 Mini Review
Mini ReviewIntroduction
In general terms, we could define the specialty of Obstetrics and Gynecology (hereinafter G&O), as the field of medicine that specializes in the care of women during pregnancy and childbirth, and in the diagnosis and treatment of diseases of the organs. female reproductive. With this, it is intended that the women of the world reach the highest possible standards of health and physical, mental, reproductive, and sexual well-being throughout their lives [1]. As old as humanity, the care of women in a way specifically linked to the regarding pregnancy and childbirth, they have been constant in the different societies in which life has developed. Much more modernly, barely a century or a little more, the general care of women has been spreading to the extent that survival first, longevity later, made their way into our vital evolution. To all this, if anything, and even more closely in time, one could add in a similar sense, the alterations of the male reproductive system in relation (exclusively) to the search for fertility.
In this constant and changing evolution, like life itself, our specialty of G&O is today dynamically witnessing a continuous and perpetual “paradigm change” [2]. All this surely hand in hand with the multiple social changes (and even demographic), that women themselves have been leading, over the past 100 years (suffering many times, which of course must also be recognized), until completing a path that has caused a better and greater attention to health care over even other more “classic” functions. To speak, therefore, of the evolution of G&O is inevitably to refer to the evolution of the woman herself [3] and her role in the world, since ours is a specialty that, far from attending only to the disease, deals extensively and more intense each time, of health care and the evolution of a situation that is so physiological and essential for the future of humanity, such as gestation, its search when it does not arrive, and everything related to both situations and their complications and evolutions. The objective of this short clinical note is to succinctly review those circumstances of all kinds (medical and biological, but also social and cultural) that condition the paradigm changes that gynecology faces in this wellentered 21st century. Similarly, perhaps provide some guidelines for reflection on these changes in future direction.
Reflections for Paradigm Changes
Indeed, women have gradually changed their position in a radical way, occasionally in a more abrupt or intense way, but qualitatively and quantitatively definitively in the world (at least in the Western world), presenting very different needs, with an “empowerment” generalized and at all levels [4] With it, our specialty has been forced to assume cultural changes, with different beliefs and origins of the women themselves that forced, at different times in history, to modify protocols and diverse approaches for different pathologies. Barely half a century ago, various alternative forms of fertility [5] were described by gynecologists (among others), even designing new forms of maternity, thus offering an alternative fertility to the natural one of the past 400,000 years (with in vitro fertilization, fertility deferred or without a partner [6], the possibility of procreating even beyond menopause in “older” women [7], the cryopreservation of ovarian tissue before its definitive damage resulting from a necessary iatrogenesis, maternal surrogacy that even unfolds the (once) immutable role of the old “mother there is only one”..., etc, etc).
With the social changes came the modifications even of civil ethics, always under revision, permanently changing like life itself [8,9]. Trying to manage the past from the point of view provided by current thinking or the prevailing civil ethics today is not only a serious error, but also leads to permanent frustration due to the (wrong) value judgment that it would entail for people, attitudes and stories that because they are dead at least, they do not have the slightest opportunity not only to defend themselves but perhaps even to explain their positions of yesteryear [10]. In this context of permanent change, our specialty today has taken as its commitment to the identification and report to the police of violence against women in any of its states and links. Thus, the gynecologist assumes a role that goes beyond health care itself for diseases and conditions of the female genital tract and transcends care and empathy with women (not sick), insofar as they are different and susceptible to receiving verbal damage. psychological or physical.
Finally, at least for now, while our specialty is the true queen and pioneer of minimally invasive and endoscopic surgery at all levels (abdominal, perineal, even breast...) [11], while witnessing the unstoppable development of surgery to distance and robotized [12], turns over time from a primitive and fundamentally surgical perspective, to increasingly less invasive, less surgical extremes, more on the side of internal medicine with the approach of healthy aging as a banner in a continuously older population that assumes regenerative medicine and repair of senility [13] in a classic medical-surgical specialty, less and less surgical and more and more medical. In this order of things, the gynecologist becomes a true “internist for women”, with new diseases for him such as climacteric care and aging with hormonal decline, osteoporosis or sarcopenia that cause so much disability in a world that honors even the puerile adoration of the increasingly immature youth, while socially despising the “sexalescence” [14] and the creativity of the (previously misnamed) “third age” and the “silver economy” [15], true engines of entrepreneurship beyond retirement. Thus, in this dynamic context, the gynecologist assumes to be more than “the woman’s family doctor”, to the point of mutating and being the “caregiver or healthprovider of women’s health throughout life”, the authentic alma mater of this blessed specialty that since assistance at the beginning of life, is obstinate in staying by her side while she lives her dreams of professional fulfillment in a changing environment and in permanent crisis.
Let’s toast to those paradigm shifts that history forces us to make every day and let’s hope that this very future grants us sufficient capacity to adapt to all of them and pilot them in an environment that will always be imbued with risk and uncertainty, such as biology. same of the woman; perhaps combating ignorance and empathy are the (only) keys to achieving it [16].
Final Comments
It is extraordinary to conclude anything concrete when constant change is the work dynamic not only of our specialty, but of biology and of life itself. In relation to the issue that concerns us today, there are surely more factors (than those briefly indicated in (Table 1)) and some even more important than those mentioned (such as the ambulatory use of various surgical procedures, the substantial change in the role of assistance to childbirth, the modeling of new assistance groups, even birth outpatient care [17], etc, etc), but between all of them they are transforming a specialty that was born timidly and quietly at the risk of intuitive assistance at birth as a need of social populations in anywhere in the world and that today assumes a change of roles driven by paradigm shifts that, like life itself, never cease throughout not only the previous century but those to come.
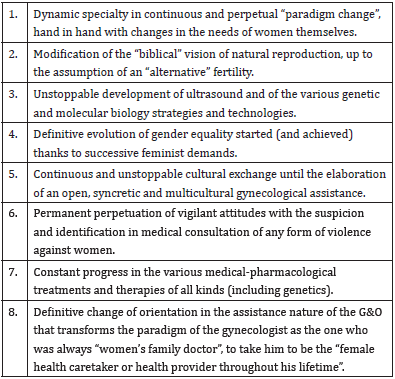
Table 1: Main paradigm changes assumed by gynecology in the 21st century. If it were a matter of systematizing the milestones of the supposed paradigm shift that G&O has been leading in this first quarter of the new century, apart from other more general conditions for all health care, we could point out a few items that we try to systematize below one by one.
Therefore, welcome are all those changes that allow us to enjoy life itself, in which everything and always is mutation, because otherwise it would not even be Life.
Conflict of Interest
The authors declare that they have no conflict of interest in this manuscript.
Contribution of Each Author
JLN collaborated with the original idea, the bibliographic search, the initial and final writing of the manuscript. JM collaborated with the revision of the manuscript and its final writing. SPG collaborated with the revision of the manuscript and its final writing.
References
- (2022) FIGO Strategic Plan 2021-2030. International Federation of Gynecology and Obstetrics.
- Neyro JL, Cristóbal I, Vásquez D, Franco R, Palacios S (2020) Reflections on healthcare after the COVID19 pandemic. Toko Gin Pract 79(6): 338-343.
- (2022) Women of the world, unite! Explore women's activism from past generations to the present.
- (2022) Goal 5: Achieve gender equality and empower all women and girls.
- Berquo E (1989) The family in the twenty-first century: a demographic review]. Rev Bras Estud Popul 6(2): 1-16.
- Pedro J, Brandão T, Schmidt L, Costa ME, Martins MV (2018) What do people know about fertility? A systematic review on fertility awareness and its associated factors. Ups J Med Sci 123(2): 71-81.
- (2014) American College of Obstetricians and Gynecologists Committee on Gynecologic Practice and Practice Committee. Female age-related fertility decline. Committee Opinion No. 589. Fertil Steril 101(3): 633-634.
- Persson I, Savulescu J (2010) Moral transhumanism. J Med Philosophy 35(6): 656-69.
- Neyro Bilbao JL, Ángel Elorriaga M, Lira Plascencia J (2015) Contraception and bioethics: between the conscience objection and the autonomy principle. Ginecol Obstet Mex 83(2): 125-38.
- Sellers J (1989) Medical ethics and the civil rights movement. Why informed consent is too little, too late. Second Opin. 1(12): 46-61.
- Bhagavath B, Benjamin A (2015) Minimally Invasive Gynecologic Surgery for Benign Conditions: Progress and Challenges. Obstet Gynecol Surv 70(10): 656-666.
- Minig L, Achilarre MT, Garbi A, Zanagnolo V (2017) Minimally Invasive Surgery to Treat Gynecological Cancer: Conventional Laparoscopy and/or Robot-Assisted Surgery. Int J Gynecol Cancer 27(3): 562-574.
- Burns TC, Quinones Hinojosa A (2021) Regenerative medicine for neurological diseases-will regenerative neurosurgery deliver? BMJ 373: n955.
- (2022) The second adolescence.
- (2022) Silver economy, older people will be the engine of the economy of the future.
- Saltelli A, Funtowicz S (2004) The Precautionary Principle: implications for risk management strategies. Int J Occup Med Environ Health 17(1): 47-57.
- (2022) Available in https://www.neyro.com/2015/05/04/la-revista-hola-entrevista-aldoctor-neyro-en-relacion-al-parto-ambulatorio-de-la-duquesa-de-cambridge/. Last access May 22.
