 Research Article
Research ArticleABSTRACT
Elevated hemidiaphragm image in chest X-ray study is usually linked to thoracic problems including eventration, phrenic nerve paralysis and parenchymal lung volume loss. Nevertheless, some upper abdominal abnormalities could lead to this phenomenon, which should be cautiously considered. In this article, we report a pyogenic liver abscess case due to rare complications of chronic gallbladder diseases.
Keywords: Liver Abscess; Gallbladder Stone; Elevated Hemidiaphragm
Abbreviations: RUQ: Right Upper Quadrant; CT: Computed Tomography; DM: Diabetes Mellitus
Introduction
Elevated hemidiaphragm image in chest X-ray study is usually linked to thoracic problems including eventration, phrenic nerve paralysis and parenchymal lung volume loss [1]. Nevertheless, some upper abdominal abnormalities could lead to this phenomenon, which should be cautiously considered. In this article, we report a pyogenic liver abscess case due to rare complications of chronic gallbladder diseases.
Case Report
A 71-year-old man with a history of diabetes mellitus was admitted to the hospital complaining of right upper quadrant (RUQ) pain, fever and hiccups after meals lasting for one week. According to his description, there was no decreased appetite, nausea, vomiting, bowel habit change, dysuria, cough, chest pain or other respiratory symptoms. On admission, he was febrile with a temperature of 38.2°C and otherwise unremarkable vital signs. Abdominal physical examinations revealed RUQ tenderness without rebound tenderness. Laboratory studies demonstrated neutrophilic leukocytosis, an elevated high-sensitivity C-Reactive protein (hsCRP) and normal liver function test except a slightly increased γ-glutamyl transferase (γ-GT). Blood parameters included a white blood cell count of 20.0×109/L (a normal range of 3.6-11.2), a neutrophilic segment of 82.9%, hsCRP of 19.37 mg/dL (a normal range of <1.0), a total bilirubin of 0.55 mg/dL (a normal range of 0.2-1.3), alanine aminotransferase (ALT) of 40 IU/L (a normal range of 5-40), γ-GT of 80 IU/L (a normal range of 8-50), and alkaline phosphatase of 106 IU/L (a normal range of 38-126).
Chest X-Ray showed elevation of right hemidiaphragm (Figure 1). Sonography of the abdomen revealed a hypoechoic lesion in the right lobe of liver, and liver abscess was suspected. Urgent computed tomography (CT) of abdomen was then arranged to show one lobulated lesion (5.0×3.5 cm in size) with hypodensity and ring enhancement in right lobe of the liver, consistent with liver abscess (Figure 2). Furthermore, one gallbladder stone (2.5×1.5 cm in size) accompanied with gallbladder wall thickening and gallbladder fistula with the liver abscess were noticed. Therefore, antibiotic treatment with Ceftriaxone was administered. Percutaneous drainage of the abscess was performed on the next day (Figure 3), and brick red material was aspirated for pus culture (Figure 4). Consequently, culture result was positive for Escherichia coli. After antibiotic treatment and abscess drainage, the patient had no further symptoms and was discharged with antibiotics and cholecystectomy was advised at two weeks later.

Figure 1: Chest X-Ray of elevation of right hemidiaphragm.

Figure 2: Computed tomography shows one lobulated lesion with hypodensity and ring enhancement in right lobe of the liver, which is compatible with liver abscess.
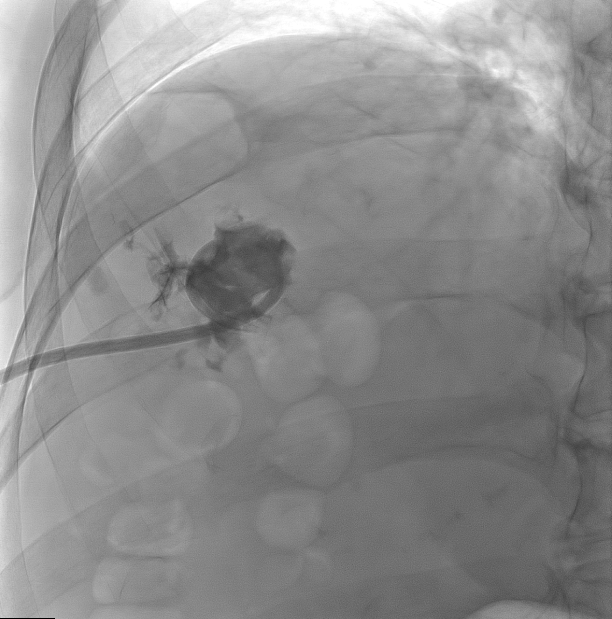
Figure 3: Percutaneous drainage of the liver abscess.

Figure 4: Aspirated brick red material from the liver abscess.
Discussion
Development of an intrahepatic abscess on account of gallbladder perforation is a rare situation as reported [2,3]. Some predisposing factors may lead to the perforation including diabetes mellitus (DM), cholelithiasis, trauma or malignancy history, male gender and the elderly [3]. Moreover, DM played an important role in pyogenic liver abscess comorbidities along with malignant neoplasms [4]. Therefore, the senior man with DM history in our report suffered a higher risk of both gallbladder perforation and liver abscess. Clinical presentations of biliary origin liver abscess are not highly specific and sensitive. Common symptoms include higher body temperature, chilling, RUQ pain, weak and jaundice [2,4]. Chest X-ray usually serves as the primary image examination to screen an emergent febrile patient and abnormal findings, inclusive of elevation of right hemidiaphragm, right basilar lung atelectasis and pleural effusion, suggest the presence of liver abscess [1,5]. Sequentially, abdominal ultrasound is recognized as the first-line choice for identifying cholecystitis; however, CT is a more sensitive method to diagnose a perforation or visualize the hole sign between liver abscess and gallbladder, as compared with ultrasound [2,3].
Regarding the most common pathogen for liver abscess, Klebsiella pneumoniae should be the answer in most countries in Eastern Asia. However, the major pathogen resulting in liver abscess of biliary origin in a recent study performed in Eastern Asia was Escherichia coli, which is consistent with the culture finding in our case [4]. Moreover, the treatment suggestions included intravenous antibiotics and percutaneous drainage [2,3,5]. Cholecystectomy is usually advised to prevent the recurrence of cholecystitis [2].
Funding
none to disclose.
Author Disclosures
The authors declare no conflicts of interest.
References
- Abbey-Mensah GN, Waite S, Reede D, Hassani C, Legasto A (2017) Diaphragm Appearance: A Clue to the Diagnosis of Pulmonary and Extrapulmonary Pathology. Curr Probl Diagn Radiol 46(1): 47-62.
- Hussain T, Adams M, Ahmed M, Arshad N, Solkar M (2016) Intrahepatic perforation of the gallbladder causing liver abscesses: case studies and literature review of a rare complication. Ann R Coll Surg Engl 98(6): e88-91.
- Kochar K, Vallance K, Mathew G, Jadhav V (2008) Intrahepatic perforation of the gall bladder presenting as liver abscess: case report, review of literature and Niemeier's classification. Eur J Gastroenterol Hepatol 20(3): 240-244.
- Shi S, Xia W, Guo H, Kong H, Zheng S (2016) Unique characteristics of pyogenic liver abscesses of biliary origin. Surgery 159(5): 1316-1324.
- Cooper BL, Lo BW, Dendy SE (2016) Man with fever and elevated hemidiaphragm. J Emerg Med 51(3): e57-e58.
