguish the peak frequencies of produced sounds when surgical instruments are in contact with those of hammering sounds because their frequency ranges are almost the same, and solving this problem is the greatest challenge.
Keywords: Intraoperative Fractures; Total Hip Arthroplasty; Hammering Sound; Fourier Analysis; Peak Frequency
Introduction
Total hip arthroplasty (THA) provides patients with a high level of postoperative satisfaction [1]. However, it has been reported that during surgery, serious intraoperative fractures occur at a rate between 0.4 and 4.9% [2,3]. During surgery, orthopedic surgeons with good clinical experience can determine how stable the hip stem is fixed through the changes in the hammering sound, which is a proven fact. Fourier analysis verified the changes in the hammering sound [4]. It has been revealed that when the stem is fixed into a femur, the peak frequency with the same spectral shape [5-7]. In the engineering field, to check the stability of a bolt, a hammering test was conducted. A hammering test is a procedure for checking the contact of a structure with another. The surfaces of structures, such as bridge girders, piers, and tunnel linings, are hammered to identify their state based on the sound produced. Based on this idea, this theory can be applied to the medical field, focusing on hammering sounds in THA. We have indicated the possibility for surgeons to check how stable the stem is fixed to the femur and predict possible intraoperative fractures [6-8]. In this study, a hammering sound analysis system was built, and an application was developed to check whether it is possible to prevent intraoperative fractures and collect hammering sounds in operating rooms for real-time analysis. A miniaturized analysis system was used to measure the frequencies and of hammering sound levels along with ambient sounds to review the ideal position for collecting sounds.
Materials and Methods
This study was approved by the ethics commission of the organization to which the author belongs (B16-239). The patients were had provided informed consent. Clinical trials were conducted on 12 patients of total hip replacement (eight women and for four men, with a mean age of 70.1 years), conducted at Kitasato University Hospital. The surgery was performed by an orthopedic surgeon specialized in the hip joint with more than 20 years of clinical experience. It was attended by three orthopedic surgeons along with one scrub nurse and one anesthesiologist staying at all times on the foot and head sides of the patients, respectively. The hammering sound analysis system for the hip stem developed by the author et al. consists of a PC, sensor amplifier, and storage scope. The system had a drawback that uses many large instruments [5]. Improvements were made to the system to enable one tablet unit to cover all functions so that the system could be easily carried into the operating rooms. Table 1 lists the development platform for this application. The application was designed to capture hammering sounds produced when the stem is driven into the femur, detect the power spectrum through fast Fourier transformation, determine the maximum peak frequency (hereafter, the peak frequency), and continuously make assessments (see Figure 1). The system determines that the stem has been fixed and provides a warning that further hammering would cause a bone fracture, when the peak frequency stays within a range of ±0.05 kHz three times in a row [5].
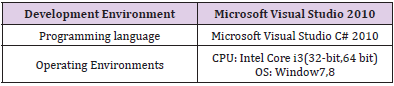
Table 1: Application development environment.
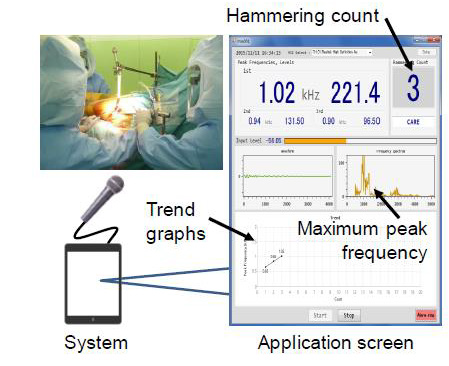
Figure 1: Graphical user interface of the developed system.
The miniaturized hammering analysis system consisted of a Miix 2 8 (a tablet PC) and a directional microphone. This system was used to store the sound source and, at the same time, perform a series of actions-level assessments, frequency measurement, shorttime Fourier analysis, and draw maximum frequency trend graphsto analyze and monitor data in real-time. Sounds were collected with a sampling frequency of 44.1 kHz and aquantization bit rate of 16 bits. The sound collection and analysis started concurrently with the stem driving into the femur, and data were recorded until the operating surgeon finished the stem driving. A review was conducted on the ideal positions at which hammering sounds were collected in the operating rooms. Microphones were placed at four locations: on the right and left sides of the upper- and lower-limbs of the patient (see Figure 2). Each microphone was placed 2 m away from the surgical field to check which location the microphone was less likely to incorrectly detect hammering sounds or to fail to detect any hammering sounds. A KZ-GM1351 digital noise level meter was used to identify the ambient sound in the operating room. At the same time, the analysis system was used to store the sources of ambient sounds, make level assessments, measure frequencies, conduct short-time Fourier analysis, and create a trend graph of maximum frequencies in real time.

Figure 2: Position to collect hammering sound in the operating room.
Results
In the 12 cases analyzed, no intraoperative fracture was predicted, and both the operator based on the sensory determination and analysis system made correct determinations about the stability of the stem. No problem was found immediately after the surgery, and the stability was good for five years in all cases. In all 12 cases, the miniaturized analysis system successfully evaluated stem stability. For the 12 joints, the frequency determined based on hammering sounds was 4.02 ± 2.33 kHz at the time when the stem stability had been obtained. The hammering sound levels for the 12 joints from the start and end of hammering were 7.31 ± 1.91 dB. The relationships between the frequency distributions, levels of the hammering sounds, and ambient sounds during surgery of one of the 12 joints are shown (see Figure 3). The green round plots represent hammering sounds, and the frequency for this joint was 2.82 ± 0.62 kHz with a level of 8.81 ± 2.85 dB. Yellow circles represent the voices of the medical staff. The red triangle plots represent sounds that were not detected by the developed system, which were eight in number. The hammering sounds were detected using a digital noise-level meter. The five x-plots represent the voice of the medical staff that were mistakenly detected as hammering sounds.
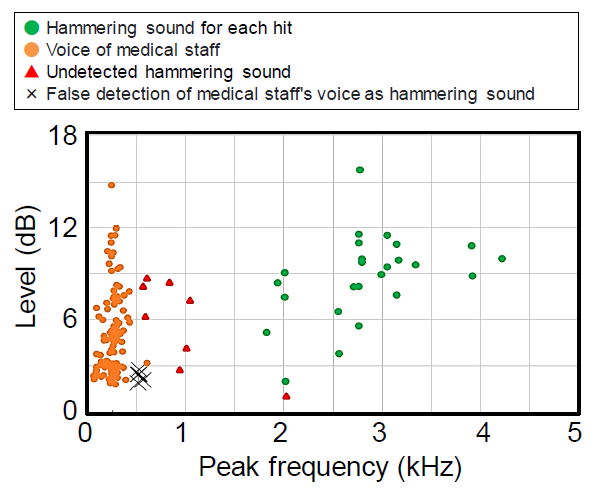
Figure 3: Level and the peak frequency of hammering sound, the voice of medical staff, and undetected hammering sound. Cross is false detection of the medical staff’s voice as a hammering sound.
The microphone on the head side of the patient failed to detect only two sounds, which were the least likely to fail in detecting sounds (see Figure 4). The microphone on the lower limb side of the patient failed to detect nine sound-levels that were below 4 dB. Each microphone on the right and left sides of the patient failed to detect three sounds, the frequencies and levels of which were inconsistent with no particular tendency in the observed characteristics. The results of the measurement of ambient sound in the operating room indicated that the levels of the voices of the medical staff were 8.85 ± 4.70 dB with a frequency of 0.48±0.16 kHz. (Figure 5A) shows one of the 181 voice sounds of the medical staff, which revealed that its level was the highest among the ambient sounds. The sound of the second-highest level was that produced when a surgical instrument is contacted, the level of which was 8.26 ± 6.23 dB with a frequency of 2.71 ± 0.52 kHz (see Figure 5B). The sound produced by surgical instruments had many peak frequencies, with a mean maximum frequency of 3.26 ± 0.99 kHz and a sound level of 2.024 ± 0.95 dB (see Figure 5C).
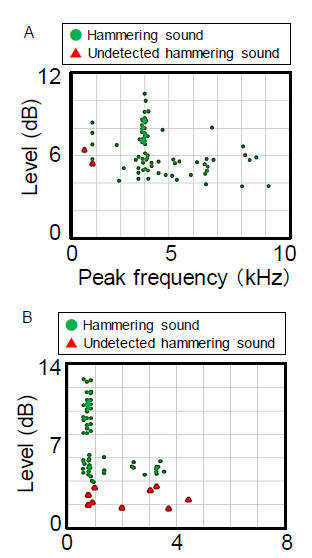
Figure 4:
A) F-P5500.
B) AT9913
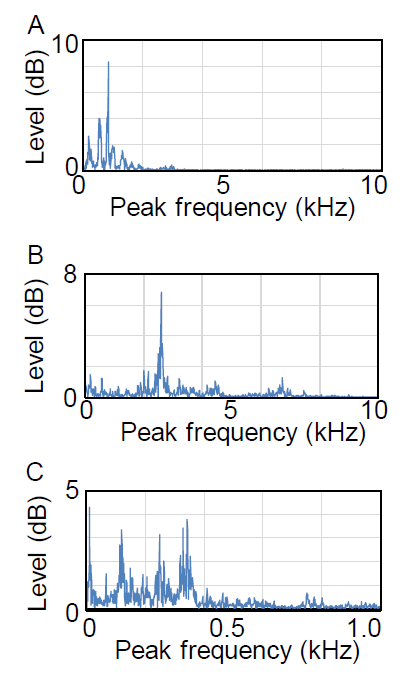
Figure 5: Environmental sounds in the operating room.
A) Voices of surgeons and medical staff.
B) Sound of surgical instruments hitting.
C) Surgical suction noise.
Discussion
In the areas of orthopedic surgery and dentistry, it was reported more than two decades ago that it is possible to determine if an implant is insufficiently fixed through frequency analysis, thus preventing it from loosening [9,10]. However, for hammering and broaching in THA, stability is still determined based on experience and sense without being based on objective data [11]. Frequency analysis is advantageous because it is noninvasive and allows surgeons to make objective determinations [12]. Ooyama et al. used a digital video camera in THA to record the hammering sounds produced when the system was inserted, and after surgery, they conducted a frequency analysis on the recorded sounds. The analysis results indicated that for ten joints out of 22 joints, clusters of hammering sounds were observed that exhibited consistent frequencies three times in a row, and they reported that it is useful to use frequencies as a determination indicator for analyzing the stability of cementless stems [13]. As our analysis results showed [14], it has been reported that the peak frequency when stability was obtained is approximately 3 kHz. This frequency depends not on the stem type but on the impactor’s material [15]. It has been reported that the peak frequency is 8.5 kHz for metal impactors and 4.5 kHz for resin impactors; we used a resin impactor that exhibited a similar frequency [16]. Hammering sound qualities depend not only on the sounds produced when the hammer is in contact with the impactor but also on the ambient medium and environment. Hammering sounds were collected in a quiet environment without any noise being completely eliminated. While the voices of medical staff exhibit a round waveform, such as a sinusoidal waveform, hammering sounds exhibit a sharp signal waveform with a sawtooth wave, meaning that it is possible to distinguish voices, which are noise, from hammering sounds by differentiating their waveforms [6]. Undetected hammering sounds included those that were not detected because their levels were low, which probably required microphones to be selected again. The microphone placed on the upper limb could collect sound without any obstacle because it was directed toward the sound source from the upper part of the sterilization sheet. The surgeons and scrub nurse attended to the microphones placed at the other three locations. The sterilization sheet placed behind the microphone on the head side may have acted as a dish antenna to effectively collect sound waves. We surmised that surgical instruments around the lower limbs produced enough noise in the lower limb side, which was in contact with one another when they were used. It is difficult to distinguish the peak frequencies of sounds produced when surgical instruments are in contact with those of hammering sounds, because their frequency ranges are almost the same. One possible solution is to incorporate an active noise-canceling capability into this application. If this solution does not allow for distinction, the basis of the measurement principle must be significantly changed from the fast Fourier transform to, for example, acoustic emission.
Conclusion
In all cases analyzed; the analysis system successfully determined stem stability in real-time. The analysis system was less likely to fail to detect sounds when the microphone was placed on the head of the patient and directed toward the surgical field. It is possible to distinguish the voices of the medical staff, a major ambient sound in the operating room, from the hammering sounds. However, it is difficult to distinguish the peak frequencies of sounds produced when surgical instruments are in contact with those of hammering sounds because their frequency ranges are almost the same, and solving this problem is the greatest challenge.
Conflict of Interest
The authors did not receive and will not receive any benefits or funding from any commercial party directly or indirectly related to the subject of this article.
Acknowledgment
This study was supported by a Kitasato University School of Allied Health Sciences (Grant-in-Aid for Research Project, No. 2017-2021, 6610), KAKENHI Grant Number JP 26820160. We are grateful to Yasuo Otsu, Masahiro Kakeshita, and Takanori Usui for their assistance.
References
- Mihalko WM, Wimmer MA, Pacione CA, Laurent MP, Murphy RF, et al. (2014) How have alternative bearings and modularity affected revision rates in total hip arthroplasty? Clin Orthop Relat Res 472(12): 3747-3758.
- Moroni A, Faldini C, Piras F, Giannini S (2000) Risk factors for intraoperative femoral fractures during total hip replacement. Ann Chir Gynaecol 89(2): 113-118.
- Schwartz JT, Mayer JG, Engh CA (1989) Femoral fracture during non-cemented total hip arthroplasty. J Bone Joint Surg 71(8): 1135-1142.
- George Whitwell, Claire L Brockett, Steve Young, Martin Stone, Todd D Stewart (2013) Spectral analysis of the sound produced during femoral broaching and implant insertion in uncemented total hip arthroplasty. J Engineering in Medicine 227(2): 175-180.
- Sakai R, Uchiyama K, Takahira N, Kakeshita M, Otsu Y, et al. (2020) Usefulness of hammering sound frequency analysis as an evaluation method for the prevention of trouble during hip replacement. Journal of Biomedical Science and Engineering 13(5): 74-80.
- Sakai R, Kitazato T, Uchiyama K, Yoshida K, Yamamoto T, et al. (2021) Investigation of hammering sound frequency during total hip arthroplasty to prevent intraoperative fracture. Journal of Biomedical Science and Engineering 14(10): 339-345.
- Sakai R, Kikuchi A, Morita T, Takahira N, Uchiyama K, et al. (2011) Hammering sound frequency analysis and prevention of intraoperative periprosthetic fractures during total hip arthroplasty. Hip International 21(6): 718-723.
- Sakai R, Yamamoto T, Uchiyama K, Takahira N, Kakeshita M, et al. (2020) Prediction of intraoperative fracture by hammering sound frequency analysis and stress estimation during total hip arthroplasty. Journal of Biomedical Science and Engineering 13(6): 113-119.
- Li PL, Jones NB, Gregg PJ (1994) Loosening of total hip arthroplasty Diagnosis by vibration analysis. J Bone Joint Surg Br 77(B): 640-644.
- Meredith N (1997) Resonance frequency measurements of implant stability in vivo. A cross-sectional and longitudinal study of resonance frequency measurements on implants in the edentulous and partially dentate maxilla. Clinical Oral Implants Research 8(3): 226-233.
- Kroeber M, Ries MD, Suzuki Y, Renowitzky G, Ashford F, et al. (2002) Impact biomechanics and pelvic deformation during insertion of press-fit acetabular cups. J Arthroplasty 17(3): 349-354.
- Oyama J, Endo MM, Furuichi I (2010) Analysis of hammering sound by sound wave analysis when inserting cementless femoral stem. Orthopaedic surgery and traumatology 53(9): 1105-1109.
- Oyama J, Endo MM, Furuichi I (2011) Analysis of hammering sound by sound wave analysis when inserting cementless femoral stem. Hip Joint 37: 211-215.
- Furuichi I, Oyama J, Endo MM (2012) Analysis of hammering sound by sound wave analysis when inserting cementless femoral stem -6th reports Study of 3 cases of intraoperative fracture. Japanese Journal of Replacement Arthroplasty 42: 149-150.
- Oyama J, Endo, MM Furuichi I (2012) Analysis of hammering sound by sound wave analysis when inserting cementless femoral stem -7th reports ECHELON. Japanese Journal of Replacement Arthroplasty 42: 151-152.
- Furuichi I, Oyama J, Endo MM (2013) Analysis of hammering sound by sound wave analysis when inserting cementless femoral stem-8th reports Analysis of metal impactor use group. Japanese Journal of Replacement Arthroplasty 43: 669-670.
