 Research Article
Research ArticleABSTRACT
Objectives: Immune-related genes play an important role in predicting tumor survival, monitoring the state of tumor immune microenvironment, tumor immune escape and immunotherapy. However, lung cancer (LC) is one of the most common malignant tumors, and its incidence rate and mortality have increased year by year. Lung adenocarcinoma (LUAD) is the main subtype of LC. Therefore, it is particularly important to explore the role of immune - related genes in LUAD.
Methods: Transcriptome data from The Cancer Genome Atlas (TCGA) and immune gene data from Immunology Database and Analysis Portal (ImmPort Portal) and Systems Biology of the Innate Immune Response(innateDB) were collected, anddifferentially expressed immune-related genes wereanalysed. Based on survival related immune-related genes (IRGs) and COX regression analysis, an immunerelated gene-based prognostic index (IRGPI) was established. Transcriptome data from GEO database were analyzed to verify the accuracy of the model. The predictive capacity of IRGPI was evaluated using a Kaplan-Meier Curve and Receiver Operating Characteristic Curve (ROC). Tumor Immune Dysfunction and Exclusion (TIDE) is used to predict lung adenocarcinoma immunization and immunotherapy mechanism.
Results: Data of 535 lung adenocarcinoma tissues and 59 normal tissues were obtained from TCGA database, and 8108 immune-related genes and 683 immunerelated differentially expressed genes were screened from these data. IRGPI based on 32 survival-related IRGs (CD79A, IGHM, IGKC, CTLA4, CD27, S100B, TLR8, PTX3, ARG2, FGR, LILRB3, NHA, LGR4, FCN1, DUOX1, AGER, SEMA3A, CX3CR1, FGF14, HDGF, PDGFB, ANGPTL4, PTH1R, TEK, SHC3, DCN, HSPD1, FLI1, PLK1, C7, C6, PRKCE) was determined and used to predict the total survival of patients with LUAD.The IRGPI of LUAD was correlated with clinical stage, differential immune cells and immune-related functions affecting patient survival (p<0.05).
Conclusion: The discovery of lung adenocarcinoma characteristics and immunerelated genes is found to provide a new insight for immune mechanisms, as well as a new prognostic biological marker for patients with LUAD.
Keywords: Lungadenocarcinoma (LUAD); Bioinformatics; Immune-Related Gene (IRGs); Prognostic Index; Tumor Microenvironment (TME)
Introduction
Although the treatment of lung adenocarcinoma (LUAD) has improved in surgery [1], chemotherapy [2], radiotherapy [3] and targeted therapy [4], the five-year survival rate is still lower, at around 15% [5]. Metastasisand recurrence of LUAD are still difficult problems in the course of treatment [6,7]. In order to improve the survival rate of LUAD, the patient’s prognosis should be closely monitored, and the treatment plan should be adjusted in time, so a separate prognosis indicator is required to assess the patient’s clinical state. Tumor microenvironment (TME) is the internal environment for the generation and survival of Tumor cells [8-10]. The occurrence of tumor is closely related to immune cell infiltration in TME, and it is necessary to escape the anti-tumor immune response in order to grow rapidly [11-13]. Analysis of the characteristics of TME can be helpful for clinical immunotherapy. TIDE uses a suite of gene expression markers to assess two different tumor immune evasion mechanisms, including tumor-infiltrating cytotoxic T lymphocyte dysfunction and rejection of cytotoxic T lymphocyte by immunosuppressive factors [14,15]. It has been shown that TIDE score can more accurately predict the prognosis of melanoma patients treated with immunotherapy [16]. TIDE is a calculation method using gene expression profile to predict tumor immune checkpoint (ICI) response. Patients with higher TIDE score have a higher chance of tumor immune escape and a lower response rate to ICI treatment [14]. Although there are several studies on LUAD based on immune-related genes [17,18], there is an urgent need for a more comprehensive and reliable indicator that can simultaneously predict survival and immunotherapy efficacy in LUAD patients. Therefore, based on tumor genomics and bioinformatics analysis, we attempted to develop an IRGPI for LUAD to provide a basis for predicting survival, prognosis and immunotherapy effect of LUAD.
Methods
Sample Clinical Information and Data Collection
Transcriptome data and clinical information of LUAD samples were downloaded from TCGA and GEO as test sets and validation sets, respectively [19,20]. Immune-related genes were downloaded from Immport and INnatedB databases [21].
Screening of DEGs and IRGs
DEGs were screened by comparing LUAD with normal samples using R packet “Limma”.The genes of | log2 (Fold Change) |> 1 and FDR (False Discovery Rate, FDR) <0.05 were screened as DEGs [22]. Then, IRGs is extracted from the identified DEGs list and heat maps of DEGs and IRGs are generated through R package “PhatMap”. GO and KEGG enrichment analysis was performed by R packages “GOplot” and “GGplot2”, and bubble graphs and bar graphs were generated [23,24].
Screening of Weighted IRGs Genes Associated with Survival
Weighted gene co-expression analysis was performed by R package “Limma” and “WGCNA”, and dendritic and module diagrams were generated. Then, r-package survival was used to analyze the survival of all differentially expressed IRGs, and univariate Cox analysis was used to determine the IRG associated with survival (P<0.05). According to the risk ratio, the forest map is generated [25].
Development and Assessment of IRGPI
The survival- related IRGS is multivariable analysis to develop IRGPI.IRGPI is established by multiplying the expression value of the IRGS of the multivariable analysis with the COX regression coefficient [26]. After that, Patients were then divided into highrisk and low-risk groups based on the comparison of IRGPI values with median. Kaplan-meier (KM) survival curves were constructed to verify the overall survival in different risk groups [27], and ROC curves were established according to TIDE and TIS to evaluate the sensitivity and specificity of the models [28]. GSEA enrichment analysis of IRGPI was performed using R package “enrichplot” [29]; Single-factor and multi-factor independent prognostic analysis was performed using R package “survival” [30]; Clinical correlation heat maps were prepared using R package “ComplexHeatmap” [28].
Evaluation of Tumor Immune Cell Infiltration
R pack “reshape2” and “ggpubr” were used to analyze the difference of immune cells in IRGPI high and low risk groups. Similarly, R pack “survival” and “survminer” were used for its functional analysis. Next, R package “GSVA” was used to analyze the differences of immune-related functions in IRGPI high-low risk groups, and R package “SurvMiner” was also used to conduct its functional analysis [31].
Calculation of TIDE and TIS
TIDE score was calculated on TIDE website(http://tide.dfci. harvard.edu/login/, and TIS score was obtained by calculating the average value of Log2-Scale Normalized expression of 32 genes [32].
Statistical Analysis
Cox regression analysis was used for multivariate survival analysis. Bilateral P values < 0.05 were considered statistically significant. Independent T test was used to compare the differences between different clinical parameters between the two groups Univariate survival analysis kaplan-Meier survival analysis with log-rank test was performed.
Result
Screening and Functional Analysis of Differentially Expressed Immune-Related Genes
Screening and functional analysis of differentially expressed immune-related genes A total of 8108 differentially expressed genes were obtained in differentially expressed analysis (535 tumor samples and 59 normal samples), of which 1864 genes were down-regulated and 6244 genes were up-regulated (Figure 1A). The intersection of these genes with immune-related genes yielded 682 differentially expressed immune-related genes, of which 258 genes were down-regulated and 424 genes were upregulated (Figure 1B). In order to explore the biological function of differentially expressed IRGs, GO enrichment analysis and KEGG enrichment analysis were conducted for differentially expressed IRGs(n=682). The genes most related to BP,CC and MF are the humoral immune response(Figure 1C), immunoglobulin complex (Figure 1E), and activation of signal receptor factor activity (Figure 1E), respectively. Cytokine-cytokine receptor interaction is the most important signaling pathway (Figures 1D,1G,1H).
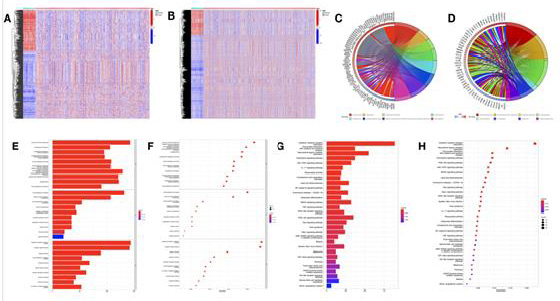
Figure 1: Screening and functional analysis of differentially expressing immune-related genes.
(A) TCGA differential gene heat map;
(B) TCGA immunotrophism differential gene heat map;
(C) GO enrichment analysis ring map;
(D) GO enrichment analysis column;
(E) GO enrichment analysis bubble map;
(F) Kegg enrichment analysis ring map;
(G) KEGG enrichment analysis histogram;
(H) KEGG enrichment analysis bubble map.
Construction and Verification of IRGPI
Based on the cluster analysis of genes, the WGCNA analysis identified 7 highly correlated modules between patients (Figures 2A & 2B). The module genes with P <0.05 were selected for prognostic analysis, and 95 immune-related genes related to LUAD patients’ OS were obtained, among which 28 genes had HR>1 and 67 genes had HR<1 (Figure 2C). IRGPI values based on TCGA database information were used as validation sets to determine the survival rate of LUAD patients (Figure 2D). Similarly, GEO database information is used as a test set to verify the rationality of IRGPI values (Figure 2E). It was found that in both data sets, the OS of high-risk patients was lower than that of low-risk patients (P <0.05). In order to evaluate the prediction accuracy of IRGPI established in this paper, ROC curve was generated and AUC was calculated (Figures 2F & 2G). The areas under the ROC curve of patients at one, three and five years were 0.753,0.761 and 0.778, respectively, indicating that the proposed IRGPI has advantages in monitoring the prognosis of patients.
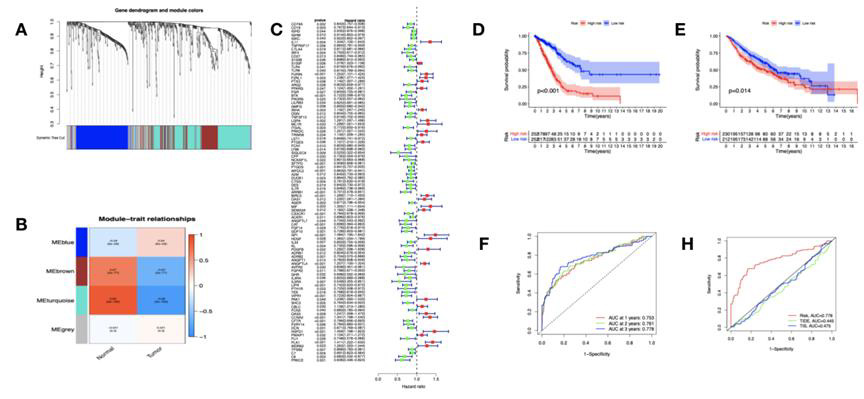
Figure 2: Construction and validation of prognostic indicators of immune-related genes.
(A) WGCNA tree branch map;
(B) WGCNA module diagram;
(C) OS-related IGRs forest maps;
(D) K-M survival analysis of test set IRGPI;
(E) K-M survival analysis of validation set IRGPI;
(F) Survival related ROC curve validation of THE prognostic value of RGPI for TIDE score;
(G) Survival related ROC curve validation of the prognostic value of RGPI for TIS score.
IRGPI Evaluation
The differentially expressed immune-related genes in the model were involved in GSEA enrichment analysis. IRGPI highrisk samples gene sets in cancer and tumor transfer related paths (Figure 3A), and the gene set of IRGPI low risk samples is enriched in DNA replication related pathways (Figure 3B). To verify the independent prognostic value of IRGPI, univariate and multifactorial independent prognostic analyses were performed (Figures 3C & 3D). The prognosis of LUAD was significantly correlated with tumor stage. Further analysis of the correlation between IRGPI and clinic showed that IRGPI was correlated with tumor stage (Figure 3E), and IRGPI was correlated with tumor stage in high and low risk groups (Figure 3F).

Figure 3: IRGPI assessment.
(A) GSEA enrichment analysis of IRGPI in low-risk group;
(B) GSEA enrichment analysis of IRGPI in high-risk group;
(C) Univariate Cox regression analysis;
(D) Multivariate Cox regression analysis;
(E) IRGPI and clinical correlation;
(F) IRGPI and clinical correlation in the high and low risk group.
Immune Cell Analysis of Differences Affecting Survival in Patients With LUAD
In order to assess whether IRGPI can accurately reflect the state of tumor immune microenvironment, we analyze the relationship between IRGPI and immune cell infiltration Results show that the IRGPI is associated with a significant difference was found in 6 kinds of immune cells, including Plasma cells, Monocytes, Macrophages M0, Dendritic cells resting, Mast cells resting,Mast cells activited (Figure 4A). There are 9 immune cells associated with LUAD survival, including B cells naïve (Figure 4B), Plasma cells (Figure 4C), T cells CD4 memory activated (Figure 4D), NK cells resting (Figure 4E), Monocytes (Figure 4F), Macrophages M0 (Figure 4G), Macrophages M1 (Figure 4H), Neutrophils (Figure 4I), Dendritic cells resting (Figure 4J).
Analysis of Immune-Related Function Differences Affecting Survival in Patients With LUAD
To determine the major immune-related functions of IRGPI in the high and low risk groups, differences and survival analyses were performed.High and low-risk group IRGPI and 13 immunocytocytes related functions, including aDCs,B cells,DCs,HLA,iDCs,Mast cells,Neutrophils,pDCs,T cell co-inhibition,T cell (Figure 5A) costimulation, T hepler cells,TIL,Type II IFN response . There are 21 immune-related functions related to LUAD patient survival, including pDCs (Figure 5B), Type II IFN response (Figure 5C), Type I IFN response (Figure 5D), TIL (Figure 5E), Th1 cells (Figure 5F), Tfh (Figure 5G), T hepler cells (Figure 5H), T cell co-inhibition (Figure 5I), Parainflammation (Figure 5J), NK cells (Figure 5K). Diagram illustrates the top 10 immune related functions.
ICI Treatment for High and Low Risk Group IRGPI
To assess the potential clinical efficacy of immunotherapy in the high-low risk group of IRGPI, we performed TIDE analysis on the data.Results showed that the TIDE prediction score of IRGPI in the high-risk group was lower than that in the low-risk group (Figure 6A), suggesting that patients were more likely to benefit from ICI treatment, less likely to escape the immune system, and better prognosis.It has also been found that high-risk group IRGPI has a high Exclusion (Figure 6D), while low-risk group IRGPI has a high dysfunction (Figure 6C). However, there was no difference in microsatellite instability (MSI) scores between the high and low risk groups (Figure 6B).

Figure 4: Differences and survival analysis of immunocytocytes in IRGPI.
(A) IRGPI high and low risk group immunocytocytes; (B) b cells naive; (C) Plasma cells; (D) T cells cd4 memory activated; (E) NK cells resting; (F) Monocytes; (G) Macrophages M0; (H) Macrophages m1; (I) Neutrophils; (J) Dendritic cells resting.
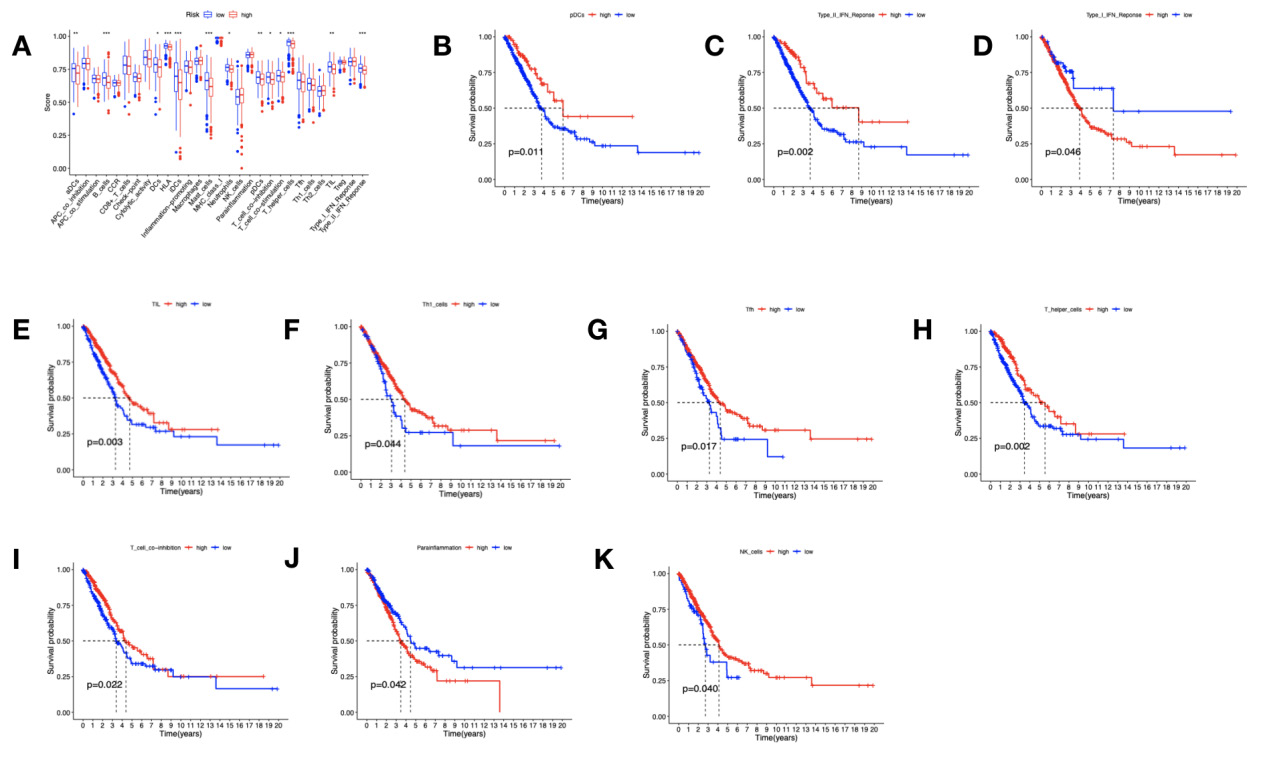
Figure 5: Differences in immune-related functions and survival analysis.
(A) Differences in immune-related functions; (B) B cells; (C) CD8+; (D) HLA; (E) iDCs; (F) inflammation; (G) Mast cellls; (H) MHC class I; (I) T hepler cells; (J) TIL(K)Type II IFN reponse.
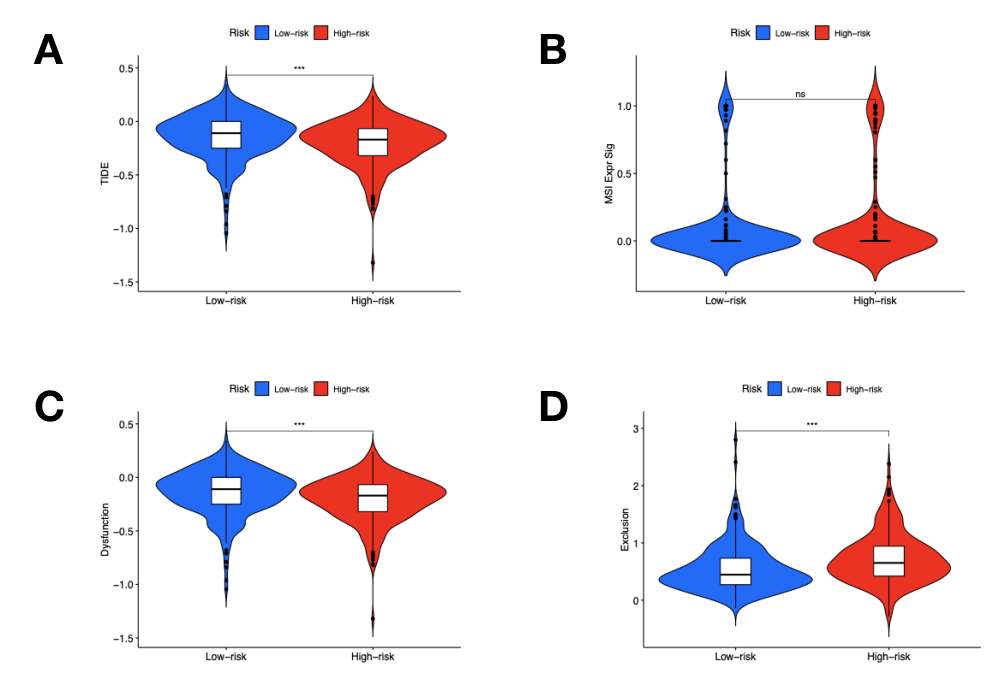
Figure 6: Immune escape and immunotherapy.
(A) TIDE; (B) MSI; (C) Dysfunction; (D) Exclusion.
Discussion
The development of cancer immunotherapy and targeted drugs has led to a more precise and personalized treatment for LUAD [33- 35]. To ensure the prognostic effect of immunotherapy in patients with lung adenocarcinoma, we established an IRGPI that can be used to evaluate and detect the immune response in patients with LUAD, so that it can be used as a biomarker of LUAD immunotherapy and benefit from ICI treatment. According to the results obtained by us, among the differentially expressed IRGs, the most relevant BP is that the differentially expressed IRGs of humoral immune response is significantly correlated with the interaction between cytokine and cytokine receptor, suggesting that LUAD patients are related to the immune response. In recent years, cancer immunotherapy has been gradually applied in clinical diagnosis and treatment [36]. and various types of bioinformatics analysis can identify prognostic biomarkers and their potential mechanisms [37]. For example, Xin Lin et al. used a combination of bioinformatics methods and LUAD prognostic status to show that patients in a group of patients with advanced NSCLC benefited from radiotherapy [38]. There are also researchers to predict the prognosis of lung cancer using bioinformatics to analyze the expression spectrum gene of lncRNA, miRNA or mRNA [39-41].
In this study, a biomarker based on immune-related genes was found, which is suitable for reflecting the immune status and tumor prognosis of LUAD patients. To establish this biomarker, Cox regression analysis was used to integrate the expression levels of IRGs associated with survival. Finally, 32 central genes out of 95 genes were extracted to construct predictive models, and the risk scores of LUAD patients were calculated. Based on these scores, patients in the analyzed samples were divided into high risk group and low risk group. In TCGA and GEO cohort, patients with high IRGPI had worse survival, while patients with low IRGPI had better survival Comparing our IRGPI with other models, we found that our model’s large area under the ROC curve proved to be an effective prognostic immune-related biomarker and was effective in predicting survival. Considering the cancer is closely related to immune, clinical treatment of tumor immune microenvironment [42-45]. IRGPI must be considered and immune cell infiltration between the relevant assessment can be used to reflect the state of microenvironment [46-47]. Here, we show that IRGPI and Plasma cells, Monocytes, Macrophages The infiltration level of M0 was significantly correlated (P <0.05), and it was mainly enriched in immune-related functions such as pDCs,Type II IFN, REponse and TIL.
These immune cells and immune-related functions played a very important role in the prognosis of LUAD [48-49]. Although tumor immune dysfunction and exclusion (TIDE) analysis focuses on the function and state of T cells and cannot fully reflect the complexity of TME’s involvement in immunotherapy response, TIDE can still predict the patient’s response to immunotherapy [50]. TIDE score has been proved to be able to accurately predict the impact of immunotherapy on the prognosis of melanoma patients and head and neck squamous cell carcinoma patients [16,49]. In our study, TIDE score showed statistical difference in the high and low IRGPI risk group, and the high IRGPI risk group was mainly manifested in immune dysfunction.
In conclusion, the IRGPI developed in this paper can be used to accurately evaluate the immune infiltration of patients and detect the prognosis of LUAD. It is a very robust biomarker of immunerelated prognosis. IRGPI grouping can help distinguish the immune and molecular characteristics and provide direction for clinical prediction of patient prognosis and tumor immunotherapy.
Acknowledgment
Thanks to the lab teachers for the writing guidance and proof reading
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of authors.
Funding
This work is supported by the Scientific and Technological Program of Guangzhou, Grant no. 201904010009; Doctoral workstation foundation of Guangdong Second Provincial General hospital, Grant no.2021BSGZ009; the National Nature Science Foundation of China, Grant Number: 81871211, 81502507; the Scientific and Technological Program of Guangzhou, Grant no. 202108050520130002.
References
- Goldstraw P, Kaeri C, John C, RR Prota, Hisao A, et al. (2016) The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming eighth edition of the TNM classification for lung cancer. J Thorac Oncol 11(1): 39-51.
- Ghimessy A, Radeczky P, Laszlo V, Hegedus B, Renyi Vamos F (2020) Current therapy of KRAS mutant lung cancer. Cancer Metastasis Rev 39(4): 1159-1177.
- Bradley JD, Paulus R, Komaki R, Masters G, Blumenschein G, et al. (2015) Standard dose versus high dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non small cell lung cancer RTOG 0617 a randomised two by two factorial phase 3 study. Lancet Oncol 16(2): 187-199.
- Ruiz Cordero R, Devine WP (2020) Targeted Therapy and Checkpoint Immunotherapy in Lung Cancer. Surg Pathol Clin 13(1): 17-33.
- N Bannister, J Broggio (2021) Cancer survival by stage at diagnosis for england.
- Miller VA, Hirsh V, Cadranel J, Chen Y, Park K, et al. (2012) A fatinib versus placebo for patients with advanced metastatic non small cell lung cancer after failure of erlotinib gefitinib or both and one or two lines of chemotherapy LUX Lung 1 a phase 2b/3 randomised trial. Lancet Oncol 13(5): 528-538.
- Lawrence RE, Salgia R (2010) MET molecular mechanisms and therapies in lung cancer. Cell Adh Migr 4(1): 146-152.
- Hanahan D, Weinberg RA (2011) Hallmarks of cancer the next generation. Cell 144(5): 646-674.
- Isomoto K, Haratani K, Hayashi H, Shimizu S, Tomida S, Niwa T, et al. (2020) Impact of EGFR TKI Treatment on the Tumor Immune Microenvironment in EGFR Mutation Positive Non Small Cell Lung Cancer. Clin Cancer Res 26(8): 2037-2046.
- Öjlert ÅK, Halvorsen AR, Nebdal D, Lund Iversen M, Solberg S, et al. (2019) The immune microenvironment in non small cell lung cancer is predictive of prognosis after surgery. Mol Oncol 13(5): 1166-1179.
- Wang SS, Liu W, Ly D, Xu H, Qu L, et al. (2019) Tumor infiltrating B cells their role and application in anti tumor immunity in lung cancer. Cell Mol Immunol 16(1): 6-18.
- Ge P, Wang W, Li L, Zhang G, Gao Z, et al. (2019) Profiles of immune cell infiltration and immune related genes in the tumor microenvironment of colorectal cancer. Biomed Pharmacother, pp. 118
- Gajewski TF, Schreiber H, Fu YX (2013) Innate and adaptive immune cells in the tumor microenvironment. Nat Immunol 14(10): 1014-1022.
- Jiang P, Gu S, Pan D, Jingxin Fu, Avinash Sahu, et al. (2018) Signatures of T cell dysfunction and exclusion predict cancer immunotherapy response. Nat Med 24(10): 1550-1558.
- Qiang W, Dai Y, Sun G, Xing X, Sun X (2020) Development of a prognostic index of colon adenocarcinoma based on immunogenomic landscape analysis. Ann Transl Med. 8(6): 284.
- Jiang P, Gu S, Pan D, Fu J, Sahu A, et al. (2018) Signatures of T cell dysfunction and exclusion predict cancer immunotherapy response. Nat Med 24(10): 1550-1558.
- Sun S, Guo W, Wang Z, Wang X, Zhang G, et al. (2020) Development and validation of an immune related prognostic signature in lung adenocarcinoma. Cancer Med 9(16): 5960-5975.
- Qu Y, Cheng B, Shao N, Jia Y, Song Q, et al. (2020) Prognostic value of immune related genes in the tumor microenvironment of lung adenocarcinoma and lung squamous cell carcinoma. Aging Albany NY 12(6): 4757-4777.
- Wang Z, Jensen MA, Zenklusen JC (2016) A practical guide to The Cancer Genome Atlas TCGA. Methods Mol Biol 1418: 111-114.
- Jensen MA, Ferretti V, Grossman RL, Louis M Staudt (2017) The NCI Genomic Data Commons as an engine for precision medicine. Blood 130(4): 453-459.
- Bhattacharya S, Andorf S, Gomes L, Patrick Dunn, Henry Schaefer, et al. (2014) ImmPort: disseminating data to the public for the future of immunology. Immunol Res 58(2-3): 234-239
- Ritchie ME, Phipson B, Wu D, Yifang Hu, Charity W Law, et al. (2015) Limma powers differential expression analyses for RNA sequencing and microarray studies. Nucleic Acids Res 43(7): 47.
- Gu Z, Eils R, Schlesner M (2016) Complex heatmaps reveal patterns and correlations in multidimensional genomic data. Bioinformatics 32(18): 2847-2849.
- Ito K, Murphy D (2013) Application of ggplot 2 to pharmacometric graphics. CPT Pharmacometrics Syst Pharmacol 2(10): 79.
- Qiang W, Dai Y, Sun G, Xing X, Sun X (2020) Development of a prognostic index of colon adenocarcinoma based on immunogenomic landscape analysis. Ann Transl Med 8(6): 284.
- Zhang Z, Reinikainen J, Adeleke KA, Marcel E Pieterse, Catharina GM GroothuisOudshoorn (2018) Time varying covariates and coefficients in Cox regression models. Ann Transl Med 6(7): 121.
- Rizvi AA, Karaesmen E, Morgan M, Leah Preus, Junke Wang, et al. (2019) gwasurvivr an R package for genome wide survival analysis. Bioinformatics 35: 1968-1970.
- Chen Y, Li ZY, Zhou GQ, Sun Y (2021) An Immune Related Gene Prognostic Index for Head and Neck Squamous Cell Carcinoma. Clin Cancer Res 27(1): 330-341.
- Lin K, Huang J, Luo H, Luo C, Zhu X, et al. (2020) Development of a prognostic index and screening of potential biomarkers based on immunogenomic landscape analysis of colorectal cancer. Aging (Albany NY) 12(7): 5832-5857.
- TM Therneau (2015) A package for survival analysis in S. Version 2.38. CRAN.
- Ji Q, Cai Y, Shrestha SM, Shen D, Zhao W, et al. (2021) Construction and Validation of an Immune Related Gene Prognostic Index for Esophageal Squamous Cell Carcinoma. Biomed Res Int 2021: 7430315.
- Wang X, Su W, Tang D, Jing J, Xiong J, et al. (2021) An Immune Related Gene Prognostic Index for Triple Negative Breast Cancer Integrates Multiple Aspects of Tumor Immune Microenvironment. Cancers (Basel) 13(21): 5342.
- Lee YT, Tan YJ, Oon CE (2018) Molecular targeted therapy: Treating cancer with specificity. Eur J Pharmacol 834: 188-196.
- Gotwals P, Cameron S, Cipolletta D, Cremasco V, Crystal A, et al. (2017) Prospects for combining targeted and conventional cancer therapy with immunotherapy. Nat Rev Cancer 17(5): 286-301.
- Van den Bulk J, Verdegaal EM, de Miranda NF (2018) Cancer immunotherapy: broadening the scope of targetable tumours. Open Biol 8(6): 180037.
- Yang Y (2015) Cancer immunotherapy harnessing the immune system to battle cancer. J Clin Invest 125(9): 3335-3337.
- Morrison AH, Byrne KT, Vonderheide RH (2018) Immunotherapy and Prevention of Pancreatic Cancer. Trends Cancer 4(6): 418- 428.
- Lin X, Li Y, Wang J, Han F, Lu S, et al. (2017) LHX3 is an early stage and radiosensitivity prognostic biomarker in lung adenocarcinoma. Oncol Rep 38(3):1482-1490.
- B Ling, X Liao, Y Huang, L Liang, Y Jiang, et al. (2020) Identification of prognostic markers of lung cancer through bioinformatics analysis and in vitro International Journal of Oncology 56(1): 193-205.
- Mao Y, Xue P, Li L, Xu P, Cai Y, et al. (2019) Bioinformatics analysis of mRNA and miRNA microarray to identify the key miRNA gene pairs in small cell lung cancer. Mol Med Rep 20(3): 2199-2208.
- Chen R, Li WX, Sun Y, Duan Y, Li Q, et al. (2017) Comprehensive Analysis of lncRNA and mRNA Expression Profiles in Lung Cancer. Clin Lab 63(2): 313-320.
- Lei X, Lei Y, Li JK, Du WX, Li RG, et al. (2019) Immune cells within the tumor microenvironment: Biological functions and roles in cancer immunotherapy. Cancer Lett 470: 126-133.
- Hinshaw DC, Shevde LA (2019) The Tumor Microenvironment Innately Modulates Cancer Progression. Cancer Res 9(18): 4557 -4566.
- Thakkar S, Sharma D, Kalia K, Tekade RK (2020) Tumor microenvironment targeted nanotherapeutics for cancer therapy and diagnosis: A review. Acta Biomater 101: 43-68.
- Wang JJ, Lei KF, Han F (2018) Tumor microenvironment recent advances in various cancer treatments. Eur Rev Med Pharmacol Sci 22(12): 3855-3864.
- Tian Z, Meng L, Long X, Diao T, Hu M, et al. (2020) Identification and validation of an immune related gene based prognostic index for bladder cancer. Am J Transl Res 12(9): 5188-5204.
- Huang RZ, Mao M, Zheng J, Liang HQ, Liu FL, et al. (2021) Development of an immune related gene pairs index for the prognosis analysis of metastatic melanoma. Sci Rep 11(1): 1253.
- Zhong R, Chen D, Cao S, Li J, Han B, et al. (2021) Immune cell infiltration features and related marker genes in lung cancer based on single cell RNA seq. Clin Transl Oncol 23(2): 405-417.
- Hendry S, Salgado R, Gevaert T, Prudence A Russell, Tom John, et al. (2017) Assessing Tumor Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv Anat Pathol 24(6): 311-335.
- Jiang P, Gu S, Pan D, Fu J, Sahu A, et al. (2018) Signatures of T cell dysfunction and exclusion predict cancer immunotherapy response. Nat Med 24(10): 1550-1558.
