 Case Report
Case ReportAbstract
PCL avulsions are rare injuries of the knee joint. What adds even more to the complexity of this injury is the association with other conditions such as Hoffa fractures. The posteromedial knee approach has been suggested as an appropriate approach to posterior tibia plateau, and femoral condyle fragments fixation, however, not many surgeons are familiar with this approach. We present a rare PCL avulsion injury associated with an ipsilateral lateral femoral condyle Hoffa fracture. This case was successfully managed using an uncommon posteromedial knee approach with excellent clinical and radiological outcomes at 18 months follow up. This case was reported in accordance with the CARE guidelines.
Keywords: PCL Avulsion; Hoffa Fracture; Tibia Plateau; Knee; Surgery
Abbreviations: PCL: Posterior Cruciate Ligament; OKS: Oxford Knee Score; TLS: Tegner Lysholm Scores
Introduction
Posterior Cruciate Ligament (PCL) avulsions are rare injuries of the knee joint. What makes this injury even more complex is its association with Hoffa fracture, which is an intra-articular distal femur fracture affecting one or both of the femoral condyles in the coronal plane Hoffa [1] and constitutes around 0.65% of all femur fractures [2]. The posteromedial knee approach has been suggested as an appropriate approach to posterior tibia plateau, and femoral condyle fragments fixation with a safe complication profile and good clinical outcomes [3,4] Yet, not many surgeons are familiar with this approach. A thorough literature review was conducted on PubMed, Web of Science and Google Scholar till July 2021. It is to the best of our knowledge that no such cases with this combination of injuries and this surgical approach have been reported in the literature before. This case report presents an unusual PCL avulsion injury associated with an ipsilateral lateral femoral condyle Hoffa fracture. Also, we highlight our surgical treatment and patient’s clinical, functional, and radiological outcomes 18 months following management of this unique injury pattern.
Case Report
A 35-year-old gentleman sustained a road traffic accident after developing an epileptic generalized tonic-clonic seizure while driving his car. He complained of severe left knee pain and swelling. On physical examination, the patient was hemodynamically stable, conscious, and oriented. The left injured knee was moderately tender, swollen, with superficial abrasions anteriorly. The range of motion was limited to 0-30 degrees of extension-flexion. Also, he had tenderness over the lateral femoral condyle area. Varus stress test was suggestive of grade 2 injury of lateral collateral ligament of the left knee. The posterior drawer test could not be assessed at that time due to the severity of pain but tested positive intraoperatively. All compartments were soft with intact lower limbs neurovascular exam. Preoperative radiological evaluation with plain radiographs & CT scan of the left knee revealed a comminuted tibial plateau fracture extending posteriorly with multiple intra-articular fragments, comminuted Hoffa fracture of lateral condyle of the left femur (Figures 1 & 2).

Figure 1: Preoperative AP & Lateral X-rays.
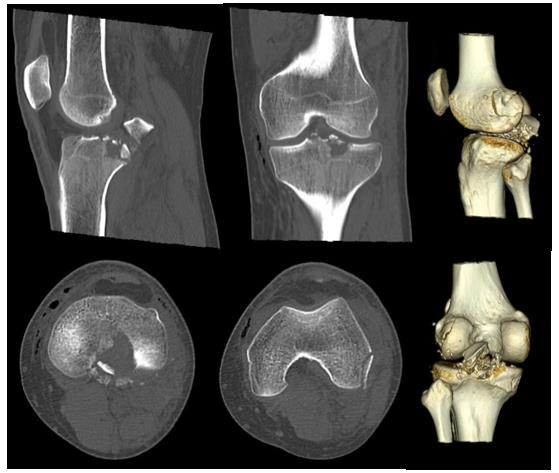
Figure 2: Preoperative knee CT scan.
Open reduction and internal fixation of left PCL avulsion and lateral femoral condyle fractures was performed by a senior knee orthopaedic surgeon at a trauma 1 center. In prone position and after scrubbing, prepping and draping the left lower limb, a proximal thigh tourniquet was inflated. Then a posteromedial knee approach was taken as described by Burks and Schaffer [5]. First, the PCL avulsed fragment was reduced and fixed with one 3.5 millimeters lag screw and a washer. Next, another posterior lateral 1 x 3 cm fragment was fixed using a 3.5 mm lag screw. Finally, a backup fixation was done with No.5 non-absorbable braided suture in the PCL and tied around the screw and washer. Furthermore, a small posterolateral incision, as an extension of the posteromedial approach in a lazy “S” fashion, was made on the left lateral femoral condyle, and a shell of bone was fixed with two headless 3.5 mm screws. Special knee tests were negative at the end of the procedure. Fluoroscopy confirmed excellent reduction and hardware placement.
Outcome & Follow-up
The patient was observed for a total follow-up period of 18 months following surgery and had frequent clinic visits at 1, 6, 12 and 18 months with the following findings (Table 1). Thorough clinical and radiological assessment was done in each visit, validated knee functional outcome scores including Tegner activity, Lysholm score and Oxford knee score (OKS) were utilized. Radiographic and bed side images at final follow up are shown in Figures 3 & 4, respectively.

Figure 3: Final AP & Lateral X-ray at 18 months follow-up.
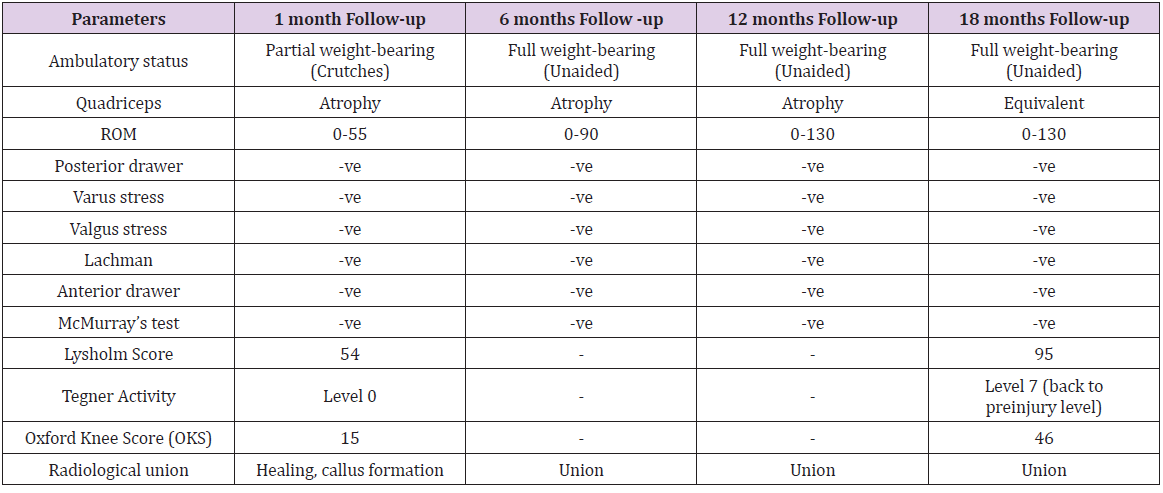
Table 1: A summary of the postoperative follow up parameters. PWB: Partial weight bearing. FWB: Full weight bearing.

Figure 4: Clinical images at the final follow-up period of 18 months postoperatively.
Discussion
PCL avulsion fractures are rare and challenging injuries. While the best treatment options remain controversial, poorly treated PCL avulsions might lead to debilitating long term consequences of an unstable knee, malunion and nonunion [6,7]. These fractures can also be associated with other bony and ligamentous injuries around the knee joint, increasing surgical complexity. PCL avulsion fractures often have a similar mechanism of injury to PCL intrasubstance tears, such as dashboard injury, where an anteroposterior force applied to a flexed knee and sports traumatic injuries with a knee in hyperextension position [8]. Also, Hoffa and tibial plateau fractures are associated with high-energy trauma such as motor vehicle accidents, particularly in the younger population. While non-operative management could be considered in some PCL avulsion cases with minimal displacement of less than 5mm [9], most surgeons advocate for surgical fixation, taking into account various factors including fracture characteristics, displacement, comminution, and associated injuries [10,11]. The use of posteromedial knee approach has been reported in the literature with some technical variations, however, a recent paper describe the method used in our case and showed excellent radiological and functional outcomes [12] (Figure 5).

Figure 5: Intraoperative clinical image of the posteromedial knee approach used (from a previous case).
Patient Perspective
“After the horrific accident and how badly injured I was, I never thought I will be back on my legs walking. I’m really thankful to have reached this level of activity and getting back to my normal life”
Conflict of Interest
The author(s) declare that they have no competing interests.
Authors Contribution
LS was involved with the clinical follow up, data collection, drafting, reviewing, and editing of the manuscript. MS & EB were involved with performing the surgery, clinical follow up, data collection, drafting, reviewing, and editing of the manuscript. MA is the senior who performed the surgery and was involved with reviewing and editing of the manuscript. All contributors met the ICMJE and journal criteria for authorship and approved the final manuscript.
Funding
None.
Ethical Approval
MRC-04-21-691
Informed Consent
Obtained.
Acknowledgement
None.
References
- Hoffa A (1904) Lehrbuch der frakturen und Luxationen für Ärzte und Studierende: Enke.
- Mandredini M, Gildone A, Ferrante R, Bernasconi S, Massari L (2001) Unicondylar femoral fractures: therapeutic strategy and long-term results. A review of 23 patients. Acta orthopaedica belgica 67(2): 132-138.
- Bali K, Prabhakar S, Saini U, Dhillon MS (2012) Open reduction and internal fixation of isolated PCL fossa avulsion fractures. Knee Surg Sports Traumatol Arthrosc 20(2):315-321.
- Lamichhane A, Mahara D (2012) Management of posterior cruciate ligament avulsion by cannulated screw fixation. Journal of Institute of Medicine Nepal.
- Burks RT, Schaffer JJ (1990) A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop Relat Res 254: 216-219.
- Gwinner C, Hoburg A, Wilde S, Schatka I, Krapohl BD, et al. (2016) All-arthroscopic treatment of tibial avulsion fractures of the posterior cruciate ligament. GMS Interdisciplinary plastic and reconstructive surgery DGPW 5: 02.
- Logan M, Williams A, Lavelle J, Gedroyc W, Freeman M (2004) The effect of posterior cruciate ligament deficiency on knee kinematics. Am J Sports Med 32(8):1915-1922.
- Hooper PO, Silko C, Malcolm TL, Farrow LD (2018) Management of Posterior Cruciate Ligament Tibial Avulsion Injuries: A Systematic Review. Am J Sports Med 46(3): 734-742.
- Zhao J, He Y, Wang J (2006) Arthroscopic treatment of acute tibial avulsion fracture of the posterior cruciate ligament with suture fixation technique through Y-shaped bone tunnels. Arthroscopy 22(2): 172-181.
- Katsman A, Strauss EJ, Campbell KA, Alaia MJ (2018) Posterior cruciate ligament avulsion fractures. Current Reviews in Musculoskeletal Medicine 11(3): 503–509.
- White EA, Patel DB, Matcuk GR, Forrester DM, Lundquist RB, et al. (2013) Cruciate ligament avulsion fractures: anatomy, biomechanics, injury patterns, and approach to management. Emerg Radiol 20(5): 429-440.
- Babikir E, AlKhayarin M, Asad W (2021) Posteromedial Approach to Fix Posterior Cruciate Ligament Tibial Avulsion: A Backup Fixation and Case Series. J Orthop Surg Tech 4(1).
