 Case Report
Case ReportABSTRACT
Background: When we find a head or neck mass in children we quickly think of a vascular malformation because of its frecuency and location. Lipoblastoma is a rare, benign, rapidly growing tumor in infancy and early childhood. This tumor could be presented as a located painless mass in any part of the body, less frecuently in head and neck, or as a diffuse and infiltrating behaviour called lipoblastomatosis.
Case Presentation: This series is about three patients all under 24-months-old with fickle, painless and rapidly growing neck mass. All patients had imaging including ultrasound. In only one case, who need a second intervention we did a magnetic resonance (MRI) to establish the extension of the residual mass. All microscopic análisis confirm lipoblastoma. Almost ten years follow-up did not show recurrences.
Conclusion: Lipoblastoma is an unusual soft tissue tumor. Surgical resection without collateral damage is the best option. Microscopic analysis confirm diagnosis. The purpose of this series is to describe an unusual presentation of a head and neck mass in children.
Keywords: Lipoblastoma; Neck Mass in Children; Case Report
Background
Since 1926, Jaffe used the term lipoblastoma to describe a tumor of immature fat cells located in the groin area [1]. Thirty two years later, Vellios et al. [2] described an “unusual tumor resembling fetal adipose tissue located in anterior wall of the thorax in an 8-monthold- child”; since it differed from hibernoma and other tumors of adult adipose tissue clinically, grossly and microscopically named this as lipoblastomatosis. Chung and Enziger used benign lipoblastoma for circumscribed types and benign lipoblastomatosis for diffuse multicentric type of these tumors [3]. Children Neck lipoblastoma is an unfrequent diagnosis, if we stand beside a toddler with a mass in his neck our first diagnosis is lymphangioma. The aim of this case series is showing our experience in the last ten years.
Case Presentation Section
Case 1
An Eigth-months-old boy presented with a one-month rapidly growing painless, mobile and painless left-sided neck tumor. Ultrasound shows a solid, heterogeneous mass ahead of sternocleidomastoid muscle without contact with cervical large vessels. We decided surgical treatment performing a biopsy of this mass because it had run into the neck without a clear margin to do a complete resection. In the patient’s follow-up we noted a new mass bulge out from the left-side of the neck. Computed tomography (Figure 1) confirmed recurrence. After that, imaging especialits suggest a MRI to establish the extension of the residual mass. A new surgery was performed with a complete wide resection without collateral damage. Findings were compatible with lipoblastoma (Figure 2). Seven years follow-up with clinical examination and imaging did not show any local recurrence.
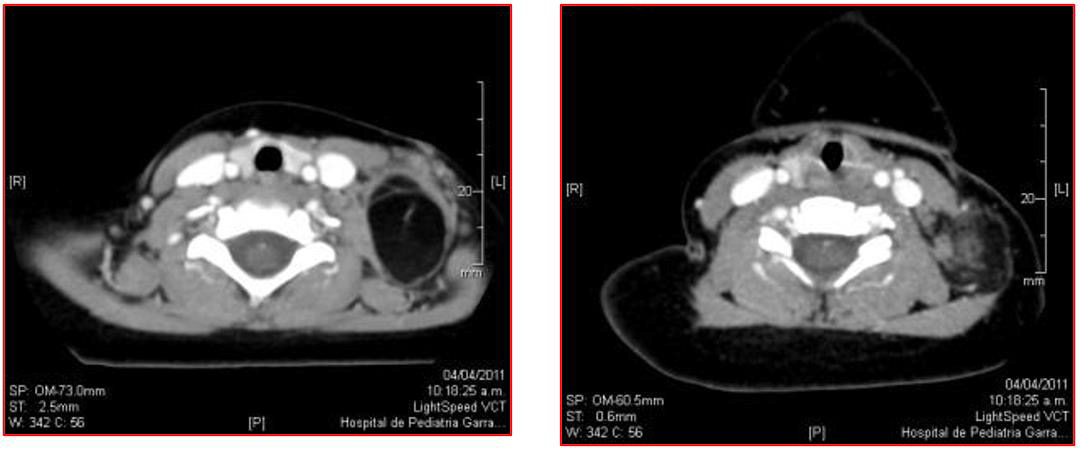
Figure 1: CT Scan showing a big, round, fat-Hounsfield-density, lobulated lesion.
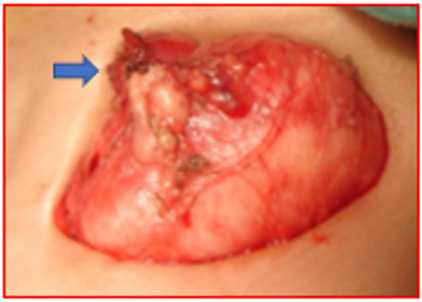
Figure 2: Macroscopic view of a neck lipoblastoma. The tumor is located over the skin in it anatomical position. Look at the root of the mass (blue arrow) that have origin in the neck and expans to the supraclavicular región and the upper chest.
Case 2
A 20-months-old boy presented with an eigth-month progressive growing left-sided neck tumor (Figure 3). Ultrasound showed a solid, heterogeneous 4 inch longitudinal diameter mass in left supraclavicular space. Complete resection with clear margins was performed. Follow-up did not show any recurrence.
Case 3
A 14-months-old boy presented with an only-month rapidly growing left-sided neck tumor. Ultrasound (Figure 4) showed a superficial soft tissue mass with images features similar to lipoma. Complete resection was performed and pathology named it as a lipoblastoma. Margins were uncompromised and he did not show any recurrence in follow-up.

Figure 3: Chest X-Ray of a toddler with a giant cervical mass (red arrow). The tumor doesn`t involve bones only soft tissue without invasion of the thorax.
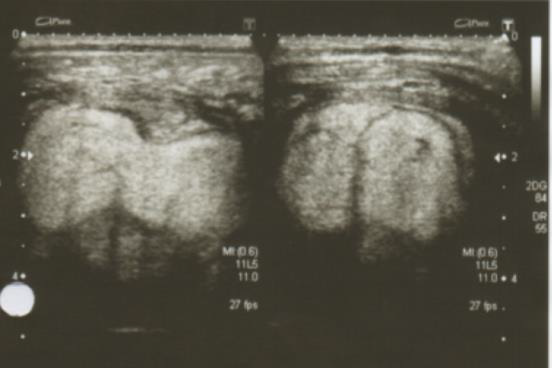
Figure 4.
Discussion
From 2011 to 2021, we described three cases, all younger than two years old, of located soft tissue mass in neck topography. All patients were male consisting with the male preponderance (3:1) reported in literature [4]. All patients have had markers in order to rule out the diagnosis of another cervical tumor like neuroblastoma or teratoma such as Alpha- fetoprotein, human chorionic gonadotrophin and urine catecholamines. This tumor is presented as a lateral cervical rapidly growing, soft mass in all cases. Ultrasound and Computer Tomography shows features similar to lipoma. Imaging is not helpful in diagnosis because it is very difficult to establish the difference between malignant and benign lesions. Preoperative imaging should be used to assess extent of disease and surgical planning [5]. In this series we do not think that was usefull complete the patients study with a CT or MRI previous the surgery because the pathognomonic imaging in US. In case of recurrence we made more sensitive and especific imaging studies in order to know the extent of the disease and compromise of other structures to improve the surgical result trying to be the patient last surgery [6]. One patient of the series had a local recurrence succesfully treated with a second surgery reaching complete resection of the tumor. The goal is always to perform a complete resection with negative margins, but this can be difficult to obtain with lipoblastomatosis. When negative margins are unobtainable, close clinical follow-up with examination and imaging studies is advised. Regardless of margin status, posoperative follow-up in light to document recurrence rate should be done. In our series, we have a seven-year follow up period according to the five-years follow up recommendation [4]. Patients with lipoblastoma have an excellent prognosis despite off the tumor potential for local invasion and rapidly grows up. Metastases have never been reported.
The recurrence rate is 14%, it is more frequent in lipoblastomatosis. There are slender descriptions about children’s head and neck lipoblastoma. In 2006, Sinha BK [7] reported 100 cases in literature with only 10 patients involving cervical region [7]. Other reports described similar numbers ranging between 11 to 30%. In imaging lipoblastoma cannot be distinguished from myxoid liposarcoma but thinking on patients age, liposarcoma is extraordinarily rare in children younger than 10 years old. Fatcontaining lesions of the head and neck are commonly encountered in daily practice. Lipomas, liposarcomas, lipoblastomas, dermoids or teratomas are different entities with similar behavior in imaging methods [8]. Cross sectional imaging using MRI or CT are the mainstay, they provide exquisite detail in head and neck pathologies diagnosis quest (Table 1) Identifying, localizating and characterizing the tumors, imaging helps to establish the extent of local involvement, bone invasion, nodal disease and distant metastasis. Imaging provides critical information for biopsy, surgical resection, chemotherapy or radiation. It plays an important role in the assessment of treatment response and disease recurrence [9]. Microscopically differentiating between this two entities propose a challenge and as a result of that, genetic analysis is necessary [10]: Lipoblastomas may have break-points in the long arm of chromosome 8 (8q 11-13) and liposarcomas typically show either the translocation t(12;16)(q13:p11) with the FUS/ TLS-CHOP chimeric fusión protein or the translocation t(12;22) (q13;q12) with the EWS-CHOP chimeric fusion protein [11]. No atipical lesions were described [12].
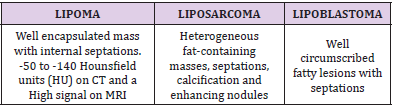
Table 1: Imaging differential diagnosis of head and neck masses.
Conclusion
When we talk about head and neck tumors in children, lipoblastoma is a rare condition that usually confused with lipoma in imaging. We cannot reach a differential diagnosis of a cervical mass showing a rapidly painless growing behaviour within imaging. Therefore, surgical treatment is the best option after ruling out other malignant conditions. Imaging and clinical follow-up is also requested despite off benign condition and the feasibility of the surgical resection.
Declarations
Ethics Approval and Consent to Participate
Not Applicable.
Consent for Publication
Written informed consent were signed by parents of the study participants
Availability of Data and Material
Not Applicable.
Competing Interests
The authors declare that they have no competing interests.
Funding
Not Applicable.
Authors’ Contributions
• DPD: Corresponding Author (conception, desing, acquisition and drafted)
• RJ, PRC, LY, QH and BM take part in surgeries and following of the patients (acquisiton in case series)
• FPS contributed to work desing and analysis in discussion.
• OA is on a fellowship in imaging and interventional radiology. He contributed to the manuscript writting differential diagnosis of head and neck fat-containing masses.
• MC revised the manuscript until sended.
• All Authors read and approved the final manuscript.
Acknowledgement
Special thanks to Prof. Mónica Laporte who provided professional services making possible the correct writing of this case series.
References
- Jaffe RH (1926) Recurrent lipomatous tumors of the groin: Liposarcoma and lipoma psudomyxomatodes. Arch Pathol 1: 381-387.
- Vellios F, Baerz J, Shumaker HB (1958) Lipomatosis. A tumor of fetal fat different from hibernoma. Report of a case with observations of the embryogenesis of human adipose tissue. Am J Pathol 34(6): 1149-1159.
- Chung EB, Enzinger FM (1973) Benign lipoblastomatosis. An análisis of 35 cases. Cancer 32(2): 482-492.
- Speer A, Schofield DE, Wang KS, Shin CE, Stein JE, et al. (2008) Contemporary management of lipoblastoma. Journal of Pediatric Surgery 43(7): 1295-1300.
- Mc Vay M, Keller JE, Wagner CW, Jackson RJ, Smith SD (2006) Surgical management of lipoblastoma. Journal of Pediatric Surgery 41(6): 1067-1071.
- Chun YS, Kim WK, Park KW, Lee SC, Jung SE (2001) Lipoblastoma. Journal of Pediatric Surgery 36(6): 905-907.
- Sihna BK, Thapa N, Banskota DK (2006) Lipoblastoma in head and neck – a rare childhood tumour. Katmandu University Medical Journal 4(1): 94-97.
- Kale HA, Prabhu AV, Sinelnikov A, Branstetter B (2016) Fat: friend or foe? A review of fat-containing masses within the head and neck. Br J Radiol 89(1067): 20150811.
- Ngoc Anh Tran, Jefrey P Guenette, Jyothi Jagannathan (2020) Soft Tissue Special Issue: Imaging of Bone and Soft Tissue Sarcomas in the Head and Neck. Head and Neck Pathology 14(1): 132-143.
- Dilley AV, Patel DL, Hicks MJ, Brandt ML (2001) Lipoblastoma: pathophysiology and surgical management. Journal of Pediatric Surgery 36(1): 229-231.
- Brandal P, Bjerkehagen B, Sverre H (2006) Rearrangement of chromosomal region 8q 11-13 in lipomatous tumours: correlation with lipoblastoma morphology. J Pathol 208(3): 388-394.
- Bruyeer E, Lemmerling M, Poorten V, Sciot R, Hermans R (2012) Paediatric lipoblastoma in the head and neck: three cases and review of literatura. Cancer Imaging 12(3): 484-487.
