 Case Report
Case ReportABSTRACT
Millimetric wave (MMW) therapy was discovered in the 1970s’ in USSR countries and used clinically for their hypoalgesic properties in various pain pathologies. Subsequently, these hypoalgesic properties were related to a central nervous system response following peripheral stimulation, mainly involving secretion of endorphins, as well as other neurotransmitters such as parasympathetic, DOPA, etc... In the more recent past (after 2010), the development of miniaturized solutions has allowed the personal use of MMWs -outside medical structures- in the management of chronic pain, and in particular neuroplastic or nociplastic pain, independently of any etiology. We report here on two cases of fibromyalgia, in which these two contributions to pain are involved. In each case, the patients experienced the use of a portable, wristband designed MMW system. The deliberate use of the device was first intended for wellness or stress relief purposes. The notion of the non-specificity of MMWs on chronic pain is discussed at the end of the article.
Keywords: Pain; Nociplastic; Neuroplastic; Hypoalgesia; Millimetric Waves; Fibromyalgia; Endorphins
Introduction
Until the 2010s, millimetric wave applications (MMW, electromagnetic radiation of frequencies from 30 to 100 GHz) were mainly intended for technical innovations: military - with radar; or civil - for driving assistance or in communications systems where the renewed interest for millimetric waves was linked to the development of 5G (27GHz) and 6G (up to THz). In contrast, the medical applications identified and used clinically, in particular for pain conditions, in the USSR in the 1980s [1,2], had sank into oblivion. Since then, research led to the development of a plausible mechanistic support for these effects (essentially hypoalgesic and anti-inflammatory effects). Meanwhile, the miniaturization of electronic systems has made it possible to envisage a manageable portable device, designed as a wrist-worn transmitter. As this system is harmless, the immediate question is to identify possible clinical indications. Along with well-being or stress control, pain relief is obviously a primary objective, and especially chronic pain. Specifically, as reported by Tanaka et Al in “The International Classification of Diseases”, eleventh revision (ICD-11[3]), chronic pain can be classified into primary and secondary. The primary chronic pain is fibromyalgia or low-back pain; the secondary chronic pain occurs secondary to an underlying medical condition subcategorizing into cancer-related, post-trauma, neuropathic, headache and orofacial, visceral, and musculoskeletal pain”.
Moreover, IASP [4] clearly distinguishes 3 main modes of pain: nociceptic, neuropathic, and nociplastic. In health care, etiological treatment of any lesion is the obvious effective approach, especially for nociceptive and/or neuropathic pain, where the support of the injury, whether anatomical, tissue or nerve, is generally known. As regards the third type of pain - nociplastic - and especially fibromyalgia, where the multifocal painful context (the usual hyperesthesia, among others) is in the foreground, the response to “classic” analgesics is disappointing, leading to a chronic evolution and to psychological and social consequences. Can MMW systems then be helpful in the management of these significant nociplastic pains, both physically (e.g. for wellness or rehabilitation purposes) and psychologically? Finally, the synthesis of these classifications covers many complex and poorly understood pathologies, including isolated nociplastic pain (fibromyalgia among others) or mixed pathologies associated with ongoing nociceptive or neuropathic pain (premenstrual pain, arthropathy, cancer, post trauma, etc.). We specifically report here on two clinical cases of combined fibromyalgia and other chronic pain.
In addition to their long-term treatment, both patients presented here decided to try out the MMW transmitter bracelets available on the internet and initially intended to improve wellbeing and sleep, and to relieve stress. The basic principle of this system uses the analgesic properties of millimetre waves (in the 30-90 GHz bands), widely described in the last decade of the 20th century and more recently reviewed in some recent studies and reports. The basic mechanism relies on endorphin secretions from the CNS, which in turn is triggered by a peripheral stimulus (i.e., MMW) applied to the cutaneous receptors of the wrist. In practice, as described elsewhere [5], the miniaturized transmitter is mounted on a bracelet and worn like a watch: this device emits a continuous electromagnetic wave of 60 GHz at a power density of 14mW/cm2 on 2cm2 in contact with skin surface (3 sessions of 30 minutes per day) on the palmar side of the wrist, i.e. in very close contact with the median nerve. We report here on the patients’ pain management and the evolution of their autonomy.
Case Descriptions
The first patient, Mrs H…, 37 years old (born in 1982), was employed as a secretary in a military settlement with no history of surgery, ongoing medical treatment or addiction. In April 2020, while picking up a heavy object on the ground, she experienced acute and extremely violent low back pain (VAS estimated at 9, see Table 1). Initial treatment was carried out by infusion (DIAZEPAM, TRAMADOL, PREDNISONE, PARACETAMOL) then per os after several days, maintaining a VAS of 7. The painful areas were not clearly identified but fluctuated, along with migratory paraesthesia. Clinically, there was a moderate motor deficit in both lower limbs, without Lassegue sign, but with sharp reflexes and a bell sign in the L3L4 vertebrae. In these physical conditions, neither daily activities nor work were possible. This state was to last until December 2020. In the meantime, the symptomatology diversified and completed in the form of Arnold neuralgia located on the right side, with irradiations in the right hemi -skull, and on the radial radius of the right upper limb (path C6).The electromyographic tests carried out did not show any abnormalities, nor did the biological results (ACAN, rheumatoid factor, serum protein electrophoresis, TSH ...). The MRI scans performed excluded any root or foraminal constraint at the lumbar level and showed only a posterior overhang located on the right at the C5C6 level. The combination of gabapentin (75mg/ day); gentle physiotherapy and TENS® stimulation provided only partial pain relief (constant VAS) still at 5 or above. At the medical consultation at the end of her legal leave, fibromyalgia diagnosis was finally made. As shown on the SF36 score [6] at that time (Table 2), Mrs Therese H. was clinically and psychologically unable to work, while the medical support was unsatisfactory. Thus, she finally decided to test the millimetric device (MMW) at J0.
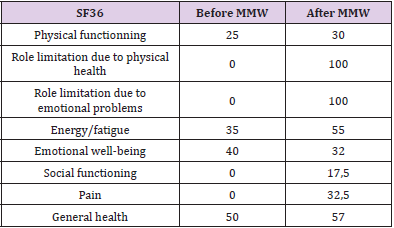
Table 1: Calculated SF36 [6,21] score before and after 1-month MMW trial.
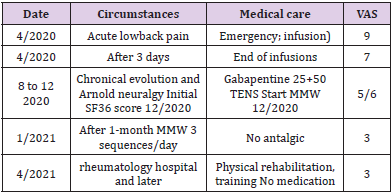
Table 2: Evolution of pain with corresponding care and clinical milestones.
After a couple of days (3 sequences a day) Mrs H. stopped all medication completely and noted a progressive improvement of her physical autonomy as well as a relief of pain. This improvement appears clearly on the SF36, with pain scores recorded after 1 month of MMW use. These dramatic changes were particularly marked for disabilities related to functional and physical problems (0 to 100). This meant that she could do some shopping again and take care of her children (and possibly carry them). Pain relief was also noted (score dropped from 0 to 32.5) although still incomplete (VAS fell from 5 to 3). Moreover, these changes enabled her to undergo rehabilitation in a rheumatological hospital. She was finally able to resume her professional activities (with a converted workstation) and to take care of her children (including play activities such as walks) Second patient: Ms M…, aged 49 (born in 1972) worked as paramedical health manager in a military settlement. In 2004, she contracted postpartum Hashimoto’s thyroiditis which resulted in an unstable and unbalanced hypothyroidism. Alternating hypo-/ hyper-thyroïdism on Levothyroxine was, at the time (2004), given as an explanation for her chronic fatigue. More recently Morton’s disease was identified (nodule on the left foot), as well as a moderate psoriasis (ears and scalp). Her main ailment was actually a multifocal disseminated burning pain, involving:- in the limbs: fingers, right hand and shoulders; feet (from the sole to the inner ankles). Initial VAS ranged from 4 to 6;- in the axial skeleton: neck, back and lumbar pain. Initial VAS ranged 4 to 7.
The sacroiliac MRI was found to be normal, as were X-rays of the hands and feet (showing only limited inflammation) and biological markers (ACAN, FR, antibodies, etc.). These factors allowed to rule out inflammatory rheumatic pathologies (PR, PSR, LE) and Lyme disease (endemic area). The diagnosis of fibromyalgia was finally established and scored as follows (see Table 3): Remarkably, due to the energetic and voluntary nature of the patient, the consequences related to fibromyalgia were minimal, exclusively regarding: role limitation (item 2, Table 3) due to physical and emotional health problems and limitation of social functioning (item 3, Table 3). Not surprisingly these sections of SF36 were little improved neither by the use of MMWs, nor by the exercise rehabilitation program. Conversely, although Ms M. still felt tired, feelings of general heath and energy were improved, while pain decreased significantly (22.5 to 45, see also Table 4). These results were somewhat confounded by the simultaneous drop in pain, which in turn was reduced by physical activity improvement (itself possible due to the decrease in pain!). This feature is illustrated in Table 4.
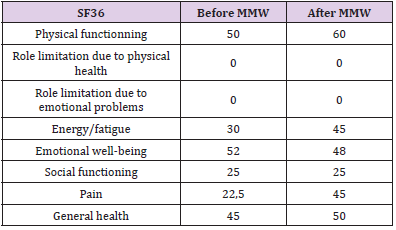
Table 3: Calculated SF36 outcomes [21] score before and after 4-month MMW trial.
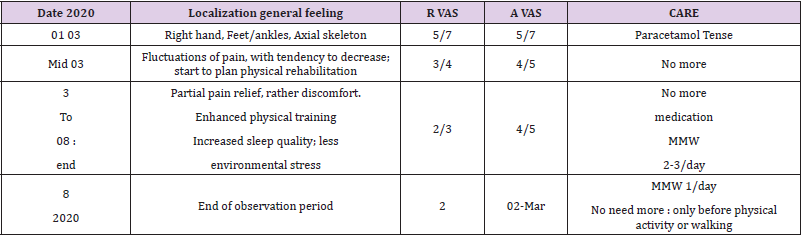
Table 4: VAS evolution and care over time / MMW use and training (R: rest; A: activity).
Discussion
Millimetre Wave Therapy (MMW), as used in Eastern Bloc countries from the 1970 onwards, consisted in the application of electromagnetic waves in the alternative treatment of a wide variety of diseases. It involved millimetre wavelength at extremely high frequencies of the order of 40-60GHz. Due to the low power involved (10mW / cm2) applied very locally (loco dolenti or at different acupuncture points), the method did not cause any adverse effects. Later, after a period of complete disuse, several research teams continued to study MMW therapy for various applications, including chronic pain management for which there were no associated side effect. At this time, more than a simple thermal effect, this mechanism of direct stimulation of nerve endings was found to trigger a central response mediated by the production of endorphins. Studies reporting a loss of effect with naloxone have strongly supported the hypothesis of an “opioid-induced” pathway based on central secretion of endorphins (CNS) triggered in the periphery (skin). In addition to fundamental molecular and cellular work, a large number of animal studies Radzievsky [7], Chuyan and Dzheldubayeva [8], Ziskin [9], and human investigations, have highlighted the potential value of MMWs in the field of pain relief or treatment.
Thus, with regard to experimental pain in animals, the authors concluded that “the analgesic effects are characterized by a certain universality”. With regard to human outcomes, the reviews by Pakhomov [10], Alekseev [11] and Mattsson [12] provide a comprehensive approach to the clinical results observed in MMW. These include experimental results (elevation of the pain threshold, cold tolerance) in healthy volunteers (Radzievsky, et al. [13,14]), as well as observations of analgesic effects on clinical neuropathic pain: diabetic sensorimotor polyneuropathy (Moazezi, et al. [15]), trigeminal neuralgia (Mediaktov, et al. [16]) or chronic joint pain (Bakaliuk, et al.[17]). Usichenko [18] also focused on pain from a wide variety of conditions in terms of their nature (somatic, visceral, neuropathic) and mode of expression (acute, chronic), on which the analgesic effects of MMW had been observed. In the field of neuropathic/neurosomatic pain, the National Center for Complementary and Alternative Medicine (NCCAM, USA [19]) had also identified “this form of treatment (MMW) as one of the main fields of complementary and alternative medicine in terms of ‘analgesia’, following the identification of so-called nociplastic pain, including fibromyalgia”. In the case of fibromyalgia, disturbances in neuroplastic processes involved in the balance of inhibitory systems have been proposed as mechanistic support, leading to a “sensitization syndrome” mechanism. This is manifested by hypersensitivity to sensory stimuli and an abnormal - exaggerated – response to stress. As Wallace, et al. [20]. state, this is “the decline of descending inhibitory activity (deregulation of dopamine, serotonin, norepinephrine, epinephrine and endogenous opioids) and enhancement of endogenous activity. ascending exciter (author’s translation)”. Note here that these are non-endorphinic action points already mentioned in MMWs [21].
In the face of limited effectiveness of drug-based solutions, which are not without side effects, non-invasive and nonmedicinal (drug-free) solutions are meeting a growing demand from patients, especially if they are effective and ambulatory. Discontinuation of medical treatment (analgesics) was achieved in both cases, especially for P1. Although the first non-drug treatment recommended to patients suffering from chronic pain is physical exercise, it is extremely difficult to apply it, as even the simplest gestures of daily life are painful. In the two cases presented here, the use of MMWs made it possible, by acting on the pain and the physical and social effects of fibromyalgia, to take a step towards rehabilitation, in a rheumatological centre (patient 1) or to enable a physical exercise programme (patient 2), and even more to improve social and family experiences.
The considerable miniaturization of the system makes it ambulatory, even portable (e.g. by integration into a bracelet, marketed as a non-medical anti-stress wellness device) and selfmanageable by the patient, offering a considerable advantage.
Concluding Remarks
In the absence of stable anatomical, clinical or paraclinical cause (typically fibromyalgia), the decrease in pain intensity, with or without a placebo effect, combined with an active contribution to the management of the device, allows the other rehabilitation procedures to be carried out, where sports activity/physical rehabilitation is the main focus. In conclusion, even though the MMWs transmitter device is originally a bracelet designed and marketed for well-being and stress relief, its action has historically proven to be effective in a non-specific way on all kinds of pain, such as those related to fibromyalgia. At this stage, it would be desirable to validate this effective, harmless, inexpensive and ambulatory method through in-depth clinical trials.
Acknowledgment
Many thanks to Carolyne Ramusga-Bassani, (Formation and Talents Company) for manuscript correction and fruitful discussions.
Public Declaration of Interest
JC Debouzy works as independent medical advisor in electromagnetism, Remedee Labs is one of the costumers ; D Crouzier is the Remedee Labs CEO.
References
- Yanenko О, Peregudov S, Fedotova I, Golovchanska О (2014) Equipment and Technologies Of Low Intensity Millimeter Therapy. Radioelektronika biomeditchiinii Tekhlogyi 59: 103-110.
- Pakhomov AG, Akyel Y, Pakhomova ON, Stuck BE, Murphy MR(1998) Current state and implications of research on biological effects of millimeter waves: A review of the literature. Bioelectromagnetics 19: 393-413.
- Armstrong HL, International classification of diseases, eleventh revision (ICD-11), 2021, eprints.soton.ac.uk.
- IASP Definitions of Chronic Pain Syndromes.
- Debouzy JC, Verdu P, Crouzier D (2021) Paripex. Indian Journal of Research10(5): 2250-1991.
- Ware JE, Sherbourne CD (1992) The MOS 36-Item Short form health survey (SF-36), I. Conceptual framework and Item selection. Medical Care 30: 473-483.
- Radzievsky A, Gordiienko O, Cowan A, Alekseev SI, Ziskin MC(2004) Millimeter-Wave-Induced Hypoalgesia in Mice: Dependence on Type of Experimental Pain. IEEE Trans Plasma Sci 32: 1634-1643.
- Chuyan EN, Dzheldubayeva ER (2007) Roles of Different Neurochemical Systems in Mechanisms Underlying the Antinociceptive Effect of Extrahigh-Frequency Electromagnetic Radiation. Neurophysiology 39(2): 165-173.
- Ziskin MC (2006) Physiological Mechanisms Underlying Millimeter Wave Therapy. In: Ayrapetyan SN, Markov M.S. (Eds.)., Bioelectromagnetics Current Concepts. NATO Security Through Science Series.
- Pakhomov AG, Murphy PR(2000) Low-intensity millimeter waves as a novel therapeutic modality. IEEE Trans Plasma Sci 28: 34-40.
- Alekseev S, Ziskin MC (2018) Biological and Medical Aspects of Electromagnetic Fields, in Biological Effects of Millimeter and Submillimeter Waves (4th)., pp. 200-210.
- Mattsson Mo, Simko M (2019) Emerging medical applications based on non-ionizing electromagnetic fields from 0 Hz to 10 THz. Med Devices (Auckl) 12: 347-368.
- Radzievsky AA, Rojavin MA, Cowan A, Ziskin MC(1999) Suppression of pain sensation caused by millimeter waves: a double-blinded, cross-over, prospective human volunteer study. Anesth Analg 88: 836-840.
- Partyla T, Hacker H, Edinger H, Leutzow B, Lange J, et al. (2017) Remote Effects of Electromagnetic Millimeter Waves on Experimentally Induced Cold Pain: A Double-Blinded Crossover Investigation in Healthy Volunteers. Anesth. Analg 124: 980-987.
- Moazezi Z, Hojjati SMM, Ayrapetyan S (2008) Low-intensity millimeter wave as a potential tool in treatment of diabetic sensorymotor polyneuropathy. Int Dent Med Disord 1: 50-55.
- Mediatkov RS, Vasilenko AM, Arkhipov VV, Kislov Vy, Smirnov VF (1995) Use of a ‘Sharm’therapeutic-diagnostic system in complex therapy of trigeminal nerve neuralgia, p. 83-87.
- Bakaliuk TG, Zoria LV, Pogorila MA (1998) Microwave resonance therapy in primary osteoarthrosis: the pathogenetic validation of its clinical use. Patol Fiziol Eksp Ter 4: 22-25.
- Usichenko TL, Gizhko V, Lysenjuk VP (2008) Pain Relief Effects of Millimeter Waves Applied To Acupuncture. Informacionno analytichekaia Sistema 33(1-2): 59-61.
- Schütze T, Längler A, Zuzak TJ, Schmidt P, Zernikow B (2016) Use of complementary and alternative medicine by pediatric oncology patients during palliative care. Supportive Care in Cancer 24: 2869-2875.
- Wallace DJ, Gotto J (2008) Hypothesis: Bipolar Illness with Complaints of Chronic Musculoskeletal Pain Is a Form of Pseudofibromyalgia. Semin Arthritis Rheum 37(4): 256-259.
- Steward AL, Sherbourne CD, Hayes RD (1992) Summary and discussion of MOS measures. In: AL Stewart and Ware JE (Eds.)., Measuring functioning and well-bring: the medical outcome study approach. DurHam NC, Duke Univ Press, pp. 345-371.
