 Research Article
Research ArticleABSTRACT
Background: Hemophilia is an inherited type of disease in which clotting factor
VIII cannot produce properly in the body. These diseases can lead to prolonged bleeding
after injury or surgery and sometimes bleeding in the joint.
Objective: The objective of this study was to determine the level of activity limitation
due to joint pain among hemophilia patients.
Material and Method: 152 hemophilia patients was selected for data collection.
Data for this research was gathered from hemophilia center in Lahore between
5-19 years of age. Data was collected using Standardized Questioner of Activilim by
Convenient sampling technique. Data was analyzed using IBM SPSS Statistics 25.
Results: Responses were collected from 152 patients with an age 5-19 years. Pain
was observed and affected daily activities and quality of life. Respondents reported
functional impairment that limited the kind of work and activities they participated
in, with activities involving the lower extremities being most affected. Running and
squaring were impossible to perform among few children. Facing difficulty in toilet,
taking bath, during shower and other physical activities.
Conclusion: Pain was observed and affected daily activities and quality of life.
Respondents reported functional impairment that limited the kind of work and activities
they participated in, with activities involving the lower extremities being most affected.
Keywords: Hemophilia; Joint Pain; Hemophilic Patients
Introduction
Hemophilia is an inherited type of disease in which clotting
factor VIII cannot produce properly in the body. These diseases can
lead to prolonged bleeding after injury or surgery and sometimes
bleeding in the joint [1]. The first time hemophilia was discovered in
the 2nd century AD and a full description of hemophilia was written
in the 19thcentury.The ant hemophilic factor was discovered in the
middle of 20 century [2]. Approximately 40,000 peoples are affected
by hemophilia worldwide and it is the most complicated disease
in the world [3]. Hemophilia is the type of X-linked group disease
in which blood coagulation factor VIII cannot produce. Based on
clotting factor hemophilia has two types. The deficiency of clotting
factor VIII is called hemophilia A and the deficiency of clotting
factor IX is also called hemophilia B [4]. Hemophilia A is the most
common genetic disorder about 80 % of people have hemophilia
A in the overall population of hemophilia diseases. The prevalence
of hemophilia A (HA) 1 per 5000 in the general population and the
prevalence of hemophilia B (HB) is 1 per 30,000 in overall general
papulation .Hemophilia is mainly present in the male population
.on based on coagulation factor activity hemophilia is also divided
into three further groups .Clotting activity less than 1 percent is
severe if 1-5 % is moderate and if clotting greater than 5-30 %. The
intensity of bleeding is depending on hemophilia severity. If the intensity of hemophilia is severe, the spontaneous bleeding occurs
in soft tissues, joints, nose, and other parts of the body, and if the
intensity of diseases is moderate or mild the prolonged bleeding
occurs after injury or surgery [5].
Bleeding in joints is more common in hemophilia patients
due to a lack of clotting factors. The bleeding in the joint produces
more complications in joint. Inflammatory reactions start due
to hem arthrosis. Hemophilic arthropathy starts due to repeated
episodes of bleeding in joints. The inflammation of the synovial
membrane in a joint can lead to a breakdown of articular cartilage
of the joint. The articular breakdown starts in early childhood
in hemophilic patients. Chronic pain starts in hemophilic joints
due to the breakdown of articular cartilage. Chronic hemophilic
arthropathy can various effects on bone health, it can cause chronic
pain in joints, swelling, limit the daily activities of life, decrease the
range of motion of joints and also decrease the quality of life in
hemophilic patients. The most common joints which are affected by
hemophilia are ankle, knee, hip, elbow, and shoulder joints. There
are usually weight-bearing joints that have a bad impact on physical
movements. The bleeding the joints cause hypertrophy of physics
which lead to valgus deformity in hemophilia patient [6].
Joint illness linked with recurrent joint bleeding causes
discomfort and functional impairment in people with hemophilia
(PWH) (hemarthroses). Discomfort is common in PWH, according
to many studies [7,8] and pain associated with hemophilia has
been linked to a worse health-related quality of life (HRQoL). PWH
also has mental health problems [9,10]. According to the EQ-5D-
3L, depression affects around one-third of PWH, and the Patient
Health Questionnaire (PHQ-9), a scale used to evaluate the severity
of depressive symptoms in adults, 37 percent of PWH fulfilled the
criteria for depression in another research [11]. The influence of
hemophilia on emotional well-being, like other elements of HRQoL,
is rarely studied in the therapeutic context. In the comprehensive
care environment or to individualize hemophilia therapy, neither
general nor disease-specific patient-reported outcome (PRO) tools
are routinely employed [12]. Greater expertise with and validation
of PRO instruments in PWH may expand their usage for clinical
outcome monitoring, as well as provide possibilities to improve
patient dialog and treatment of specific outcomes.
The repeated episode of bleeding in joints can start the
inflammatory reaction in joints. This inflammatory reaction starts
the breakdown process in joints. The breakdown has a serious
impact on bone and joint health it can lead to osteoporosis of
bone, articular cartilage damage, and bony osteophytes formation
in joints, decrease the range of motion of joints and also decrease
the daily activity of life. Hemophilia patients have a great risk of
depression. The main reason for depression in hemophilia patients
is a decrease in the activity of life [13]. Swelling, heat, and immobility
are all symptoms of joint bleeding. Furthermore, acute bleeding
produces significant discomfort in the affected joint, a symptom
that has received little attention in prior research. The bulk of
studies in this area focused on the management of pain in general
and the use of analgesics [14]. The hemophilia patient faced many
psychosocial problems. This problem related to their education
and jobs and is also a problem for the caregiver of children with
hemophilia and barrier for happy living the people with hemophilia
because they cannot perform the daily activity due to pain in joints
and difficulty to concentrate his work [15].
Recurrent bleeding, in addition to the acute discomfort,
triggers a persistent process that results in synovitis, increased
cartilage degradation, and bone deterioration, eventually leading to
hemophilic arthropathy. Despite the existence of numerous potential
pathophysiological ideas, the actual underlying processes for either
blood-induced arthropathy or, more specifically, joint bleedinginduced
pain are yet unknown. Similar to other inflammatory
joint diseases, the associated inflammatory response might be
addressed as one possible source of pain complaints [16,17]. All of
these mechanisms, on the other hand, contribute to hemophilia’s
reported joint discomfort. As a result, current research is focusing
on the causes and effects of persistent pain caused by hemophilic
arthropathy. Because pain therapy is often ineffective, and many
analgesic and anti-inflammatory medications are prohibited due
to their clotting-inhibitory effects, a deeper pathophysiology
understanding of pain in persons with hemophilia (PWH) is vitally
necessary [18]. Hemophilic patients faced many problems in our
society. They face social, mental, and physical problems. The reason
for study in hemophilia to find out the activity limitation due to pain
or hemarthrosis.
Literature Review
J Michael soucie (2015) et al. Conduct a cross-sectional study
in a hemophilic treatment center in the USA. The study sample size
was 4343 males aged 2-19 years with hemophilia diseases. They
collect the data to assess the joint range of motion. They concluded
that the range of motion limitation in hemophilia patients depends
on the severity of disease and damage of articular cartilage due to
bleeding in joints [19]. M. Witkop (2017) et al. Purpose a crosssectional
study to find the prevalence and joint pain due to bleeding
joint in people with hemophilia. Their study sample size was 381
whose age is middle to 37. They found that 71 % of people have
a severe type of hemophilia and pain in the joint more common
the people with hemophilia. In this study, they concluded that the
functional activity limitation and quality of life decrease in people
with hemophilia are due to chronic pain in the joint [7]. Tyler and W
Buckner (2018) conducted a study in which they find the prevalence of functional limitation or living quality in hemophilia patients. The
study sample size was 381 adult patients with hemophilia whose
age was medial to 34 old. They use the visual analogs scale and brief
pain inventory v2 short form to collect the data. They found that
patients present severe pain in joints and functional limitation and
also decrease the quality of life due to pain in joints. They concluded
that early asses of joints bleeding and proper history improve the
quality 0f life and activity of daily life [20]. Heng Zhang (2019) et
al purpose a cohort study in China to identify the health-related
quality of life in children. The study sample size was 42 children
and the data was collected from kid’s life assessment tools. The
conclusion of that study was health-related quality of life decrease
in the children with hemophilia which depend on the severity
of hemophilia or joint bleeding and bleeding joint decrease the
activity of limitation [21].
MjidDavari and Zahra Gheribnaseri (2019) et al. conducted
a cross-sectional study to determine the joints health status
and living quality in hemophilia patients. The data was collected
from the HR-QO2 questioner and joint health is to collect from
hemophilic joint health score the study sample size was 38 people
with hemophilia. They concluded that health-related quality of life
in hemophilia patients was very low and many joints problems are
found due to bleeding in joints [22]. Merel A and timmer (2020)
purpose a study to determine the movement or behavior pattern
in hemophilia patients. The study sample size was 107 people who
have hemophilia. They collect the data from the Kruskal wall test
and HJHS TOOLS. They found that runner and bike person with
hemophilia is a few limitations in their life and they also concluded
that sitting or standing was better for joint health [23]. In 2019 Dr.
Edward Nguyo Maina purpose a cross-sectional study to find the
prevalence of musculoskeletal problems in people with hemophilia.
His study sample size was 37 people with hemophilia. He was data
collected from the gilbert joint scoring system. He found that 86.5
% recurrent bleeding in joint, 75.7% of people have limited range
of motion, and 70% have flexion contracture formation in joint with
hemophilia. They found that musculoskeletal problems was linked
with the severity of diseases [24].
Objective
The objective of this study was to determine the: “Level of activity limitation due to joint pain among hemophilia patients.”
Rationale
Hemophilia causes activity limitation or other health disorders in children. The Research gap exist to determine the level of activity limitation occur in hemophilia patients due to pain in joints. This study may also helpful for physiotherapy field to find the best physiotherapy treatment for hemophilia patients regarding their activity limitation. The main rationale of my study to find advance prevention and eliminates the activity limitation risk factor in further studies.
Operational Definitions
Outcome measure tools that was used in the study is Activilm
Questionnaire.
The ACTIVILM Questionnaire focus on assessing the basic
knowledge of activity limitation by different question their correct
answer [25].
Variables:
a) Dependent variable: Activity limitation & pain
b) Independent variable: Hemophilia patient are independent
variable.
Value of sensitivity/ specificity/validity/ reliability=0.95.
Materials and Methods
A. Study Design: Design of study was Cross-Sectional.
B. Study Settings: Data for this research was gathered from
hemophilic center in Lahore.
C. Duration of Study: 06 months.
D. Sample Size: Sample size is calculated using following formula
and parameters.
Here
Z 1−α/2 = is standard normal variate (at 5% type 1 error (P<0.05)
it is 1.96 and at 1% type 1 error (P<0.01) it is 2.58). As a majority
of studies P values are considered significant below 0.05 hence 1.96
is used in formula.
p = Expected proportion in population based on previous
studies or pilot studies.
d= Absolute error or precision − Has to be decide by researcher
Using 75.7% proportion of the condition sample size is 152
(Table 1).
Table 1: Antibody characterics used for immunohistochemistry.
Nguyo, E.M., Prevalence of musculoskeletal complications among hemophilia patients as seen at Kenyatta National Hospital. 2020, University of Nairobi.
E. Sample Technique: Non-probability convenient sampling
was used.
F. Criteria of Sample Selection:
a) Inclusion Criteria:
i. Hemophilia patients.
ii. Age between 5-19 years.
b) Exclusion Criteria: The people who have joint bleeding due
to hematoma or other joint disorder such as juvenile arthritis.
Data Collection Procedure
The data was collected after approval from the ethical board of concerned institute. The study design for the study was a descriptive cross-sectional study. The data collected from only people with hemophilia diseases. A convenience non-probability is used as a sampling technique for a minimum sample size of 152 and father data was added according to study requirement to minimum choice of error. The duration of the study was of 6 months and eligibility criteria for participants include volunteers. The data was collected from the ACTIVLIM questionnaire that including the activity limitation assessment and knowledge. The data was collected in the different hemophilic centers in Lahore city. The data collected in the form of a hard copy. And distribute to hemophilia patients. Hemophilia patient was filled the form.
Ethical Consideration
The data was collected after the approval of the ethical board. The participant was provided with information regarding the study and informed consent was signed by the participant. Volunteers were preferred. The identity of participants kept confidential and the participant was allowed to withdraw from the study.
Statistical Analysis
Data was analyzed by using SPSS software for the questionnaire.
Results
a) Among 152 participants, male were 146(96.1%) and female were 6(3.9%) (Table 2 & Figure 1).
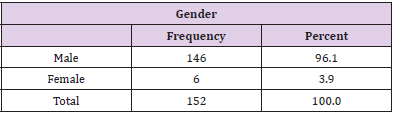
Table 2: Frequency distribution of Difficulty in gender.
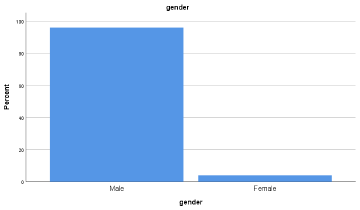
Figure 1: Frequency distribution of Difficulty in gender
b) Among 152 participants, Putting on a T Shirt was difficult among 27(17.8%) and Easy among s125 (82.2%) (Table 3 & Figure 2).
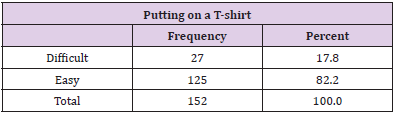
Table 3: Frequency distribution of Difficulty in Putting on a T shirt.
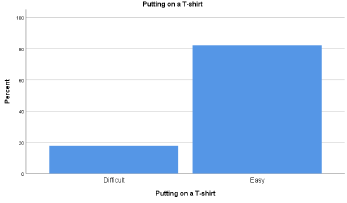
Figure 2: Frequency distribution of Difficulty in Putting on a T shirt.
c) Among 152 participants, Washing ones upper body was difficult among 35(23.0%) and Easy among 117(77.0%) (Table 4 & Figure 3).
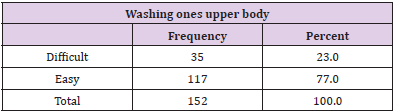
Table 4: Frequency distribution of Difficulty in Washing Ones Upper Body.
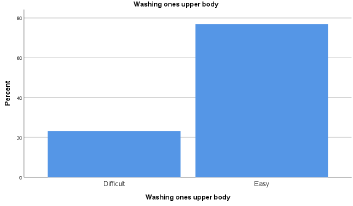
Figure 3: Frequency distribution of Difficulty in Washing Ones Upper Body.
d) Among 152 participants, Dressing ones lower body was difficult among 83(54.6%) and Easy among 69(45.4%) (Table 5 & Figure 4).
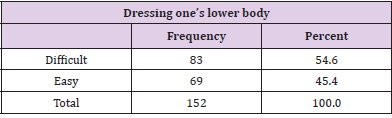
Table 5: Frequency distribution of Difficulty in Dressing Ones Lower Body.
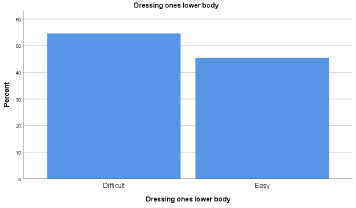
Figure 4: Frequency distribution of Difficulty in Dressing Ones Lower Body.
e) Among 152 participants, Taking a Shower was Impossible among 2(1.3%), difficult among 87(57.2%) and Easy among 63(45.4%) (Table 6 & Figure 5).
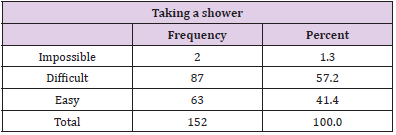
Table 6: Frequency distribution of Difficulty in Taking a Shower.
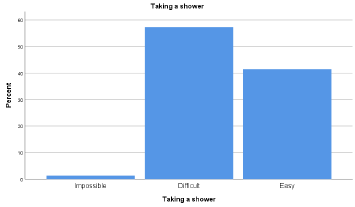
Figure 5: Frequency distribution of Difficulty in Taking a Shower.
f) Among 152 participants, Sitting on the toilet was Impossible among 12(7.9%), difficult among 91(59.9%) and Easy among 49(32.2%) (Table 7 & Figure 6).
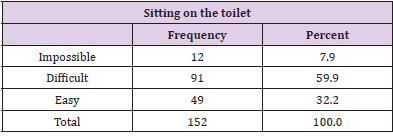
Table 7: Frequency distribution of Difficulty in Sitting on the Toilet.
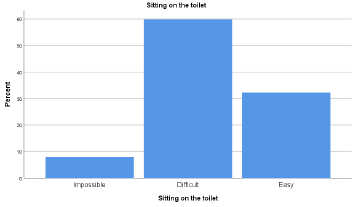
Figure 6: Frequency distribution of Difficulty in Sitting on the Toilet.
g) Among 152 participants, Taking a bath was Impossible among 4(2.6%), difficult among 85(55.9%) and Easy among 63(41.4%) (Table 8 & Figure 7).
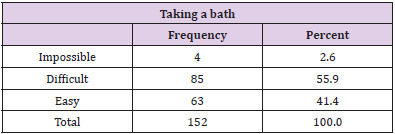
Table 8: Frequency distribution of Difficulty in taking a bath.
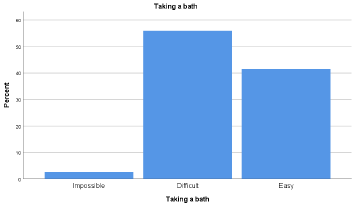
Figure 7: Frequency distribution of Difficulty in taking a bath.
h) Among 152 participants, Walking Upstairs was Impossible among 9(5.9%), difficult among 96(63.2%) and Easy among 47(30.9%) (Table 9 & Figure 8).
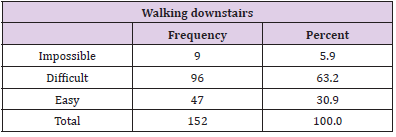
Table 9: Frequency distribution of Difficulty in walking downstairs.
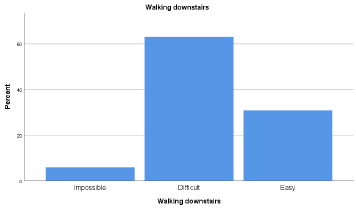
Figure 8: Frequency distribution of Difficulty in walking downstairs.
i) Among 152 participants, Stepping out of a bath tub was Impossible among 1(0.7%), difficult among 53(34.9%) and Easy among 98(64.5%) (Table 10 & Figure 9).

Table 10: Frequency distribution of Difficulty in Stepping out of a bathtub.
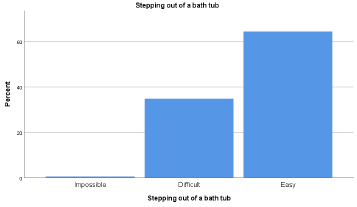
Figure 9: Frequency distribution of Difficulty in Stepping out of a bath tub.
j) Among 152 participants, Opening a door was difficult among 12(7.9%) and Easy among 140(92.1%) (Table 11 & Figure 10).
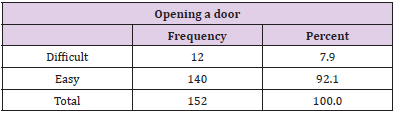
Table 11: Frequency distribution of Difficulty in opening a door.
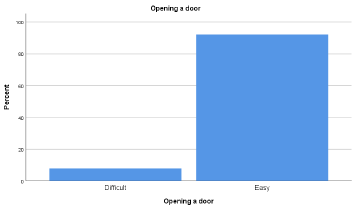
Figure 10: Frequency distribution of Difficulty in opening a door.
k) Among 152 participants, Walking outdoor on level ground was Impossible among 4(2.6%), difficult among 52(34.2%) and Easy among 96(63.2%) (Table 12 & Figure 11).

Table 12: Frequency distribution of Difficulty in walking outdoors on level ground.
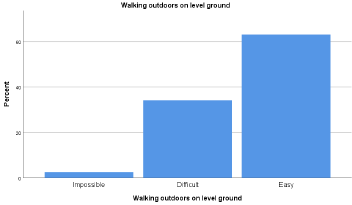
Figure 11: Frequency distribution of Difficulty in walking outdoors on level ground.
l) Among 152 participants, Washing ones face was difficult among 25(16.4%) and Easy among 127(83.6%) (Table 13 & Figure 12).
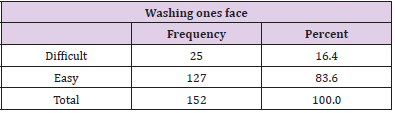
Table 13: Frequency distribution of Difficulty in washing ones face.
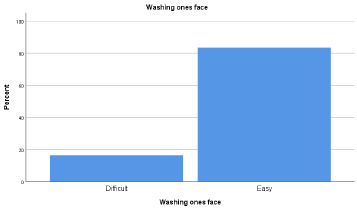
Figure 12: Frequency distribution of Difficulty in washing ones face.
m) Among 152 participants, hanging up a jacket on a hat stand was difficult among 67(44.1%) and Easy among 85(55.9%) (Table 14 & Figure 13).
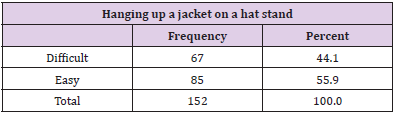
Table 14: Frequency distribution of Difficulty in Hanging up a jacket on a hat stand.
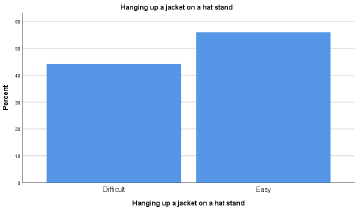
Figure 13: Frequency distribution of Difficulty in Hanging up a jacket on a hat stand.
n) Among 152 participants, Wiping ones upper body was Impossible among 1(0.7%), difficult among 52(34.2%) and Easy among 99(65.1%) (Table 15 & Figure 14).
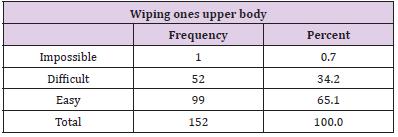
Table 15: Frequency distribution of Difficulty in wipes ones upper body.
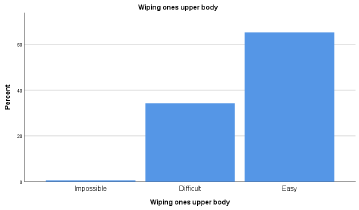
Figure 14: Frequency distribution of Difficulty in wipes ones upper body.
o) Among 152 participants, walking upstairs was Impossible among 6(3.9%), difficult among 134(88.2%) and Easy among 12(7.9%) (Table 16 & Figure 15).
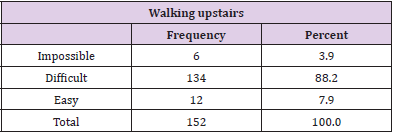
Table 16: Frequency distribution of Difficulty in walking upstairs.
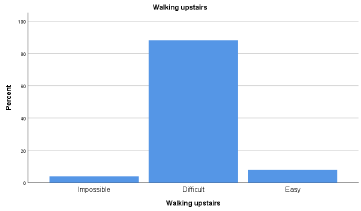
Figure 15: Frequency distribution of Difficulty in walking upstairs.
p) Among 152 participants, Carrying a heavy load was Impossible among 13(8.6%), difficult among 133(87.5%) and Easy among 6(3.9%) (Table 17 & Figure 16).
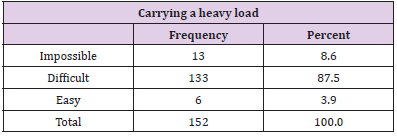
Table 17: Frequency distribution of Difficulty in carrying a heavy load.
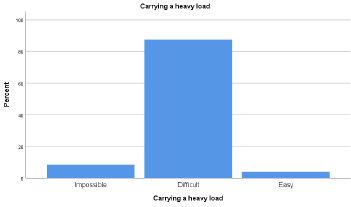
Figure 16: Frequency distribution of Difficulty in carrying a heavy load.
q) Among 152 participants, Getting in to a car was difficult among 24(15.8%) and Easy among 128(84.2%) (Table 18 & Figure 17).
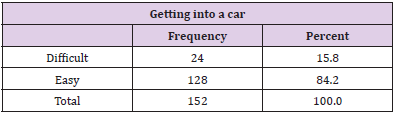
Table 18: Frequency distribution of Difficulty in getting into a car.
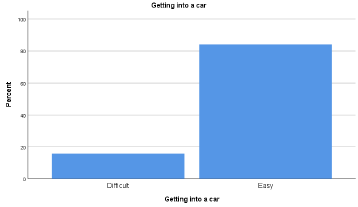
Figure 17: Frequency distribution of Difficulty in getting into a car.
r) Among 152 participants, Standing for a long time was Impossible among 12(7.9%), difficult among 117(77.0%) and Easy among 23(15.1%) (Table 19 & Figure 18).
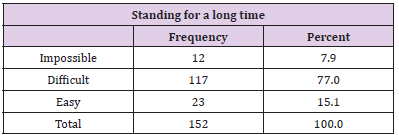
Table 19: Frequency distribution of Difficulty in Standing for a long time.
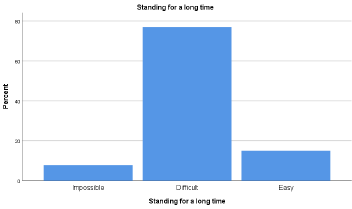
Figure 18: Frequency distribution of Difficulty in Standing for a long time.
s) Among 152 participants, Walking more than 1 km was Impossible among 23(15.1%), difficult among 117(77.0%) and Easy among 12(7.9%) (Table 20 & Figure 19).
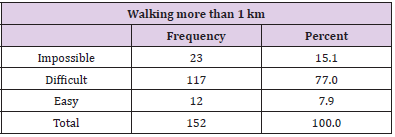
Table 20: Frequency distribution of Difficulty in walking more than 1 km.
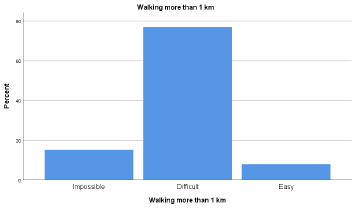
Figure 19: Frequency distribution of Difficulty in walking more than 1 km.
t) Among 152 participants, Closing a door was difficult among 8(5.3%) and Easy among 144(94.7%) (Table 21 & Figure 20).
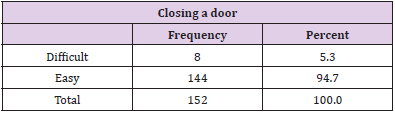
Table 21: Frequency distribution of Difficulty in closing a door.
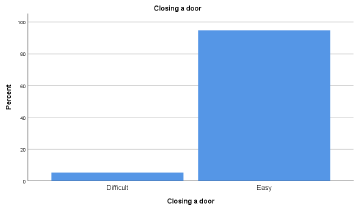
Figure 20: Frequency distribution of Difficulty in closing a door.
u) Among 152 participants, Hopping on one foot was Impossible among 5(3.3%), difficult among 97(63.8%) and Easy among 50(32.9%) (Table 22 & Figure 21).
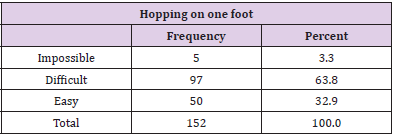
Table 22: Frequency distribution of Difficulty in Hopping on one foot.
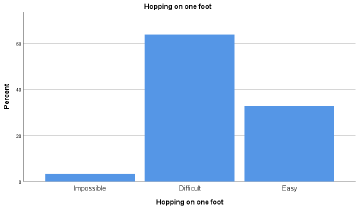
Figure 21: Frequency distribution of Difficulty in Hopping on one foot.
v) Among 152 participants, Putting on a backpack was Impossible among 3(2.0%), difficult among 105(69.1%) and Easy among 44(28.9%) (Table 23 & Figure 22).
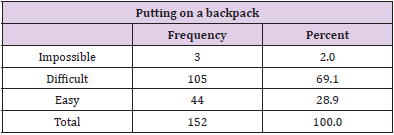
Table 23: Frequency distribution of Difficulty in putting on a backpack.
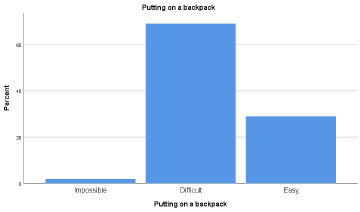
Figure 22: Frequency distribution of Difficulty in putting on a back pack.
w) Among 152 participants, Running was Impossible among 17(11.2%), difficult among 134(88.2%) and Easy among 1(0.7%) (Table 24 & Figure 23).
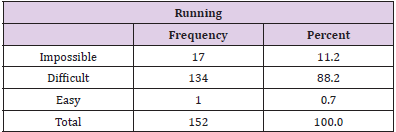
Table 24: Frequency distribution of D.
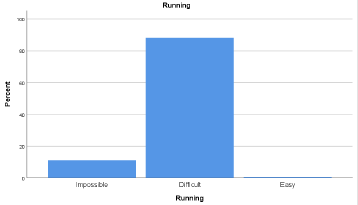
Figure 23: Frequency distribution of Difficulty in Running.
Discussion
A study conducted by Buckner, Tyler Win 2018, Study aimed
to determine the Assessments of pain, functional impairment,
anxiety and depression in US adults with hemophilia. According to
this study, participants reported feeling tired (93 percent), worn
out (86 percent), very nervous (68 percent), downhearted and
depressed (55 percent) and so down in the dumps that nothing
could cheer them up (41 percent). According to our study Among
152 participants, male were 146(96.1%) and female were 6(3.9%).
Putting on a T Shirt was difficult among 27(17.8%) and Easy
among 125(82.2%).Washing ones upper body was difficult among
35(23.0%) and Easy among 117(77.0%).Dressing ones lower
body was difficult among 83(54.6%) and Easy among 69(45.4%).
Taking a Shower was Impossible among 2(1.3%), difficult among
87(57.2%) and Easy among 63(45.4%).Sitting on the toilet was
Impossible among 12(7.9%), difficult among 91(59.9%) and Easy
among 49(32.2%).Taking a bath was Impossible among 4(2.6%),
difficult among 85(55.9%) and Easy among 63(41.4%) [25].
A study revealed patient was unable to perform the activity,
or need complete assistance to perform the activity like transfers/
squatting and running. Some need partial assistance/aids/
modified instruments/modified environment to perform the
activity like eating, bathing, dressing going up a stairs, walking
running. The other group able to perform the activities without
aids or assistance, but with slight discomfort, unable to perform
the activities similar to their healthy peers like eating, bathing,
dressing going up a stairs, walking and running. A few subjects
were able to perform the activities without any difficulty similar to
their healthy peer. According to our study among 152 participants,
walking upstairs was Impossible among 9(5.9%), difficult among
96(63.2%) and Easy among 47(30.9%). Stepping out of a bath
tub was impossible among 1(0.7%), difficult among 53(34.9%)
and Easy among 98(64.5%).Opening a door was difficult among
12(7.9%) and Easy among 140(92.1%).Walking outdoor on
level ground was Impossible among 4(2.6%), difficult among
52(34.2%) and Easy among 96(63.2%). Washing ones face was
difficult among 25(16.4%) and Easy among 127(83.6%). Hanging
up a jacket on a hat stand was difficult among 67(44.1%) and Easy
among 85(55.9%). Wiping ones upper body was Impossible among
1(0.7%), difficult among 52(34.2%) and Easy among 99(65.1%).
walking upstairs was Impossible among 6(3.9%), difficult among
134(88.2%) and Easy among 12(7.9%) [26].
According to another study knees (23.7 percent), elbows (23.7
percent) and ankles (37.4 percent) were the most often reported
sore joints (18.9 percent) among hemophilia patients. On the
International Physical Activity Questionnaire, 51% said they had
done nothing in the previous week. The median sub scores for four
physical health domains were lower than the median sub scores
for four mental health domains on the SF-36v2 health survey. Leg
functions (median, 66.7) and lying/sitting/kneeling/standing
(median, 67.5) were the most impacted Hemophilia Activities List
domains (range 0 (worst)-100 (best)), whereas self-care was the
least impacted (median, 100.0). Ankle scores (median, 6.0; range,
0-40) on the HJHS were lower than elbow/knee scores (median,
4.0/4.0).and according to our study Among 152 participants,
Carrying a heavy load was Impossible among 13(8.6%), difficult
among 133(87.5%) and Easy among 6(3.9%). Getting in to a car was
difficult among 24(15.8%) and Easy among 128(84.2%). Standing
for a long time was Impossible among 12(7.9%), difficult among
117(77.0%) and Easy among 23(15.1%). Walking more than 1 km
was Impossible among 23(15.1%), difficult among 117(77.0%) and
Easy among 12(7.9%). Closing a door was difficult among 8(5.3%)
and Easy among 144(94.7%). Hopping on one foot was Impossible
among 5(3.3%), difficult among 97(63.8%) and Easy among
50(32.9%). Putting on a backpack was Impossible among 3(2.0%),
difficult among 105(69.1%) and Easy among 44(28.9%). Running
was Impossible among 17(11.2%), difficult among 134(88.2%) and
Easy among 1(0.7%) [27].
Conclusion
Pain was observed most common problem that affected daily activities and quality of life among hemophilia patients. Respondents reported functional impairment that limit the daily routine work and activities they participated in especially with activities involving the lower extremities.
Limitations
a) Due to low population of hemophilia so data collection took
time.
b) The data was collected from single hemophilia center in
Lahore.
c) Difficulties in collection of data because of Covid-19.
Recommendation
a) Study should be analyzed through clinical analysis in future.
b) Seminars can be conducted to spread the awareness among
patients.
c) Longitudinal study should be conducted to evaluate the long
term effects of hemophilia on joint pain.
d) The data should be collected from all over hemophilia
treatment centers of Pakistan.
References
- Konkle BA, Huston H (2017) Hemophilia a.
- Franchini M, Mannucci PM (2014) Editors. The history of hemophilia. Seminars in thrombosis and hemostasis: Thieme Medical Publishers 40(5): 571-576.
- Stoffman J, Andersson N, Branchford B, Batt K, D’Oiron R, et al.( 2019) Common themes and challenges in hemophilia care: a multinational perspective. Hematology 24(1): 39-48.
- Qu Y, Nie X, Yang Z, Yin H, Pang Y, et al. ( 2014) The prevalence of hemophilia in mainland China: a systematic review and meta-analysis. Southeast Asian Journal of Tropical Medicine and Public Health 45(2): 455-466.
- Dorgalaleh A, Dadashizadeh G, Bamedi T (2016) Hemophilia in Iran. Hematology 21(5): 300-310.
- Rodriguez-Merchan E (2012) Prevention of the musculoskeletal complications of hemophilia. Advances in preventive medicine.
- Witkop M, Neff A, Buckner T, Wang M, Batt K, et al. (2017) Self‐reported prevalence, description and management of pain in adults with haemophilia: methods, demographics and results from the Pain, Functional Impairment, and Quality of life (P‐FiQ) study. Haemophilia 23(4): 556-565.
- Forsyth AL, Witkop M, Lambing A, Garrido C, Dunn S, et al. (2015) Associations of quality of life, pain, and self-reported arthritis with age, employment, bleed rate, and utilization of hemophilia treatment center and health care provider services: results in adults with hemophilia in the HERO study. Patient preference and adherence 9: 1549-1560.
- Elander J, Robinson G, Mitchell K, Morris J (2009) An assessment of the relative influence of pain coping, negative thoughts about pain, and pain acceptance on health-related quality of life among people with hemophilia. PAIN® 145(1-2): 169-175.
- Roosendaal G, Lafeber FP, Editors (2003) Blood-induced joint damage in hemophilia. Seminars in thrombosis and hemostasis; Copyright© 2003 by Thieme Medical Publishers, Inc, 333 Seventh Avenue, New …. 29(1): 37-42.
- Iannone M, Pennick L, Tom A, Cui H, Gilbert M, et al. (2012) Prevalence of depression in adults with haemophilia. Haemophilia 18(6): 868-874.
- Kempton CL, Wang M, Recht M, Neff A, Shapiro AD, et al. (2017) Reliability of patient-reported outcome instruments in US adults with hemophilia: the Pain, Functional Impairment and Quality of life (P-FiQ) study. Patient preference and adherence 11: 1603-1612.
- Manco-Johnson MJ, Soucie JM, Gill JC (2017) Prophylaxis usage, bleeding rates, and joint outcomes of hemophilia, 1999 to 2010: a surveillance project. Blood 129(17): 2368-2374.
- Rodriguez-Merchan E. (1996) Effects of hemophilia on articulations of children and adults. Clinical Orthopaedics and Related Research (1976-2007) 328: 7-13.
- Cutter S, Molter D, Dunn S, Hunter S, Peltier S, et al. (2017) Impact of mild to severe hemophilia on education and work by US men, women, and caregivers of children with hemophilia B: The Bridging Hemophilia B Experiences, Results and Opportunities into Solutions (B‐HERO‐S) study. European journal of haematology 98: 18-24.
- Wang M, Batt K, Kessler C, Neff A, Iyer NN, et al. (2017) Internal consistency and item-total correlation of patient-reported outcome instruments and hemophilia joint health score v2. 1 in US adult people with hemophilia: results from the pain, functional impairment, and quality of life (P-FiQ) study. Patient preference and adherence 11: 1831-1839.
- Varni J (1981) Behavioral medicine in hemophilia arthritic pain management: two case studies. Archives of physical medicine and rehabilitation 62(4): 183-187.
- Kempton CL, Buckner TW, Fridman M, Iyer NN, Cooper DL (2018) Factors associated with pain severity, pain interference, and perception of functional abilities independent of joint status in US adults with hemophilia: Multivariable analysis of the Pain, Functional Impairment, and Quality of Life (P‐FiQ) study. European journal of haematology 100: 25-33.
- Soucie JM, Cianfrini C, Janco RL, Kulkarni R, Hambleton J, et al. (2004) Joint range-of-motion limitations among young males with hemophilia: prevalence and risk factors. Blood 103(7): 2467-2473.
- Monahan PE, Baker JR, Riske B, Soucie JM (2011) Physical functioning in boys with hemophilia in the US. American journal of preventive medicine 41(6): S360-S368.
- Zhang H, Huang J, Kong X, Ma G, Fang Y (2019) Health-related quality of life in children with haemophilia in China: a 4-year follow-up prospective cohort study. Health Qual Life Outcomes 17(1): 28.
- Davari M, Gharibnaseri Z, Ravanbod R, Sadeghi A (2019) Health status and quality of life in patients with severe hemophilia A: A cross-sectional survey. Hematology reports 11(2): 7894.
- Timmer MA, Veenhof C, de Kleijn P, de Bie RA, Schutgens RE, et al. (2020) Movement behaviour patterns in adults with haemophilia. Therapeutic advances in hematology 11: 2040620719896959.
- Nguyo EM (2020) Prevalence of musculoskeletal complications among hemophilia patients as seen at Kenyatta National Hospital: University of Nairobi.
- Buckner TW, Batt K, Quon D, Witkop M, Recht M, et al. (2018) Assessments of pain, functional impairment, anxiety, and depression in US adults with hemophilia across patient‐reported outcome instruments in the Pain, Functional Impairment, and Quality of Life (P‐FiQ) study. European journal of haematology 100(1): 5-13.
- Ferreira AA, Bustamante-Teixeira MT, Leite ICG, Corrêa CSL, Rodrigues DdOW, et al. (2013) Clinical and functional evaluation of the joint status of hemophiliac adults at a Brazilian blood center. Revista brasileira de hematologia e hemoterapia 35(1): 23-28.
- Kempton C, Recht M, Neff A, Wang M, Buckner T, et al. (2018) Impact of pain and functional impairment in US adults with haemophilia: Patient‐reported outcomes and musculoskeletal evaluation in the pain, functional impairment and quality of life (P‐FiQ) study. Haemophilia 24(2): 261-270.
