 Review Article
Review ArticleABSTRACT
Post-surgical infections of the abdominal cavity are a process of infectious origin in which various types of aerobic and anaerobic gram-positive and gram-negative microorganisms are responsible for them; its management has evolved considerably over time, as a result of great advances in imaging studies, the implementation of minimally invasive procedures, as well as innovation in antimicrobial therapy; however, it continues to be a challenge for the medical team because this condition is often a lifethreatening emergency, due to its high morbidity and mortality, which ranges around 30% or more for severe cases, which can be caused by massive contamination of the intraoperative peritoneal cavity or failure of the anastomosis.
Keywords: Infection; Intra-Abdominal; Postsurgical; Management; Etiology; Peritonitis
Introduction
Recently, the interest inintra-abdominal postoperative infections has been increased or due to its high mortality rate that reaches 0.25% in uncomplicated appendicitis; the value is even higher with more than 50% in complicated infections of the biliary tract, and being greater than 60% in some series of tertiary peritonitis [1]; all as a result of the advance in the knowledge of the etiology and physiopathogenesis of the the introduction of new minimally invasive diagnostic techniques and the development of new antibiotic therapy. These infections make up a group of intraand retroperitoneal processes, from local infections to systemic repercussions, considered by some studies as the third most common cause of sepsis or septic shock, and the secondcause of death from the intensive care unit [2]. Postoperative infection of the abdominal cavity is a highly severe condition, accounting for 2.5% of all admissions of critical patients in intensive care rooms. One in 40 severe cases presents an infection in the peritoneal cavity as do 2% of patients operated laparoscopically; on the other hand, 29% of individuals sick with peritonitis in their initial operation, remain with it and need various reoperations to control it, with the consequent long-term hospital stay [3,4]; numerous factors determine its high incidence within them encontramos: the age of the patient, associated comorbidities, the time of diagnostic detection, neoplastic etiology, complexity and duration of the initial surgical intervention; anastomotic suture dehiscence, visceral perforation or necrosis, post-surgical abdominal abscesses and tertiary peritonitis that lead to the development of septic shock and in the worst case the death of the individual [5,6] stand out as serious. The prognosis of infections of the abdominal cavity is largely subject to a careful approach to diagnosis and implement timely aggressive antibiotic treatment in order to avoid culminating in septic shock or its recurrence leading to sequential multi-organ failure and ultimately resulting in the death of the patient. ; which requires multidisciplinary collaboration mainly in complicated cases; including life support measures, control of the focus of infection and abscess drainage and eradication of residual contamination and systematic infection with antibiotic therapy [7].
Methodology
The study design is adapted to a systematic review of the evidence present in the scientific literature on the etiology and management of postoperative infections of the abdominal cavity. The literature search took place between 1990-2021 delving into various bibliographic databases in order to obtain information and review previous studies on the subject exposed. The keywords and Boolean operators used were “infection”, “intra-abdominal”, “postsurgical”, “management”, “etiology”, “peritonitis” described through DeCS (Descriptors in Health Sciences). To achieve a greater update on the subject, the articles published in the last 30 years were set as a temporary filter for the search.
Results
Since ancient times, the surgeon has been faced with a continuous fight against surgical infections that have represented a global health problem, with those of abdominal origin being the most difficult to treat, since the emergence of antimicrobials. Intraabdominal infection has been defined as an infectious process of high prevalence produced by identified microorganisms [8]. Multiple studies have revealed that they are classified into three types: primary peritonitis defined as an inflammation caused in a possible extraperitoneal source, often by hematogenous dissemination; it is usually monomicrobial, whose causative agent involved is Escherichia Coli in 70% of cases. , 10-20% by gram-positive coconuts and 10% anaerobic, its management is aimed at the establishment of antibiotics. Secondary peritonitis is subdivided into first stay as acute by perforation (highlighting as a cause peptic ulcer, inflammation and necrosis of the intestine and appendicitis);second in postoperative peritonitis that isevident between the fifth or sixth day and habitual mente are polymicrobial and synergistic infections whereas the isolation of Enterococcus and fungi, especially of the genus Candida, has increased markedly in this type of infection; other sources have highlighted, such as the relationship of E. Coli and bacteroides fragilis is postulated with a 37% mortality and 100% development of abscesses, while the isolated E. Coli is located with a lower mortality percentage of 30% without abscess ormation; And finally post-traumatic peritonitis [9,10]. Tertiary peritonitis is a persistent peritoneal infection after the apparently correct treatment of the two mentioned above, of late and severe state of intra-abdominal infection caused by a deterioration in the defense mechanism of the host incapacitating it to contain said condition [11].
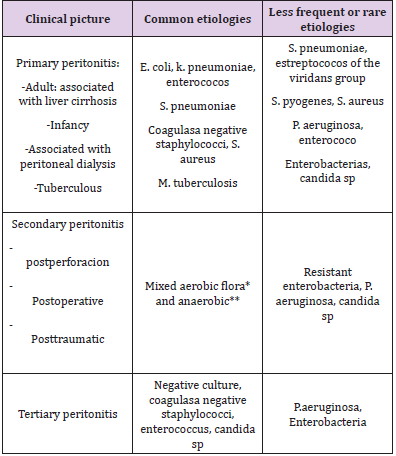
Table 1: Classification and etiology of peritonitis. Adapted from: N. Zappella C. Depondt N. Carrara P. Montravers. Secondary peritonitis of the adult. EMC - Anesthesia-Resuscitation. Volume 48, Issue 1, February 2022, Pages 1-18.
Note: * E. coli, streptococci of the viridans group, other enterobacteria
** B. fragillis, anaerobic stretococci, clostridia.
Postoperative infections of the abdominal cavity are part of the extensive group of secondary peritonitis that occur as a result of inflammatory or neoplastic intestinal pathologies that lead to the perforation of a hollow viscera, by occlusive vascular processes with mesenteric ischemia and intestinal necrosis due to lesions of the abdominal cavity or be secondary to surgery. In all these situations, contamination of the peritoneum with intestinal contents can occur and leads to the development of localized abscesses or peritonitis. Intra-abdominal infections secondary to a surgical procedure develop mainly by the development of massive microbial contamination during surgery or by a failure of an anastomosis that ends in a dehiscence of the suture with the subsequent contamination of the abdominal cavity [12]. Regarding its etiopathogenesis, it is relevant to take into account the magnitude and quality of the inoculum in intra-abdominal infections (Table 1). The presence of blood, necrotic tissues, foreign bodies, bile salts or other substances encourage the development of germs and thus the continuation of infection, also emphasizes the general and local defenses of the host, the latter where the lysozyme secreted by the mesothelial cells of the peritoneal tissue, the adhesions to it caused by the synthesis of fibrin from the serous peritoneal, the greater omentum and the polymorphonuclear with their high phagocyte capacityria, will tend to delimit and locate the infection.
Recently, bacterial peritonitis is linked to a large response of intra-abdominal compartmental cytokines, a moderate and beneficial amount but a high rate is indicative of a poor prognosis. Mesothelial cells promote the production of tumor necrosis factor (TNF-alpha), IL-1, IL-6, and IL-8 [13]. The numerous advances in the management of this pathology haveimproved significantly achieving a marked reduction in the intra-abdominal bacterial count, despite this certain patients achieve the consequent death of an uncontrolled activation of the inflammatory cascade. For this reason, intraperitoneal IL-6 values have been considered suitable prognostic markers for this type of condition [14].
Discussion
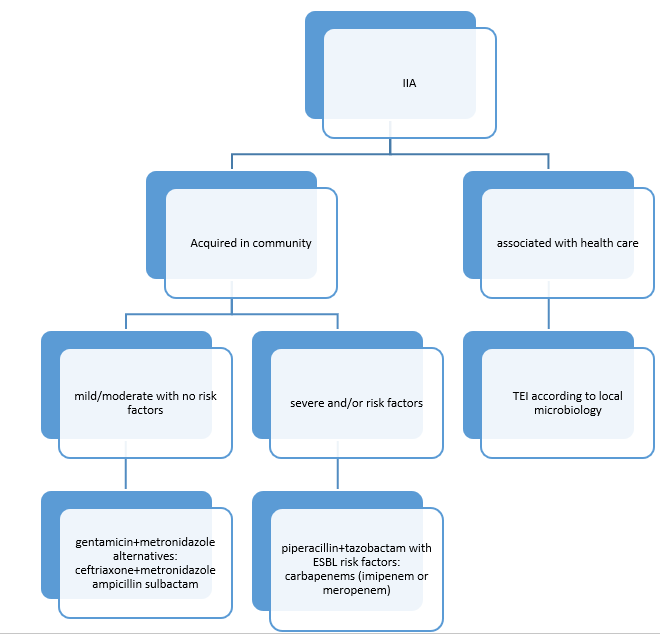
Figure 1: Algorithm for the treatment of intra-abdominal infections (IIA). Treatment. Taken from: LIliana Clara, Viviana M. Rodríguez, Pablo Saúl, Cecilia Domínguez, Mercedes Esteban. Intra-abdominal infections. MEDICINE (Buenos Aires) 2018; 78: 417-426.
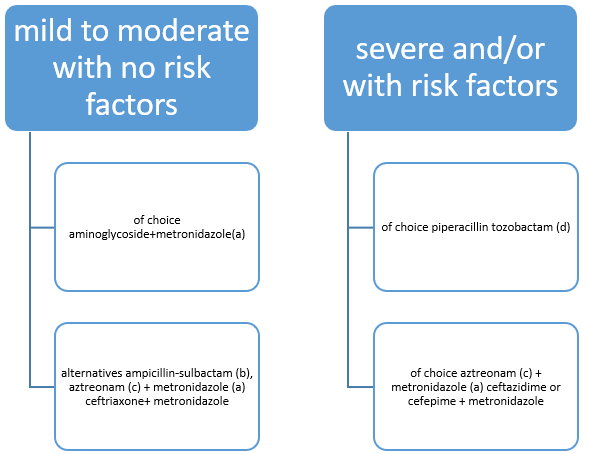
Figure 2: Empirical treatment of intra-abdominal infections in the community. Taken from: LIliana Clara, Viviana M. Rodríguez, Pablo Saúl, Cecilia Domínguez, Mercedes Esteban. Intra-abdominal infections. MEDICINE (Buenos Aires) 2018; 78:417-426.
The diagnosis of an infection in the abdominal cavity requires certainty and promptness, since the therapeutic delay leads to greater mortality and percentage of surgical reoperations of the patient, so it is recommended that the medical staff appropriate the elements in order to avoid a fatal outcome by performing a computerized tomographic study considered the best imaging study in these cases and in the acute abdomen in general, or failing that an ultrasound; however, it is also resorted to using auxiliary means such as blood count that revealed anemia, less than 8 g / L and leukocytosis with deviation to the left; increase in serum creatinine and hyperbilirubinemia and glicemia, also the blood gas will show persistent metabolic acidosis. Clinically, post-surgical intraabdominal infection usually manifests itself with elevated febrile peaks above 38ºC, chills, abdominal distention and hypersensitivity, generalized peri-tonitis in certain cases, the presence of a tabla abdomen, or the occupation of the Douglas sac fundus, others such as a fall in diuresis and blood pressure, tachycardia among others [15]. Once a definitive diagnosis is established, antibiotic treatment is immediately started that although the main therapy is surgical intervention in order to remove the origin of the image, pharmacological therapy plays an important role in the elimination of pathogens Your choice will depend on various factors such as the suspicion of responsible microorganisms, underlying pathology, speed and effectiveness in the control of infection, and their pharmacological characteristics [16,17].
The fact that the microbial agents involved in the infection are myxtos (aerobes and anaerobes) forces the doctor to use broadspectrum antibiotic therapy with an average duration in patients with a good course of the disease of about 7 days, however there is evidence documenting that an appropriate immune response and focus control, the residual inoculum can respond to treatment in a shorter time, so its completion responds to various parameters such as the normalization of the leukocyte level, (Figure 1) apirexia and recovery of intestinal functionalism [18]. The precocity of antimicrobial management guarantees greater effectiveness in the control of infection since cohort studies carried out in patients with severe sepsis have shown that for every hour that the start of appropriate therapy is delayed, the level of mortality increases by 7.6% [19]. The scheme of empirical antibiotic treatment takes into account the origin of intra-abdominal, community and nosocomial infection, the severity depending on the variables of SIRS, APACHE and venous lactate as well as the risk factors for poor evolution[20]. The surgical approach to intra-abdominal infection is based on 3 basic pillars whose main objective is to avoid the continuation of the infection that leads the patient to develop multi-organ failure, within these are: eradicate the focus, reduce the contamination of the abdominal cavity and treatment of the residual infection in an attempt to follow during the postoperative period the mentioned peritoneal cleaning [21] (Figure 2).
It should be borne in mind that at the time of reoperation there is an abdominal cavity in poorly optimal conditions, making it difficult to properly explore it. The resolution will depend on whether the infection is local or generalized, being simpler if it is by the first mentioned with one or more abscesses that resolves with the placement of a drain, unlike those cases in which the source of contamination requires surgical intervention, being complicated to perform a resection and reconstruction with primary anastomosis. The usual is to execute a resection, adequate and effective debridement, proximal referral and plan new interventions [22]. Postoperative infection of the abdominal cavity is an entity that is responsible for having a multidisciplinary team due to its high complexity with respect to a diagnostic and therapeutic approach, as well as the multiple clinical paths that can be taken during its severity; the earlier the detection of it, the sooner the decision of a possible intervention increases the positivity of a prognosis [23].
Conclusion
Intra-abdominal infections continue to be the subject of debate due to their complexity in diagnosis and management, which over time has become easier with the numerous advances in imaging techniques for early detection, minimally invasive procedures as well as the disposition with which the doctor has a wide range of antibiotics capable of counteracting it. that in conjunction with an adequate surgical intervention is effective to completely eradicate the source of contamination [24]. Due to the high mortality that it has documented, it is necessary to establish the appropriate guidelines for its resolution.
References
- (2012) Intra-abdominal Infections Protocol HG Mancha Center. Mancha Centro. Mancha Centro. Services Surgery, Pharmacy, M. Internal and Services Surgery, Pharmacy, M. Internal and Surgery, Pharmacy, M. Internal and Microbiology Update 2012.
- Daniel Stamboulian, Eduardo A, Argü Ernesto D fron. Intra-abdominal infections. Department of Infectology and Preventive Medicine, Güemes Sanatorium, Private Hospital. Infectology Service, British Hospital of Buenos Aires.
- Mesa Izquierdo O, Ferrer Robaina H, Mora Batista R, Matos Ramos YA, Travieso Peña G (2019) Morbidity and mortality due to secondary peritonitis in the surgery service. Cuban Journal of Surgery 21(2): 124-132.
- González López A, Garí Marcos L, López Roca JA, Sarabia Albor AM, Fernández Rivas DA (2020) Incidence of intra and postoperative complications in geriatric patients during elective major abdominal surgery. Cuban Journal of Anesthesiology and Resuscitation.
- García Basulto MJ, García Rodríguez ME, Benavidez Márquez A, Koelig Padrón R (2020) Patients with intra-abdominal infection in the intensive care unit. Cuban Journal of Surgery.
- Pérez Guerra JA, Vázquez Hernández M, Ramírez Moreno R López García FR (2017) Abdominal reinterventions: prevalence in elective surgeries and emergencies. Surgery and Surgeons.
- Munson JL (1991) Treatment of intra-abdominal sepsis. Clin Chir Notrh Am 6: 1229-1239.
- Condon RE, wittman DH (1998) Intraabdominal infections. In: Gorbach SL, barlett JG, blacklow NR (Eds.)., infectious Diseases, (2nd )., WB Saunders Company, Philadelphia, pp. 793-800.
- Jorge Cabarca Montemiranda (2008) Intra-Abdominal Infections. Repertoire of Medicine and Surgery 17(2).
- N ZappellaC, Depondt N, Carrara P, Montravers (2022) Secondary peritonitis of the adult. EMC - Anesthesia-Resuscitation 48(1): 1-18.
- Rangel Frausto, Pittet D, Costigan m (1995) The natural history of systemic inflammatory response syndrome (SIRS). JAMA 273: 117-123.
- Pollock AV (1990) Nonoperative anti-infective treatment of intraabdominal infections. World J Surg 14(2): 227-230.
- Schein M, Wiitmann DH, Holzheimer R, Condon RE (1996) Hypotesis Compartmentalization of cytokines in intraabdominal infection. Surgery 119(6): 694-700.
- Caínzos M, Alcalde JA, Bustamante M, Potel J, Puente JL (1995) Anergy and postoperative septic complications. In: Engemann R, Holzheimer R, Thiede A (Eds.)., Immunology and its impact on infections in surgery. Berlín Springer, Germany, pp. 177-186.
- Guerra Macías I, Espinosa Torres F (2020) The professional performance of the general surgeon in the early detection of acute postoperative peritonitis. Rev Cub de Tec de la Salud.
- LIliana Clara, Viviana M, Rodríguez, Pablo Saúl, Cecilia Domínguez (2018) Mercedes Esteban. Intra-abdominal infections. MEDICINE (Buenos Aires) 78: 417-426
- Nichols Re Surgical Inections (1996) Prevention and Treatment – 1965 To 1995. Am J Surg 172: 68-74.
- Cattan P, Yin D, Sarfati E, Lyu R, de Zelicourt M, et al. (2002) Cost of care for inpatients with community-acquired intra abdominal infections. Eur J Clin Microbiol Infect Dis 21(11): 787-797.
- Kumar A, Roberts D, Wood K, Light B, Parrillo J, et al. (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival inhuman septic shock. Crit Care Med 34(6): 1589-1596.
- Xavier Guirao, Javier Arias, Josep M Badı, Jose A Garcıa Rodriguez, et al. (2010) Recommendations in the empirical antibiotic treatment of intra-abdominal infection Elsevier Spain CIR ESp 87(2): 63-81.
- Mattox KL(1997) Introduction, background, and future projections of damage control surgery. Surg Clin North Am 77(4): 753-759.
- M Caínzos Fernández (2001) Postoperative peritonitis. Cirugía Española 69(3).
- Iliana Guerra Macías, Juliet Suárez Guerra, Jaila Suárez Guerra (2021) Some necessary considerations about postoperative intra-abdominal infection. Cuban Journal of Military Medicine 50(4): 02101281.
- LIliana Clara, Viviana M Rodríguez, Pablo Saúl, Cecilia Domínguez, Mercedes Esteban (2018) Intra-abdominal infections. MEDICINE (Buenos Aires) 78: 417-426.
