 Research Article
Research ArticleSUMMARY
Medication Gingival Hyperplasia is described as an abnormal, exaggerated and deforming increase in gum volume, caused by the intake of some medications. Among the most common are: anticonvulsant drugs, antihypertensives, particularly calcium antagonists and immunosuppressants, but cases reported by Carbamazepine are very rare. We presented the case of a male patient, 33 years old, with a history of Epilepsy and Mild Mental Retardation who after approximately 10 years of carbamazepine consumption, goes to a stomatological consultation due to an increase in the volume of the gums in the maxilla and canker sores in the mucosa of the carillo, clinically compatible with Gingival Drug Hyperplasia and Recurrent Aphthous Stomatitis. After discontinuation of the causative drug and drug treatment both lesions disappeared. Although the concomitance of these two diseases is not usual, it was observed that they can occur simultaneously.
DeCS
Drug Gingival Hyperplasia, Recurrent Aphthous Stomatitis, Epilepsy, Carbamazepine
Keywords: Gingival/Chemically Induced Enlargement; Anticonvulsants/Adverse Effects; Canker Sores
Introduction
Epilepsy is a chronic disease characterized by recurrent seizures and due to sudden, hypersynchronous discharges of neurons from the cerebral cortex [1]. In a patient with epilepsy, the incidence of infections, post-surgical gingival hemorrhage and delayed healing, caused by the drugs they consume, is higher. Several drugs have been used in the treatment of this disease, known as anticonvulsants, but there are adverse reactions at the stomatognathic level related to its systemic use, such as Gingival Drug Hyperplasia (Figure 1) (HGM); this term is used to refer to the exaggerated and disfiguring increase in gum volume caused by some medications [2].Of imprecise etiology, an incidence between 4-7% is estimated [3] and within its clinical expression is observed: painless, globular and mobile enlargement, pale pink that can also be observed reddish and bleeding when there is an infection or overadded inflammation [4] The first description of a drug that caused gingival enlargement was reported in 1939 and was associated with the use of Phenytoin, [5] also over the years has been linked to the administration of other drugs: anticonvulsants, immunosuppressants and calcium channel blockers [6].
Among the most common antiepileptics associated with Hyperplasia are known: valproic acid, carbamazepine, phenobarbitone and vigabatrin [7]. Various risk factors are recognized, such as: age, sex, pharmacological variables, concomitant medication, genetic factors and periodontal and oral variables [8]. On the other hand, it is not usual to observe the concomitance of HGM with Recurrent Aphthous Stomatitis (EAR), which is also known as aphthous ulcers and is considered the most common of the lesions of the oral mucosa since it affects about 20% of the general population [9]. Patient information: Male patient of 33 years of age, single, level of schooling 6th grade, with incoordination of movements of the limbs, unoccupied, who goes to the emergency room accompanied by his mother who is also his full-time caregiver (Figure 2). The patient reports that days before going to the consultation he felt itching and pain in the cheek, his mother affirms that at that time he already had a slight increase in volume in the affected area but that he did not give it importance because he had been like this for days, he assumed that it was a dentoalveolar abscess and was sure that with antibiotics he would resolve.
Figure 1: Diagram Alterations caused by Gingival Drug Hyperplasia.

Figure 2: Oral thrush in the cheek and gingival enlargement due to the consumption of Carbamazepine.
Physical Examination
constitution of longylinear type that wanders with difficulty, white complexion, without proportionality between 3 thirds of the face, bilateral facial symmetry, pathological facies, wide oral opening, incompetent bilabial closure, face: oval, profile: straight, upper and lower internal midline that coincide with the facial midline, Temporomandibular Joint (TMJ) (Table 1) without apparent alterations, non-reactive neck ganglion chains. Intraoral Examination: gingival enlargement of approximately 2 cm located in marginal gum of 12-13, bluish-red, globular, depressible, mobile, with a tendency to hemorrhage due to overadded inflammation. Loss of gingival and dotted morphology, hypocolored and fibrous gums. Yellowish ulcer on the right side of 1 cm, painful, with imprecise edges and erythematous halo. Presence of PDB that yielded as Love Index = 43%. Fillings in 16 and 24, dyschromia in 11 associated with childhood (Table 2) trauma that was treated with TPR at 12 years of age, diastema between 22 and 23, missing teeth not restored: 25, 34, 37, 46, residual alveolar edges: ovoid, halitosis is observed. Diagnostic evaluation: The diagnostic methods used were the physical examination and the clinical method. It was struck in the teeth of the affected area without positive responses to horizontal or vertical percussion (Table 3).
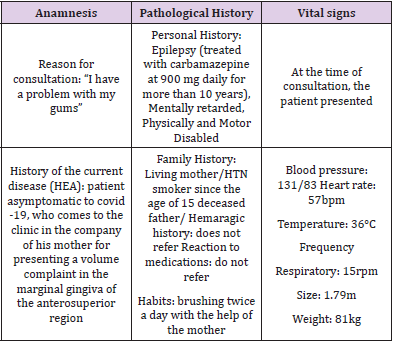
Table 1: Anamnesis data of the case in question.
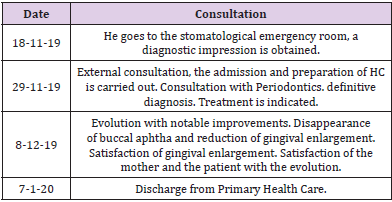
Table 2: Calendar.
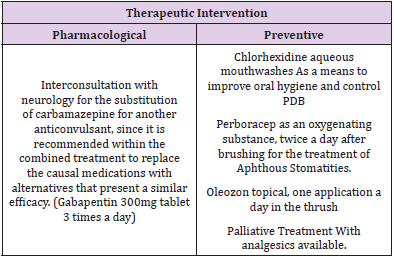
Table 3: Therapeutic intervention.
Diagnosis
Carbamazepine Drug Gingival Hyperplasia and Recurrent Aphthous Stomatitis.
Diagnostic Reasoning
The predisposing systemic factor was the administration of Carbamazepine for the treatment of Epilepsy. This drug acts through the stabilization of neuronal membranes [10] and it is known that the appearance of ulcers in the oral mucosa are usually signs of hematological toxicity. Among its clinical uses are: as a treatment of trigeminal and glossopharyngeal neuralgia [11]. The consumption of anticonvulsants for a long time can stimulate a proliferation of fibroblasts, [12] in addition to producing hyposialia, delayed healing, leukopenia, thrombocytopenia and ataxia. In the mechanism of onset of the disease involve the metabolism of the drug depending on the individual characteristics of the patient [13].
Prognosis
Favorable.
Discussion
According to Zerón and Sautto [13] when they try to explain the behavior of HGM, they affirm that enlargement facilitates the accumulation of plaque, which causes secondary inflammation, stimulates the proliferation of gingival fibroblasts and potentiates collagen metabolism; in turn, the plaque would act as a reservoir for the drug and increase the severity of the enlargement. The relationship between the time of administration and the onset of HGM depends on the drug used and the time of consumption, for example: Manzur et al [8] state that after 9 months they have reported the onset of signs in patients treated with nifedipine, and between 1-3 months after the ingestion of phenytoin. In contrast, in patients treated with Carbamazepine, it is only occasionally observed, although it is used more frequently. A recent study in Villa Clara, Cuba shows a frequency of 2.2% in epileptic patients [2]. On the other hand, we did not find updated articles on EAR and Epilepsy, although it has been shown that the consumption of Carbamazepine sometimes causes aphthous lesions or ulcers. Stomatitis is characterized by the appearance of prodromal symptoms such as: feeling of hyperesthesia, inflammation, burning, stinging and pain; and after 24 hours give way to vesicles that when broken form yellowish ulcers, red margins and variable size that can occur anywhere in the oral mucosa [14].
Canker sores usually resolve within one to two weeks in most patients. They usually appear in childhood and adolescence, they recur less frequently and severely when patients age. The incidence varies from 5-60% [15].
Final Considerations
Currently, the number of drugs associated with HGM has increased. Its development and severity are a consequence of a multifactorial mechanism. The recognition of the different risk factors among which stand out: poor hygiene with the consequent accumulation of microbial biofilm, the association of drugs, the various expressions of individual susceptibility and genetic predisposition, are important in the control and systematic monitoring of these patients from a multidisciplinary perspective.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authorship Contribution
All the authors participated in the elaboration of the article and approved the final text.
References
- Valdés Herrera MA (2013) 27: Atención al paciente especial. In: González Naya G, Montero del castillo ME (Eds.)., ME. Estomatología General Integral. Havana: ECIMED, pp. 350.
- Montes de Oca González AM, González Falcón M, Veitia Cabarrocas F, Lahera Fernádez EL, Díaz López OB, et al. (2020) Agrandamiento gingival medicamentoso en pacientes que padecen hipertensión, cardiopatías y epilepsia. Acta Médica del Centro 15(1): 72-80.
- Ramírez Rámiz A, Brunet LLobet L, Lahor-Soler E, Miranda-Riu J (2017) On the cellular and molecular mechanisms of drug-induced gingival overgrowth. OpenDentJ 11: 420-435.
- García Reguera O, Corrales Alvarez M, Padrón Alonso M, González Díaz ME, Toledo Pimentel B, et al. (2017) 5: Diagnóstico, pronóstico y tratamiento de la enfermedad periodontal no inflamatoria. Compendio de Periodoncia. (2nd)., Havana. ECIMED, pp. 274.
- Martínez FC, Segura Ruiz F, Cicco SE (2015) Manejo del paciente epiléptico en la consulta odontológica: Revisión actualizada de la literatura. Acta Odontológica Venezolana 53(2).
- Manzur-Villalobos I, Díaz-Rengifo IA, Manzur-Villalobos D, Díaz-Caballero AJ (2018) Agrandamiento gingival farmacoinducido: Serie de casos. Univ Health 20(1): 89-96.
- Córdova García DP, Zatarain G, Reyes A, Díaz E, Pietshmann A (2020) Agrandamiento gingival inducido por fenitoínas . Rev ADM 77(6): 316-320.
- Bann AAl-Hazmi (2018) Management of Nifedipine-Induced Gingival Overgrowth with Drug Substitution: A case report. Dental Science 17(5): 600-605.
- Boza Oreamuno YD, Rugama Flores MF (2019) Estomatitis aftosa recurrente y deficiencias nutricionales: Reporte de tres casos y revisión de literatura. ODOVTOS. Int J Dental Sc 21(3): 33-43.
- (2021) Carbamazepine CIMA.
- (2016) Carbamazepine. Formulario Nacional de Medicamentos (FNM).
- Simancas Escorcia V, Díaz Cabellero A, Vergara Hernández C (2020) Survival of human fibroblastic cells in the absence of supplementation. NOVA 18(34): 47-56.
- Zerón GVJA, Sautto M (2016) Agrandamientos gingivales inducidos por medicamentos. Una visión genómica y gené Revisión de la literatura. Rev Mex Periodontol 7(1): 25-35.
- Veitía Cabarrocas F, González Díaz ME,Toledo Pimentel B, Morales Aguilar DR, Samper HR Diagnosis, prognostic and Compendium of Periodontics (2nd)., ECIMED, pp. 163-165.
- Grave de Peralta Hijuelos M, Páez González Y, Tamayo Ávila Y, Martínez Pérez M, Ochoa Pérez D (2019) Diagnosis and pathogenesis of recurrent aphthous stomatitis. MCC 23(3): 1-21.
