 Research Article
Research ArticleAbstract
Background: Orthopaedic surgeons encounter various types of joint dislocation in their daily practices. The shoulder is the most common joint to dislocate. There are multiple options in management of shoulder dislocation. However, there is a lot of controversy as to which method of stabilization. There are those surgeons that believe in bony stabilization and those that prefer soft tissue anatomical stabilization. A retrospective cohort review study was undertaken to determine the outcomes in patient that had soft tissue stabilization as a primary procedure.
Method: We reviewed our shoulder instabilities that had a Bankart lesion repair and had anatomical Bankart reconstruction. We had 52 shoulder dislocations that had soft tissue shoulder stabilization. We reviewed the files for pre- and post-operative function, number of dislocations pre operatively and redislocation rate post anterior soft tissue stabilization. The OSIS was used for telephonically assessment of all the patients.
Results: The redislocation rate was 19%. They were no statistical difference between those who are actively involved in sport. Five patients had confirmed dislocation and of those, two went on to have a Laterjet procedure performed. There were no reported infection or nerve injuries associated with arthroscopic surgery. Post op the patient was able to go back to previous level of activities. The OSIS was slightly elevated for the patients that had redislocation.
Conclusion: Soft tissue stabilization can be used as primary stabilization operation for first time dislocations.
Keywords: Arthroscopic Soft Tissue Stabilization; Primary Procedures; Shoulder Instability
Introduction
The shoulder is the joint in which most joint dislocation are encountered, with an incidence of 2 % in the general population. Anterior shoulder dislocation is the most frequent type and accounts for 90 to 98% [1,2] while posterior dislocation accounts for about 2% [3]. The main instabilities are Bankart lesion (avulsion of the anterior glenoid labrum from bone), glenoid edge fracture, Hill-Sachs lesion (osseous defect due to dislocation of the poster superior lateral humeral head) and loose body. The Perthes lesion (a labroligamantous avulsion in which the scapular periosteum remains intact) and ALPSA lesion (a medial displacement of the anterior labral ligamentous complex with an intact scapular periosteum), should be considered potential causes of shoulder intability [4,5].
In first time dislocation, 50 to 80 % of resultant Bankart lesions heal after a period of immobilisation with a variable duration between 3 to 6 weeks [6]. The recurrence rate is 17 to 96 % in conservative management of young athlete [5,6]. Treatment options for traumatic shoulder dislocation may vary from conservative or operative. Clinical and biomechanical studies have demonstrated that traumatic dislocations and subluxations result in labral detachment and capsular elongation. Open shoulder stabilization has a proven record as a standard treatment for shoulder dislocation [4,6]. Older studies have shown that arthroscopic shoulder stabilization is associated with increased risks for redislocation 10%-30% [7,8]. The purpose of this study was to evaluate the redislocation rate in our patients and also look at other involved risk factors.
Method
We retrospectively reviewed the cases that were done by our units, between the period from 2010-2020. We reviewed the patient’s files in terms of indications for theatre and post-op redislocation. The oxford shoulder instability score was assessed telephonically. The inclusion criteria included all the patients that had arthroscopic stabilization during the study period. We included patients that were having arthroscopic stabilization as a primary procedure, with a minimum of six months follow up, as this was the average rehabilitation period before return to full sporting activity, and we were able to contact for the OSIS scoring. We excluded all open shoulder stabilization, patient with previous shoulder stabilization on the same side, patients that needed stabilization plus rotator cuff surgery and multidirectional instability. We also excluded patients with large lesions involving the glenoid and /or humeral head, as was seen on either pre- operative radiography. Permission was obtained from the patient to be part of the study, and they were given the option to respond to the questionnaire if they agreed, and their charts were reviewed. Preoperatively all patients were physically examined, and joint hyperlaxity, sulcus sign, apprehension and jobs relocation test were done. The radiological investigation included plain radiography with anteroposterior, scapular lateral and axillary views and MRI was done for some of the patients.
Operative Procedure
Patient were all operated on by two surgeons in theatre, and they were either in beach chair position or lateral position depending on the surgeon’s preference. Standard portals were used, and after the posterior portal was placed a diagnostic scope was done. Two portals, anterior portal and the rotator interval, was used for the superior anterior portal. A tissue liberator was used to elevate the labrum and anterior capsule. A decision was then taken to use two or three suture anchors. The standard two suture anchors were usually used, with the first anchor places at five o clock position on the anterior glenolabrum and included inferior glenohumeral ligament advanced anteriorly with a capsular shift. The second anchor was at three o clock position. The third anchor was mostly used for large anterior Bankart injuries to increase stability or when they were an associated SLAP lesion.
Postoperatively an arm sling was used to immobilize the shoulder up to four weeks. After six weeks, active exercise under physiotherapy guidance was allowed, and external rotation allowed after nine weeks. The return to full sporting activities was allowed after six months. In our study, we had 49 male patients (94.2%) and three female patients (5.8%). Twenty-one were left-handed (40.4%), and 31 were right-handed (59.6 %). The mean age of our patient at first dislocation was 25.3, and the mean age when they had the operation was at 27.2 (Figure 1).
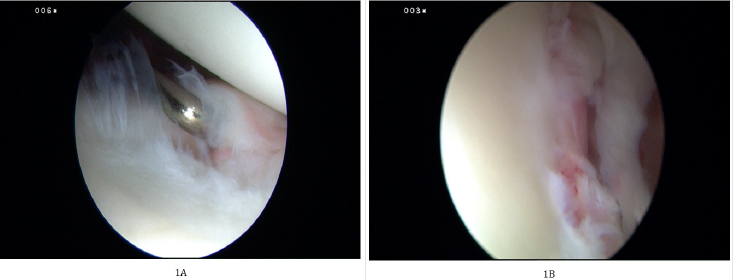
Figure 1:
A. Showing a Bankart lesion post traumatic shoulder dislocation,
B. Shows probe used to assess the integrity of the labrum before debridement and suture passing.
Statistical Methods
IBM SPSS version 26 was used to analyze the data. Frequency tables were used to summaries categorical data in counts and percentages. Continuous data were summarized using mean and standard deviation. Associations between re-operation and various factors were achieved using Fisher’s exact tests in the case of categorical factors, and t-tests for continuous factors. A p-value <0.05 was used to indicate statistical significance.
Anchor Used
The number of anchors used depended on the arthroscopic findings intra-op if the instability involved a Bankart lesion together with slap lesion we usually used three anchors. Isolated Bankart lesion that required repair and capsular shift, two anchors were usually used, at 5 o’clock and 2 or 3 o’clock position. Three anchors were sometimes used for large anterior Bankart lesion to improve stability.
Results
Demographics
There were 52 participants in the study, of which 94% were male. Their demographics are shown in the table below. We had 49 males and three females (Table 1). Being involved in sports was not a factor for re-operation, 17% of the rugby players vs 23 % of the non-rugby players had re-operation. 17.5% of the participants who played sports had re-operation while 25% of those who did not play sport had re-operation. The difference was not statistically significant, though (Table 2). There was a tendency to score higher on the OSIS scale in those with re-operation, but it was not statistically significant. Age was slightly higher in those with reoperation but also not significantly different (Table 3). There was no association between age and repair type (p=0.659) (Tables 4 & 5).
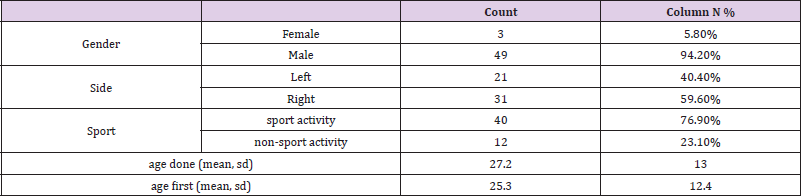
Table 1: Demographics.

Table 2: Dislocation rate.
Note: There was a 19% re-operation (dislocation) rate.
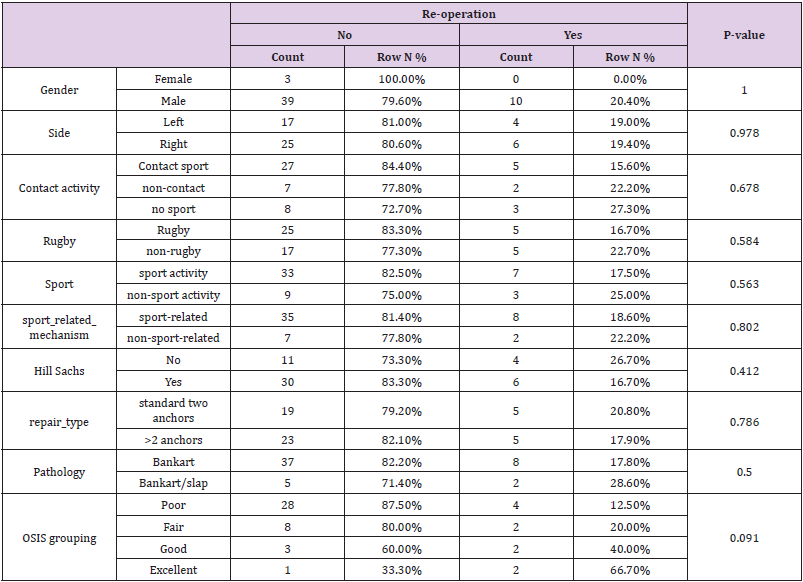
Table 3: Sporting activity and Factors associated with redislocation.
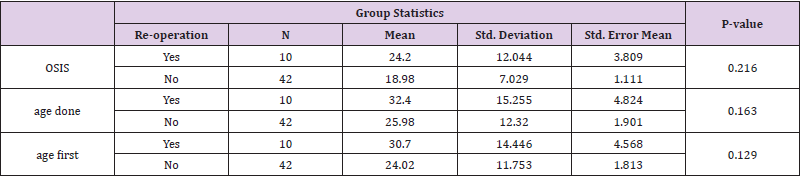
Table 4: Oxford shoulder instability score.

Table 5: Number of anchors used.
Discussion
Recurrent shoulder instability is a very debilitating condition, especially for active young patients. Arthroscopic shoulder stabilization results show variable results when compared to open repair, which has lower failure rates [8,9]. Saper, in his study, demonstrated good outcomes with arthroscopic stabilization, with a 90% stability restoration and 80% return to pre-injury levels [10]. The redislocation rate is used as one of the outcome measures post shoulder stabilizations. In our series, the redislocation rate was 19%, which compares with the most recent studies [10,11]. Most of our patients that reported having had a dislocation, only five reported a reduction by a physician. Two of the five patient went on further to a Laterjet operation. This leads us to believe that most of these cases were subjective subluxation reported as dislocation, but since it was difficult to distinguish the two, we reported them as dislocations. Looking at the number of anchors used, we found no association between the number of anchors and redislocation. Previous studies looking and the effect of the number of anchors and the rate of redislocation have conflicting results [12], however they are more evidence advocating using three anchors to improve stability. A recent paper by Ozdemir, comparing the use of two versus three anchors in Bankart lesion showed no different in outcomes in terms of the redislocation [13].
The interval between the first dislocation and the time of surgery did not seem to play a critical role in the failure of the stabilization. The mean time between the first episode and surgery was 20 weeks. We specifically looked at those involved in contact sport especially rugby players, and our results showed that the rugby players had reduced redislocation rate at 17% compared to the other contact group that had a redislocation rate of 23%. Studies looking specifically at recurrence in rugby players have shown that it could be high as 51% [14]. This could have been as a result of the younger age group in the rugby players compared to the rest of the group. A long-term follow-up, by Owens et al, showed that acute arthroscopic Bankart repair for first-time traumatic anterior dislocations resulted in good outcomes for young athletes [15]. Controversy remains regarding the optimal treatment for patients with high functional demands. Studies comparing arthroscopic stabilisation vs open Laterjet in athletes have shown better results with arthroscopic stabilisation in terms of return to sport and proprioception however there remain a higher redislocation rate with arthroscopic stabilisation [16]. A retrospective cohort study, by Blona at el, showed that the arthroscopic Bankart procedure was inferior to the open Latarjet procedure for repair of recurrent anterior shoulder dislocation [17]. The difference between the procedures with respect to the quality of outcomes significantly increased with follow-up time [18].
None of the patients in the study reported other complication as in infection, nerve injuries or other complications. The patients that had redislocation had a high OSIS score, but it was not statistically significant with a P-value of 0.2 16. The weaknesses to our study included that, the research study sample was small, with only 52 patients that fitted our inclusion criteria. We also had a short follow up with average follow up being at 4 yrs. Strongpoint, we had the same group of surgeons using the same standardized technique. We also used the same rehabilitation protocol irrespective if they were contact or non-contact sport person. Further studies looking at the redislocation rate in a similar cohort with longer follow-up duration are suggested [19,20].
Conclusion
Soft tissue stabilization can be recommended as a primary procedure for primary shoulder stabilization. The incidence of redislocation is comparable to that of bony procedures.
Conflict of Interest
No conflict of interest with any institution/organization.
References
- Canale ST, Beaty JH, Campbell WC (2012) Campbell's operative orthopaedics (12th)., St. Louis, Mo.; London: Mosby.
- Pavic R, Margetic P, Bensic M, Brnadic RL (2013) Diagnostic value of US, MR and MR arthrography in shoulder instability. Injury 44 (Suppl 3): S26-S32.
- Kraeutler MJ, Aberle NS, Brown CC, Ptasinski JJ, McCarty EC (2018) Clinical Outcomes and Return to Sport After Arthroscopic Anterior, Posterior, and Combined Shoulder Stabilization. Orthop J Sports Med 6(4): 2325967118763754.
- Ovesen J, Nielsen S (1985) Stability of the shoulder joint: cadever study of stabilizing structures. Octa Orthopaedica Scandinavica 56(2): 149-151.
- Neviaser TJ (1993) The anteriorlabroligamentous periosteal sleeve avulsion: a cause of anterior instability of the shoulder. Arthroscopy 9(1): 17-22.
- Boileau P, Villalba M, Hery JY, Balg F, Ahrens P, et al. (2006) Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am 88(8): 1755-1763.
- Patrick Vavken, Patrick Sadoghi, Julia Quidde, Robert Lucas, Ruth Delaney, et al. (2014) Immobilisation in internal or external rotation does not change recurrence rates after traumatic anterior shoulder dislocation. J Shoulder Elbow Surg 23(1): 13-19.
- Burkhart SS, De Beer JF (2000) Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy-the Journal of Arthroscopic and Related Surgery 16(7): 677-694.
- Raffaele Garofalo, Andrea Mocci, Biagio Moretti, Eugenio Callari, Giovanni Di Giacomo, et al. (2005) Arthroscopic treatment of anterior shoulder instability using knotless suture anchors. Arthroscopy-the Journal of Arthroscopic and Related Surgery 21(11): 1283-1289.
- TR Lenters, AK Franta, FM Wolf, SS Leopold, FA Matsen III (2007) Arthroscopic compared with open repairs for recurrent anterior shoulder instability: A systematic review and meta-analysis of the literature. J Bone Joint Surg Am 89: 244-254.
- Saper MG, Milchteim C, Zondervan RL, Andrews JR, Ostrander RV (2017) Outcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact Sports. Orthopaedic Journal of Sports Medicine.
- Hassanin Alkaduhimi, Just A van der Linde, Nienke W Willigenburg, Nuno Rui Paulino Pereira, Derek FP van Deurzen, et al. (2016) Redislocation risk after an arthroscopic Bankart procedure in collision athletes: a systematic review. Journal of Shoulder and Elbow Surgery 25(9): 1549-1558.
- Hideaki Shibata, Masafumi Gotoh, Yasuhiro Mitsui, Yoshihiro Kai, Hidehiro Nakamura, et al. (2014) Risk factors for shoulder re-dislocation after arthroscopic Bankart repair. J Orthop Surg Res 9: 53.
- Kramer J, Gajudo G, Pandya NK (2019) Risk of Recurrent Instability After Arthroscopic Stabilization for Shoulder Instability in Adolescent Patients. Orthop J Sports Med 7(9).
- Garofalo R, Mocci A, Moretti B, Callari E, Di Giacomo G, et al. (2005) Arthroscopic treatment of anterior shoulder instability using knotless suture anchors. Arthroscopy 21(11): 1283-1289.
- Ozdemir B, Akpinar S, Cinar BM (2021) A comparative study on the use of two versus three double-loaded suture anchors in arthroscopic Bankart repair. JT Dis relat Surg 32(1): 108-114.
- Torrance E, Clarke CJ, Monga P, Funk L, Walton MJ (2018) Recurrence After Arthroscopic Labral Repair for Traumatic Anterior Instability in Adolescent Rugby and Contact Athletes. The American Journal of Sports Medicine 46(12): 2969-2974.
- Blonna D, Bellato E, Caranzano F, Assom M, Rossi R, et al. (2016) Arthroscopic Bankart Repair Versus Open Bristow-Latarjet for Shoulder Instability: A Matched-Pair Multicenter Study Focused on Return to Sport. The American Journal of Sports Medicine 44(12): 3198-3205.
- Zimmermann Stefan, Scheyerer Max, Farshad Mazda, Sabrina Catanzaro, Stefan Rahm, et al. (2016) Long-Term Restoration of Anterior Shoulder Stability: A Retrospective Analysis of Arthroscopic Bankart Repair Versus Open Latarjet Procedure. J Bone Joint Surg Am 98(23): 1954-1961.
- Brett D Owens, Thomas M DeBerardino, Bradley J Nelson, John Thurman, Kenneth L Cameron, et al. (2009) Long-term Follow-up of Acute Arthroscopic Bankart Repair for Initial Anterior Shoulder Dislocations in Young Athletes. The American Journal of Sports Medicine 37(4): 669-673.
