 Review Article
Review ArticleABSTRACT
Background: Genetic counsellors are uniquely qualified to address cancer risk,
interpretation of genetic results, and the inevitable complications of the subsequent
ethical, legal and psychosocial issues that are encountered by individuals dealing with
cancer and with the evolution of technology that can aid in screening and testing, it has
become increasingly important for a country like India to evolve its healthcare policies
accordingly.
Main Body: Entry into and the timing of the first genetic counsellor’s referral hold
importance as they are based on family history, ethnicity, phenotypic expressions,
high-risk tumour types, non-oncological findings and incidental findings, and ensure
that all prophylactic measures, possible tests, therapies and management options are
considered. Testing procedures on the gene-level is based on examination of entire
genomes and of specific genes in order to estimate the pathogenicity of the variant.
Moreover, risk stratification is an important tenet of genetic counselling that has
enormous implications on the psychosocial well-being of the patient and their families.
In India, the burden of cancer varies in accordance with gender, religion, socio-economic
status and the resolution of this adversity seems to lie in the development of nationwide
policies aimed at improving access to healthcare including evolving technologies
for screening and management.
Conclusion: Cancer screening, testing, management are all aspects of genetic
counselling that should evolve in accordance contemporary developments in the
respective fields. Personalised medicine, e-health interventions and population-based
screening are some examples of the aforementioned development.
Keywords: Genetic Counselling; Genetic Testing; Cancer Genetics
Background
The field of cancer screening and testing has come a long way;
its evolution from basic biochemical tests screening for particular
analytes [1] to the use of gene-based testing and screening models
is a definitive example of the evolution of our understanding of
cancer syndromes and their underlying genetic basis. Identification
of people with cancer predisposition syndromes and germ line
pathogenic variants [2] has become easier with the advent
and utilization of genome-wide gene sequencing panels [3,4]
chromosomal arrays, and whole exome/genome sequencing
and, somatic tumor testing (especially for childhood cancers),
emphasizing the increasing necessity for both cancer predisposition
testing and genetic counselling programs specializing in the testing,
management and care of cancer [5].
Genetic counsellors are uniquely qualified to address
cancer risk, interpretation of genetic results, and the inevitable
complications of the subsequent ethical [6], legal and psychosocial
issues that are encountered by individuals dealing with this malady
[7,8]. Obtaining informed consent [5,6] from both minors and
adults, ascertaining the timing for a genetics referral, providing
periodic counselling and the associated aid overtime (especially
in the smooth transition of younger patients to adult/ geriatric
care) [8,9] and the dearth of childhood cancer predisposition
syndromes are some of the unique challenges that plague us today
[10]. Incidental findings due to the prevalence of genetic testing are
associated with their own set of psychological implications [11].
In countries like India, where there is enormous disparity
between socio-economic classes, a genetic counsellor will
encounter additional problems including the lack of awareness
and education amongst the under-privileged classes, genderand
religion-associated disparity in terms of cancer treatment,
management and the reality of the influence of political agendas
over government health policies.
Entry to Genetic Counselling
Referral to a genetic counselling clinic for cancer evaluation can
occur due to the prevalence of cancer syndromes within the family
(family history) [12], ethnicity [13,14], phenotypic expressions,
high-risk tumour types, non-oncological findings, like the lippigmentation
and greater the characteristic macules associated
with Peutz-Jeghers syndrome and neurofibromatosis type1 (and
bi-allelic mismatch repair) respectively and incidental findings
(variances in predisposition genes on chromosomal microarrays
and secondary findings detected by exome sequencing) [9]. Family
history alone, however, is not a reliable factor when accounting
for the necessity of a referral as cancer predisposition has been
reported in many cases of absence of said history [10], This can
be due to the formation de novo variants, parental germ line
mosaicism [15], increasing incidence of smaller nuclear families,
low penetrance and recessive inheritance masking an inherited
syndrome. Hence, a combination of the aforementioned factors
should be taken into account when making a genetics’ referral.
Moreover, the future holds the possibility population based genetic
testing for cancer predisposition syndromes.
Oncologists are confronted with the possibilities of identifying
whether reported variants are indicative of somatic changes or
inherent germ line susceptibility [16] and thus subsequent referral
to a genetics’ clinic for their particular expertise becomes necessary.
Timing of Genetic Counselling Initiation
The optimal timing of the first genetic counselling session is at the time of tumor diagnosis or after the initiation of treatment in cases of poor prognosis, to ensure that the possibility of prophylactic surgery is considered. The genetic counsellor is qualified to advise the patient on many issues associated with the patient prognosis, associated treatment plans and psychological developments [17,18]. In the case of poor prognosis, DNA banking should be administered, and genetic testing organized in a timely manner in order to assess and counsel their relatives to minimize the economic and psychological burden of post-mortem testing.
Pre-Test Genetic Counselling
Informed consent should be obtained from the patient before they undergo any genetic testing procedure. This involves complete discussion of all aspects related to the test and consequent implications, including information regarding tests most suitable to the patient (based on the various factors that have prompted the referral), the surveillance protocol that may follow (especially in cases of transition from childhood to adulthood), psychosocial [11], ethical and privacy concerns, which all vary in accordance with the laws of different countries, and plans for disclosing results to at-risk relatives [6,19]. Adults are required to provide verbal and written assent towards the procedure; minors should be guided through these discussions in an age-appropriate manner and adolescents should provide verbal and written consent in conjunction with their parents or primary guardians [9]. This allows older children to become involved with and more accustomed to their unique situation and have any fears or misconceptions addressed. The basic tenet of genetic counselling is to give patients the tools required for them to make informed autonomous decisions [20] regarding the testing and management options available to them based on factual (stratified) risk information [21-25]. Despite concerns of exacerbating patients’ anxiety, genetic testing in the absence of prior genetic counselling is linked with negative outcomes including the violation of ethical standards, ordering of unnecessary, perhaps costly, genetic tests, misinterpretation of these results and adverse effects on the patients’ psyche.
Genetic Testing
The invention of Next Generation Sequencing (NGS) technology is the biggest advancement in genetic testing seen in recent years wherein analysis is performed at a multiple gene level, or even whole transcriptomic, genomic and exomic levels, at a relatively lower cost, especially when the increased sensitivity and efficiency of obtaining results are taken into account [16]. A test should be ordered after consultation with a genetic counsellor and the choice of laboratory should be based on the type of test, its level of analysis, methodology and their variant interpretation techniques, expenses involved, time factors and their policies on privacy and ethics. The variants are reported in accordance with the five-tier classification proposed by The American College of Medical Genetics and Genomics (ACMG), namely, pathogenic, likely pathogenic, variant of uncertain significance, likely benign and benign [9,26]. Despite the succinctness of this model, further interpretation by an expert is important especially when deciding the significance/ level of pathogenicity of variants (Table 1).
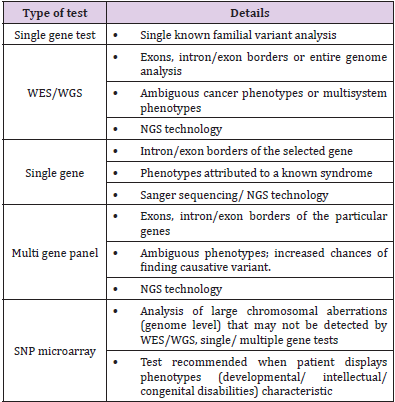
Table 1: Genetic tests for cancer gene mutation.
Note: {WES – Whole Exome Sequencing; WGS – Whole Genome Sequencing, NGS – Next Generation Sequencing, SNP – Single Nucleotide Polymorphism}
The sensitivity of these tests for identification of pathogenicity varies from greater than 95% to less than 50% and thus, a genetic counsellor must provide counsel on risk perception and management options based on empirical data and in conjunction with the oncologist. Identification of variants without certain significance tailors the advised management options to include surveillance protocols and the possibility of family variant tracking. Relatives can be tested for these only when consent is provided by the patient [6]. The inheritance patterns associated with the identified pathogenic variant determine the relatives who are atrisk. For example, if a syndrome follows an autosomal dominant pattern of inheritance, there is a 50% risk of inheriting a pathogenic variant, and its associated risks, to first-degree relatives of the proband [16,27].
Post- Test Genetic Counselling
For those individuals with a positive diagnosis, post-test counselling involves specific treatment/ management options and the necessity of periodic evaluation. In cases of childhood diagnosis of a hereditary cancer syndrome, reproductive and psychological implications especially, change over increasing age. Hence, lifelong risk management, and understanding of the options for reproductive (post- and pre-natal) counselling [28], testing post-birth, adoption, and/or utilizing donors is disseminated with increasing age of the patient in an appropriate manner suited to the child’s developmental stage8,9. Surveillance options [29] and information regarding the advent of new testing options can only be provided for at-risk individuals/ families if periodic follow-up with the genetic counsellor is maintained.
Psychological and Sociological Implications
Negative effects on the psyche of a patient with a positive
diagnosis are primarily concerned with surveillance protocols
and the reality of a life-long economic burden8. Invasive medical
procedures [30], procedures requiring sedation or general
anesthesia, false positive results, incidental findings are implicated
by various studies in causing psychological distress to the patient
and their families. There arises a general frustration with lack of
positive results when it comes to therapies advised, inconclusive
outcomes of tests and the delivery of false-positive results
(increased in whole-body MRIs) [31], impaired quality of life,
reduced satisfaction with care, and worse overall survival. Patients
undergoing surveillance may experience anxiety with regards to
scanning, referred to as “scanxiety”, and children especially may feel
adversely towards repeated blood draws and the claustrophobic
confinement experienced during MRI scans [9]. Young adults
face an ever-increasing economic burden as they are as of yet not
financially secure enough, and may not even possess insurance
cover [20], to support life- long management programs.
On the contrary, proactive surveillance and psychological
support, from say, cancer survivor groups, may empower the
patient and are viable avenues to lead a more well-adjusted life. The
patient relies on the care team in such scenarios due to generation
of trust and confidence in their counsel [32,33]. Cancer genetic
counselling in India. In India, there are about a million cases of
cancer diagnosed yearly. When the population of the subcontinent
is taken into account, these rates of incidence and mortality, match
those seen in high-income countries [34]. These elucidate the lack
of early-detection strategies and positive results of treatments
within the medical landscape of the country [35].
Studies show that breast, lung, oral, cervical, gastric and
colorectal cancers [36] have the highest incidence rates in India. It
is evident that most causative agents implicated in cancer in the
Indian population are avoidable (tobacco and alcohol consumption,
lack of education with respect to female hygiene) [34,37]. There is
a general lack of education and support for the low-income, socially
underprivileged families owing to the fallacies of an increasingly
capitalist state of government [38-40]. Even governmental policies
regarding general health are found to be inadequate in the face of growing mortality due to cancer. It is the second-leading cause of
death amongst the Indian population.
A patriarchal society has also generated the spread of female
reproductive cancers as the importance of feminine hygiene is not
acknowledged by many; additionally, a greater economic burden to
finance health care is placed on women [41]. In conjunction with
the lack of resources and such a mind-set, most evidently seen in
under-privileged communities, the incidence of cervical cancers
has witnessed an increase over the past 5-10 years. In India, the
age of onset of the female reproductive cancers is around a decade
earlier than that of developed nations (45-50 years in the former,
compared to >60 years of the latter) [42]. Moreover, oncofertility
can be improved by developing management, treatment strategies
that comprise of professionals from multiple specialties, say a
counselling team that includes a reproductive endocrinologist [43]
apart from an oncologist, psychologist and the geneticist. Hence,
advancement of cancer-associated clinical programs with respect
to diagnosis, screening, management/ treatment particular to the
Indian race [44] are a necessity in the mission to better the state of
women’s health in India [42,45].
Conclusion
Cancer testing and management is an ever-growing field primarily due to our increasing understanding of unknown syndromes and their underlying genetics, and the expansion of available information of known cancer syndromes. In accordance with these basic developments, there should be a correlating evolution in the various genetic testing and counselling practices available for the same. These take the form of improved access to aforementioned resources and formulations of government policies that tackle health care from this perspective [45]. One such advancement can be the necessitation of population-based genetic screening [46,47] and testing for common pathogenic variants of the most abundantly found cancer syndromes, e.g. BRCA 1 and 2 testing for breast cancer [4,42,48]. This type of policy can hold many implications in reducing the burden of cancer in many developing economies, like India. In the same vein, there have been discussions on the use of e-health interventions [49] like psychoeducational interventions delivered via web-based environments with auxiliary methods of communication, which includes support with professionals and peers, offer improved awareness and access to the required support for informed, autonomous decisionmaking. Personalized medicine is an avenue of modern medicine gaining quick popularity as it is tailored to an individual and their needs. Corroborating advancements in cancer genetic testing and counselling to personalized care will initiate the incidence of more positive outcomes as it pertains to lifelong care and management practices [5,11,18,50,51].
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for Publication
Not Applicable.
Availability of Data and Materials
Not Applicable.
Competing Interests
None.
Funding
No Funding was obtained for the present review.
Author’s Contributions
Gatika Agrawal(GA) and Venkatachalam Deepa Parvathi(VDP) have contributed equally to the conception, drafting, revising it critically and intellectual content. Arunasalam Dharmarajan (AD) contributed to reviewing the manuscript.
Conflict of Interest Statement
Authors, Gatika Agrawal, Venkatachalam Deepa Parvathi and Arunasalam Dharmarajan declare that they have no conflict of interest.
References
- Andrici J, Gill AJ, Hornick JL (2018) Next generation immunohistochemistry: Emerging substitutes to genetic testing? Semin Diagn Pathol 35(3):161-169.
- Jun Tu Zhen, Jamil Syed, Kevin Anh Nguyen, Michael S Leapman, Neeraj Agarwal, et al. (2018) Genetic testing for hereditary prostate cancer: Current status and limitations. Cancer.
- Lorans M, Dow E, Macrae FA, Winship IM, Buchanan DD (2018) Update on Hereditary Colorectal Cancer: Improving the Clinical Utility of Multigene Panel Testing. Clin Colorectal Cancer 17(2): e293-e305.
- Jeanna M McCuaig, Tracy L Stockley, Patricia Shaw, Michael Fung-Kee-Fung, Alon D Altman, et al. (2018) Evolution of genetic assessment for BRCA-associated gynaecologic malignancies: a Canadian multisociety roadmap. J Med Genet 55(9): 571-577.
- Dancey JE, Bedard PL, Onetto N, Hudson TJ (2012) The genetic basis for cancer treatment decisions. Cell 148(3): 409-420.
- Braverman G, Shapiro ZE, Bernstein JA (2018) Ethical Issues in Contemporary Clinical Genetics. Mayo Clin Proc Innov Qual Outcomes 2(2): 81-90.
- Christian F Singer, Judith Balmaña, Nicole Bürki, Suzette Delaloge, Maria Elisabetta Filieri, et al. (2019) Genetic counselling and testing of susceptibility genes for therapeutic decision-making in breast cancer—an European consensus statement and expert recommendations. Eur J Cancer 106: 54-60.
- Seth R (2019) The After Treatment Completion Card (ATCC): medical passport for pediatric cancer survivors. Pediatr Hematol Oncol J p. 6-7.
- Harriet Druker, Kristin Zelley, Rose B McGee, Sarah R Scollon, Wendy K Kohlmann, et al. (2017) Genetic counselor recommendations for cancer predisposition evaluation and surveillance in the pediatric oncology patient. Clin Cancer Res 23(13): e91-e97.
- Brodeur GM, Nichols KE, Plon SE, Schiffman JD, Malkin D (2017) Pediatric cancer predisposition and surveillance: An overview, and a tribute to Alfred G. Knudson Jr. Clin Cancer Res 23(11): e1-e5.
- Jacobs C, Patch C, Michie S (2018) Communication about genetic testing with breast and ovarian cancer patients: a scoping review. Eur J Hum Genet.
- Agnese DM, Pollock R (2016) Breast Cancer Genetic Counseling: A Surgeon’s Perspective. Front Surg 3(January):1-7.
- Ken Batai, Alfredo Harb-De la Rosa, Aye Lwin, Fahad Chaus, Francine C Gachup, et al. (2018) Racial and Ethnic Disparities in Renal Cell Carcinoma: An Analysis of Clinical Characteristics. Clin Genitourin Cancer 17(1): e195-e202.
- Cronin KA, Howlader N, Stevens JL, Trimble EL, Harlan LC, et al. (2019) Racial Disparities in the Receipt of Guideline Care and Cancer Deaths for Women with Ovarian Cancer. Cancer Epidemiol Biomarkers & Prev 28(3): 539 LP-545.
- Navya Nair, Melissa Schwartz, Lisa Guzzardi, Nicki Durlester, Stephanie PaninL, et al. (2018) Hysterectomy at the time of risk-reducing surgery in BRCA carriers. Gynecol Oncol Reports 26(July): 71-74.
- Silke Gillessen, Gerhardt Attard, Tomasz M Beer, Himisha Beltran, Alberto Bossi, et al. (2017) Management of Patients with Advanced Prostate Cancer: The Report of the Advanced Prostate Cancer Consensus Conference APCCC 2017. Eur Urol 73(2): 178-211.
- S van Dijk, W Otten, M W Zoeteweij, DRM Timmermans, CJ van Asperen,, et al. (2003) Genetic counselling and the intention to undergo prophylactic mastectomy: effects of a breast cancer risk assessment. Br J Cancer 88(11): 1675-1681.
- Vig HS, Wang C (2012) The evolution of personalized cancer genetic counseling in the era of personalized medicine. Fam Cancer 11(3): 539-544.
- Chico V (2018) Reasonable expectations of privacy in non-disclosure of familial genetic risk: What is it reasonable to expect? Eur J Med Genet.
- Ready K, Johansen Taber KA, Bonhomme N, Lichtenfeld JL (2019) Strategies for Improving Access to Hereditary Cancer Testing: Recommendations from Stakeholders. Genet Med 0(0): 2-4.
- Schlich-Bakker KJ, Ten Kroode HFJ, Wárlám-Rodenhuis CC, Van den Bout J, Ausems MGEM (2007) Barriers to participating in genetic counseling and BRCA testing during primary treatment for breast cancer. Genet Med 9: 766.
- Lin JS, Evans C V, Grossman DC, Tseng CW, Krist AH (2018) Framework for Using Risk Stratification to Improve Clinical Preventive Service Guidelines. Am J Prev Med 54(1): S26-S37.
- Alison H Skalet, Dan S Gombos, Brenda L Gallie, Jonathan W Kim, Carol L Shields, et al. (2018) Screening Children at Risk for Retinoblastoma: Consensus Report from the American Association of Ophthalmic Oncologists and Pathologists. Ophthalmology 125(3): 453-458.
- Sobey G (2015) Ehlers-Danlos syndrome: How to diagnose and when to perform genetic tests. Arch Dis Child 100(1): 57-61.
- Islami F, Torre LA, Drope JM, Ward EM, Jemal A (2017) Global cancer in women: Cancer control priorities. Cancer Epidemiol Biomarkers Prev 26(4): 458-470.
- Sumit Punj, Yassmine Akkari, Jennifer Huang, Fei Yang, Allison Creason, et al. (2018) Preconception Carrier Screening by Genome Sequencing: Results from the Clinical Laboratory. Am J Hum Genet 102(6):1078-1089.
- Gargallo P, Segura V, Yáñez Y, Balaguer J, Cañete A (2019) Li-Fraumeni: Will the detection in families increase the survival of its members? An Pediatr 90(1): 54-55.
- Peterson B, Gordon C, Boehm JK, Inhorn MC, Patrizio P (2018) Initiating patient discussions about oocyte cryopreservation: Attitudes of obstetrics and gynaecology resident physicians. Reprod Biomed Soc Online 6: 72-79.
- Di Silvestro P, Alvarez Secord A (2018) Maintenance treatment of recurrent ovarian cancer: Is it ready for prime time? Cancer Treat Rev 69(January): 53-65.
- G Cicero, R De Luca, P Dorangricchia, G Lo Coco, C Guarnaccia, et al. (2017) Risk Perception and Psychological Distress in Genetic Counselling for Hereditary Breast and/or Ovarian Cancer. J Genet Couns 26(5): 999-1007.
- Bolejko A, Hagell P, Wann-Hansson C, Zackrisson S (2015) Prevalence, long-term development, and predictors of psychosocial consequences of false-positive mammography among women attending population-based screening. Cancer Epidemiol Biomarkers Prev 24(9): 1388-1397.
- Grimmett C, Pickett K, Shepherd J (2018) Systematic review of the empirical investigation of resources to support decision-making regarding BRCA1 and BRCA2 genetic testing in women with breast cancer. Patient Educ Couns 101(5): 779-788.
- Braithwaite D, Emery J, Walter F, Prevost AT, Sutton S (2006) Psychological impact of genetic counseling for familial cancer: A systematic review and meta-analysis. Fam Cancer 5(1): 61-75.
- Mohandas K Mallath, David G Taylor, Rajendra A Badwe, Goura K Rath, V Shanta, et al. (2014) The growing burden of cancer in India: Epidemiology and social context. Lancet Oncol 15(6): e205-e212.
- Karki K, Singh KP, Kumar U, Mohan M (2014) Cancer Scenario with Future Perspectives in Uttarakhand Region of India. Glob J Res Anal 3(12): 1-3.
- Initiative B, Collaborators C (2018) Articles The burden of cancers and their variations across the states of India : the Global Burden of Disease Study 1990- 2016 : 5-20.
- Torre LA, Islami F, Siegel RL, Ward EM, Jemal A (2017) Global cancer in women: Burden and trends. Cancer Epidemiol Biomarkers Prev 26(4): 444-457.
- M Arora, C Mathur, T Rawal, S Bassi, R Lakshmy, et al. (2018) Socioeconomic differences in prevalence of biochemical, physiological, and metabolic risk factors for non-communicable diseases among urban youth in Delhi, India. Prev Med Reports 12(47): 33-39.
- Christina Bradshaw, Noble Gracious, Ranjit Narayanan, Sajith Narayanan, Mohammed Safeer, et al. (2019) Paying for Hemodialysis in Kerala, India: A Description of Household Financial Hardship in the Context of Medical Subsidy. Kidney Int Reports: 390-398.
- Horton R (2018) Offline: The new politics of health in India. Lancet 392(10151): 902.
- Moradhvaj, Saikia N (2019) Gender Disparities in Health-care Expenditure (HCE) and Financing Strategies (HCFS) for In-patient Care in India. SSM - Popul Heal: 100372.
- Sudha Sundar, Poonam Khetrapal-Singh, Jon Frampton, Edward Trimble, Preetha Rajaraman, et al. (2018) Harnessing genomics to improve outcomes for women with cancer in India: key priorities for research. Lancet Oncol 19(2): e102-e112.
- Gordon C, Carmichael JC, Tewari KS (2018) Oncofertility in the setting of advanced cervical cancer - A case report. Gynecol Oncol Reports 24(December 2017): 27-29.
- MaryAnn Abacan, Lamia Alsubaie, Kristine Barlow-Stewart, Beppy Caanen, Christophe Cordier, et al. (2018) The Global State of the Genetic Counseling Profession. Eur J Hum Genet 27(2):183-197.
- Christos Nikolaidis, Debra Duquette, Kari E Mendelsohn-Victor, Beth Anderson, Glenn Copeland, et al. (2018) Disparities in genetic services utilization in a random sample of young breast cancer survivors. Genet Med.
- Miller AB (2009) Cervical cancer in rural India. Nat Rev Clin Oncol 6:384.
- Simone M Rowley, Lyon Mascarenhas, Lisa Devereux, Na Li, Kaushalya C Amarasinghe, et al. (2018) Population-based genetic testing of asymptomatic women for breast and ovarian cancer susceptibility. Genet Med.
- Domchek SM (2015) Evolution of genetic testing for inherited susceptibility to breast cancer. J Clin Oncol 33(4): 295-296.
- Gillard S, Spain D, Sin J, Chen T, Henderson C, et al. (2018) eHealth interventions for family carers of people with long term illness: A promising approach? Clin Psychol Rev 60(March 2017): 109-125.
- Dainis AM, Ashley EA (2018) Cardiovascular Precision Medicine in the Genomics Era. JACC Basic to Transl Sci 3(2): 313-326.
- Li D (2018) Recent advances in colorectal cancer screening. Chronic Dis Transl Med 4(3): 139-147.
