 Review Article
Review ArticleAbstract
Low back pain or pain in the sacral region are the main complaints in the modern world, where people are increasingly sedentary and seated. Various invasive or noninvasive treatments are used with these patients. Nowadays, a treatment that has been much sought after is chiropractic instrumental manipulation. Objective: To evaluate the results of treatment with the instrumental manipulation chiropractic for lower back pain. Methods: Three databases searched: PubMed, Embase, and BVS/LILACS with the search terms “Chiropractic Manipulation”, “Instrumental Chiropractic Technique”, “Low back pain”, “Chiropractic” in English, Portuguese and Spanish, from October 2021 to November 2021. Results: Two hundred and two published articles were found, and four randomized studies were selected for this systematic review with 204 patients. Conclusion: There is high-quality evidence that instrumental chiropractic therapy reduces pain and improves the function of patients with pain in the low back spine without adverse effects.
Keywords: Instrumental Chiropractic Technique; Chiropractic Manipulation; Low Back Pain; Chiropractic
Introduction
Low back pain (LBP) is defined in the literature as pain located below the ribs that goes to the inferior gluteal folds [1]. LBP is pragmatically classified as non-specific or specific. Nonspecific LBP is defined as low back pain when there is no clear relationship between symptoms, physical findings and imaging findings [2], and represents 90-95% of low back pain cases [3]. The estimated point prevalence of nonspecific LBP is 18% [4], affects people of all ages and is a major contributor to the burden of disease worldwide [5]. As nonspecific LBP has no known pathoanatomical cause, treatment focuses on pain reduction and its consequences [6]. Pain management approaches vary widely [7]. Non-steroidal anti-inflammatory drugs, opioids and neurotropic drugs or steroid injections and surgery are the main tools used in treatment [8]. Another approach method for the treatment of non-specific low back pain is chiropractic instrumental manipulation therapy [9]. This technique is a chiropractic method that uses an instrument to replace the therapist’s hand, being the second most used technique in the world, which provides the same results and benefits as the manual method, with the advantage of being more comfortable and safer for the patient [10]. Chiropractic instrumental manipulation is used by chiropractors for the treatment of acute pain in the lumbar and sacral region [11].
The literature has a limited amount of information about the role of chiropractic in treating LBP. Appropriate and carefully performed manual manipulation of the spine has been used to care for many of these patients [12]. However, depending on the nature and extent of the patient’s pain, the high velocity, low amplitude (HVLA) force of manual manipulation, may present an undesired risk of aggravation or be completely inappropriate [13]. Chiropractic Instrumental Adjustment may offer an adequate and effective therapeutic approach in certain types of these cases due to the low strength and site-specific nature of the manipulative impulses that can be delivered to the spine with a manual adjustment instrument [14]. This instrument allows chiropractors to provide a quick, low strength thrust at specific points [15]. This systematic review aims to assess the result of the instrumental manipulation chiropractic therapy in LBP.
Methodology
Search Strategy
(((Chiropractic[mh] OR Chiropractic[tiab]) AND (Back Pain[mh] OR Low Back Pain[mh] OR Back Pain*[tiab] OR Backache*[tiab] OR Low Back Pain*[tiab] OR Lower Back Pain*[tiab])) AND (Effectiveness[tiab] OR Efficiency[tiab] OR Treatment Outcome[mh] OR Treatment Outcome[tiab] OR Efficacy[tiab] OR Effect*[tiab] OR Assessment[tiab] OR Evaluation[tiab])) AND (English [lang] OR Portuguese [lang] OR Spanish [lang]) AND (“2016/01/01”[PDAT]: “2021/04/20”[PDAT]
Eligibility Criteria
The studies included in this review must:
(i) Use instrumental manipulation chiropractic therapy,
(ii) Written in English, Spanish, and Portuguese, and
(iii) That speak of the Low back pain. Excluded articles that
were duplicates, comments, letters, abstracts of congresses, books,
book chapters, systematic reviews, and meta-analyses or narrative
reviews and that do not use instrumental for manipulation. Also
besides, articles that do not address pain in the low back spine.
Methodological Quality
The methodological quality of the articles assessed using the PEDro scale (Physiotherapy Evidence Database) which tests the effectiveness of therapy interventions. On this scale, there are 10 criteria established based on an “expert consensus” and not on empirical data. The score awarded only when a criterion is satisfied. Publications with a score of seven or more on the PEDro scale considered to be of ‘high’ methodological quality, those with a score of five to six would be of ‘regular’ quality, and a score of four or less classified as “poor” quality [16].
Risk of Bias
The risk of bias was assessed in the studies selected according to the Cochrane risk of the bias assessment tool [17]. According to the instrument, for each work, different domains related to the risk of bias were assessed independently.
Case Report (CARE)
The CAse REport (CARE) guidelines checklist is structured to correspond with key components of a case report and capture useful clinical information. This 13-item checklist provides a framework to satisfy the need for completeness and transparency for published case reports [18].
Results
A total of 202 studies were identified through a database search and, after the removal of duplicates, 99 studies were identified. During the screening process, 189 publications were excluded for not being related to the research question and the full text of nine studies was reviewed in detail. Finally, four randomized control studies were included in the systematic review. The selection process is schematized in (Figure 1). The included studies had a mean score of six when assessing the methodological quality with the PEDro scale (Figure 2), with a minimum of 5 points and a maximum of seven, evidencing moderate methodological quality. Detailed description and results of the included studies are presented in Table 1. All studies [19-21] were designed as randomized controlled trials. The risk of bias of included studies was assessed with the Cochrane risk of bias tool (Figure 3). To analyze the case study article, we used The CAse REport (CARE) guidelines checklist (Figure 4).
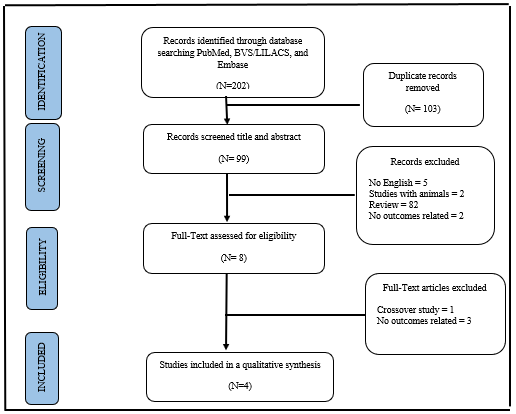
Figure 1: PRISMA flowchart with the different stages of the current systematic review.
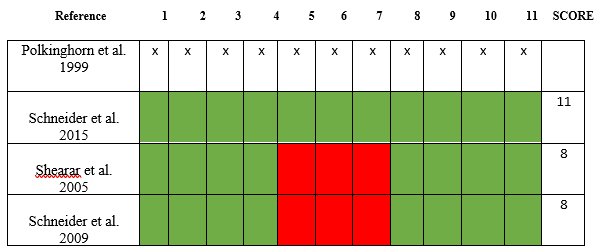
Figure 2:
(1) Methodological quality assessment of the included studies with PEDro scale.
(2) Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which
treatments were received);
(3) Allocation was concealed;
(4) The groups were similar at baseline regarding the most important prognostic indicators;
(5) There was blinding of all subjects;
(6) There was blinding of all therapists who administered the therapy;
(7) There was blinding of all assessors who measured at least one key outcome;
(8) Measures of at least one key outcome were obtained from more than 85%; of the subjects initially allocated to groups;
(9) All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where
this was not the case, data for at least one key outcome was analyzed by “intention to treat”;
(10) The results of between-group statistical comparisons are reported for at least one key outcome;
(11) The study provides both point measures and measures of variability for at least one key outcome. The Polkinghorn et al.
1999 as a case study, it does not fit this criterion.
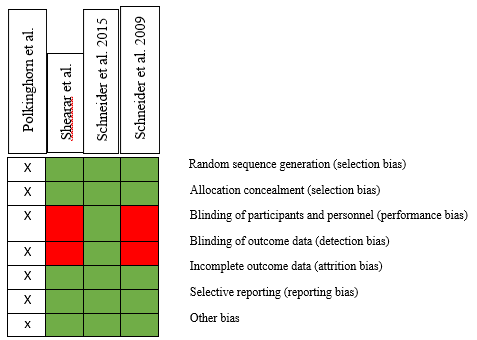
Figure 3: Risk of bias summary: authors assessment for each risk of bias criterion. The Polkinghorn et al. 1999 as a case study, it does not fit this criterion.

Figure 4: Case Report (CARE) guidelines.
Discussion
The aim of this review was to analyze the results of the treatment of patients with pain in the lower region of the spine (lumbar, sacroiliac and coccyx) using chiropractic instrumental manipulation technique. For this, we selected a case study [21], a cohort study, a randomized trial and a randomized clinical trial [21]. The Polkinghorn et al. because it is a case study, it was not evaluated using the PEDro methodological quality scales and the Cochrane risk of bias tool. The other three articles were evaluated and their methodological quality by the PEDro scale obtained a score of 8 and 15 for Schneider et al. 2015. Due to the risk of bias, Schneider et al. Obtained the low-risk result, and the other 2 articles obtained a medium risk of bias with a score of 7. In CAse REport (CARE) guidelines, Polkinghorn et al. got a good evaluation with a score of 12. Although there are several articles [22-24] in the literature that present studies on this technique, there is still a need for more research on this method. In this review, we were able to assess that in terms of clinical efficacy, chiropractic instrumental manipulation found statistically positive results for pain, although the differences between the protocol and the application of the technique were not the same in the four studies addressed. In summary, the articles that investigated the use of the instrument in manipulation only reported that it brought clinically significant benefits to patients. The results of this study may provide useful information for clinicians and patients in terms of therapeutic efficacy for treating patients with back pain without the risk of manipulation of the lumbar spine, sacro-coccygeal.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Competing Interests
The authors declare that they have no competing interests in this section.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Contribution
• Melo-Oliveira, MES: Conceptualization, Original Writing-draft;
project management
• Baumgarth, Henrique: Software and visualization; Formal
analysis; Research
• Tosi, ML: Methodology; writing-proofreading and editing.
• Edgar Idogava: Supervision
Acknowledgment
Not applicable.
Limitation
Study limitations include a small sample size, lack of a control group, and in addition, health care records may not contain all relevant data.
References
- Van Tulder M, Becker A, Bekkering T, Alan Breen, Maria Teresa Gil del Real, et al. (2006) Care CBWGoGftMoALBPiP: Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J 15(Suppl 2): S169-S191.
- Franke H, Franke JD, Fryer G (2014) Osteopathic manipulative treatment for nonspecific low back pain: a systematic review and meta-analysis. BMC Musculoskelet Disord 30: 15: 286.
- Hoy D, Bain C, Williams G, March L, Brooks P, et al. (2012) A systematic review of the global prevalence of low back pain. Arthritis Rheum 64(6): 2028-2037.
- Dagenais S, Caro J, Haldeman S (2008) A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J 8(1): 8-20.
- Maher C, Underwood M, Buchbinder R (2017) Non-specific low back pain. Lancet 18 389(10070): 736-747.
- Coulter ID, Crawford C, Hurwitz EL, Vernon H, Khorsan R, et al. (2018) Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. Spine J 18 (5): 866-879.
- Schneider MJ, Brach J, Irrgang JJ, Katherine Verdolini Abbott, Stephen R Wisniewski, et al. (2010) Mechanical vs. manual manipulation for low back pain: an observational cohort study. J Manipulative Physiol Ther 33(3): 193-200.
- Salzberg LD, Manusov EG (2013) Management options for patients with chronic back pain without an etiology. Health Serv Insights 6: 33-38.
- Fuhr AW, Menke JM (2005) Status of activator methods chiropractic technique, theory, and practice. J Manipulative Physiol Ther 28(2): e1-e20.
- Soulier F (2009) D’Equilibration Neuro Musculaire; niveau I; [online journal].
- Huggins T, Boras AL, Gleberzon BJ, Mara Popescu, Lianna A Bahry, et al. (2012) Clinical effectiveness of the Activator adjusting instrument in the management of musculoskeletal disorders: a systematic review of the literature. J Can Chiropr Assoc 56(1): 49-57.
- Côté P, Hartvigsen J, Axén I, Charlotte Leboeuf-Yde, Charlotte Leboeuf-Yde, et al. (2021) The global summit on the efficacy and effectiveness of spinal manipulative therapy for the prevention and treatment of non-musculoskeletal disorders: a systematic review of the literature. Chiropr Man Therap 29(1): 8.
- Wood TG, Colloca CJ, Matthews R (2001) A pilot randomized clinical trial on the relative effect of instrumental (MFMA) versus manual (HVLA) manipulation in the treatment of cervical spine dysfunction. J Manipulative Physiol Ther 24(4): 260-271.
- Langenfeld A, Humphreys BK, De Bie RA (2015) Effect of manual versus mechanically assisted manipulations of the thoracic spine in neck pain patients: study protocol of a randomized controlled trial 16: 233.
- Colloca CJ, Keller TS, Black P, Martin C Normand, Deed E Harrison, et al. (2005) Comparison of mechanical force of manually assisted chiropractic adjusting instruments. J Manipulative Physiol Ther 28(6): 414-422.
- Shiwa R, Pena CLO, Menezes LC, Anne Moseley, Luiz Carlos Hespanhol Junior, et al. (2011) Reproducibility of the Portuguese version of the PEDro Scale. Cad. Saúde Pública 27(10): 2063-2067.
- Sterne JA, Hernán MA, Reeves BC, Jelena Savović, Nancy D Berkman, et al. (2016) ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ 355: i4919.
- Gagnier JJ, Kienle G, Altman DG, David Moher, Harold Sox, et al. (2014) CARE Group. The CARE guidelines: consensus-based clinical case report guideline development. J Clin Epidemiol 67(1): 46-51.
- Schneider M, Haas M, Glick R, Joel Stevans, Doug Landsittel, et al. (2015) Comparison of spinal manipulation methods and usual medical care for acute and sub-acute low back pain: a randomized clinical trial. Spine (Phila Pa 1976) 40(4): 209-217.
- Polkinghorn BS, Colloca CJ (1999) Chiropractic treatment of coccygodynia via instrumental adjusting procedures using activator methods chiropractic technique. J Manipulative Physiol Ther 22(6): 411-416.
- Shearar KA, Colloca CJ, White HL (2005) A randomized clinical trial of manual versus mechanical force manipulation in the treatment of sacroiliac joint syndrome. J Manipulative Physiol Ther 28(7): 493-501.
- Keller TS, Colloca CJ, Moore RJ (2006) Increased multiaxial lumbar motion responses during multiple-impulse mechanical force manually assisted spinal manipulation. Chiropr Osteopat 14: 6.
- Colloca CJ, Keller TS, Gunzburg R (2004) Biomechanical and neurophysiological responses to spinal manipulation in patients with lumbar radiculopathy. J Manipulative Physiol Ther 27(1): 1-15.
- Apfelbeck L (2005) An integrative treatment approach of a patient with cervical radiculitis: A case report. J Chiropr Med Spring 4(2): 97-102.
