 Research Article
Research ArticleABSTRACT
Problem Statement: Cryotherapy is widely used for the treatment of acute soft tissue lesion, however, its results are directly associated with the technique used.
Approach: To establish differences between the application of cryotherapy techniques on the ankle joint.
Purpose: This is a randomized clinical trial. Twenty young and physically active participants (10 men and 10 women) participated in the study. The analysis of superficial skin temperature (SST) of the anterior, lateral, and posterior regions of the ankle, agility performance, and dynamic balance after the application of cold water immersion (CWI), cryotherapy+Game Ready® compression (CGRC), or ice pack (IP) was performed. Rewarming and agility and balance performance were analyzed up to 30 minutes after interventions.
Results: The CWI demonstrated lower SST (p<0.01) for all regions of the ankle; followed by the CGRC and IP. The CWI and CGRC provided better cooling up to 30 minutes (p<0.01) in the anterior region of the ankle. The CWI and CGRC groups showed greater cooling of the posterior region of the ankle up to 10 minutes (p=0.02). The CWI group performed worst in agility. No changes were observed in dynamic balance.
Conclusions: The CWI and CGRC groups performed better in decreasing SST in all regions of the ankle. The CWI group demonstrated reduced agility performance. Dynamic balance was not altered. These results may contribute to the choice of the best cryotherapy technique, to be used in clinical practice as recovery after exercise or for treatment of acute injuries.
Keywords: Cryotherapy; Cold Water Immersion; Cutaneous Temperature; Agility; Balance; Physiotherapy Modalities
Abbreviations: CWI: Cold Water Immersion; SST: Superficial Skin Temperature; IP: Ice Pack; CGRC: Cryotherapy+Game Ready® Compression
Introduction
Cryotherapy is widely used for the treatment of acute soft tissue [1] to reduced pain, slow edema formation, decreased tissue temperature and cell permeability, induced superficial vasoconstriction, and prevention of secondary hypoxic injury [2,3]. However, its results are directly associated with the technique used, application time, decrease in skin temperature, and depth of cold penetration [4]. Among the cryotherapy techniques the ice pack is a low-cost device which is easily accessible, causing a reduction in tissue temperature and physiological changes to at least one centimeter [5,6], the cold water immersion (CWI) allows a greater body area to be exposed to cold [7], maintaining tissue cooling for longer and providing increased analgesia [8] and cryotherapy with intermittent compression can deliver similar results [9,10]. The literature shows that cryotherapy with intermittent compression is widely used for recovery of ligament injuries [11], total knee arthroplasty [12] and reduction in post-operative pain [10].
This form of application is effective in reducing pain [10,13,14], improving tissue oxygenation and microcirculation, and providing faster recovery from ligament disorders [15]. In addition, Murgier at. al. Murgier, et al. [11] reported that pneumatic compression and cryotherapy may reduce pain and postoperative blood loss, and lead to higher functional scores [12]. On the other hand, cryotherapy and intermittent compression equipment are more expensive and less accessible for health professionals. Several studies have aimed to evaluate the differences between the application of cryotherapy techniques, with divergent methods and contradictory results [10,16,17]. In addition, Hawkins and Hawkins [18] reported that sports physical therapists applied cryotherapy with great variability for acute or sub-acute ankle sprain and that efforts need to be made to substantiate the evidence of cryotherapy application [19].
Thus, little is known about the differences between the applications of an ice pack, cold water immersion, and cryotherapy associated with intermittent compression for the purpose of reducing skin surface temperature (related to treatment efficacy) and changing agility and balance. Therefore, new research should include controlled and reproducible different techniques. To contribute to discussions on the effects and indications of different techniques of cryotherapy on the ankle joint, the present study aimed to establish differences between applications of cryotherapy techniques on the ankle superficial skin temperature (SST) in different regions of this joint; the effects on agility and dynamic balance were also evaluated. We hypothesized that the three cryotherapy techniques studied would have the same effects on decreasing skin temperature, agility and balance. In addition, we hypothesized that the anterior, posterior, and lateral regions of the ankle would present different values of cooling. Thus, the results may support clinical decision making and aid choices made according to preference among the techniques.
Methods
This was a randomized clinical study, approved by the Research Ethics Committee of the institution (case N. 2.117.378) and registered at www.clinicaltrials.gov (ID NCT03659474). All procedures were performed at the physiotherapy outpatient clinic of the University. Twenty young and physically active subjects (ten men and ten women), without injuries or complaints in the ankle participated in the study. The women’s evaluations were carried out outside the menstrual period, since when they are menstruating, worsening in agility and dynamic balance can occur [20]. The sample size was calculated based on the results of the manuscript “The Magnitude of Tissue Cooling during Cryotherapy with Varied Types of Compression” [21], considering the SST over the mid-portion of the right gastrocnemius belly in twenty minutes after application of ice only and the elastic wrap. The values used were the means of each group (15.51 and 11.01) with a standard deviation of 4.39 (p <0.05). The program used was the Power and Sample Size, with a 95% confidence interval, 5% alpha level, and test power of 90%. Thus, 20 participants were recruited.
All participants underwent cryotherapy for the ankle with three different applications: cold water immersion (CWI), cryotherapy+Game Ready® compression (CGRC), or icepack (IP). Entries were randomly performed by a researcher not involved in the study through the platform www.ramdom.org and recorded in three different periods, with a 48-hour interval between measurements (Figure 1). All participants performed the three interventions, and there was no sample loss. Initially, a pre-intervention evaluation was performed where the SSTs of the anterior, lateral, and posterior regions of the ankle were collected with a professional Flir C2® thermal camera (FLIR® systems, Inc. Washington, USA). The thermographic camera had automatic ZOOM, it was positioned perpendicularly to the ankle, with a distance of 30 centimeters from the anterior joint line of the ankle, lateral malleolus and midpoint of the calcaneus tendon. In sequence, the Y test and Side Hop Test (SHT) were developed, already used in previous studies for the analysis of dynamic balance (22,23) and agility (24), respectively. Participants were familiarized with the tests prior to conducting the data collection.
After the baseline assessment, the participants performed a warm-up with a 15-minute walk on the treadmill (Movement®) at a constant and comfortable pace. Immediately after walking, subjects were referred to one of three cryotherapy techniques for testing. For the CWI group, the ankle joint was immersed in cold water up to the mid portion of the tibia, at approximately 4°C [22], controlled by the thermal camera. For the CGRC group, the ankle joint was wrapped (cold wrap) using maximum dynamic intermittent compression (established by the equipment) and programmed to maintain a temperature of 1°C, according to the manufacturer’s instructions. For the IP group, the ankle joint was wrapped with three ice packs, each containing 500g of crushed ice. All treatments were performed for 20 minutes. The ambient temperature was always between 25 and 27 degrees Celsius. During cryotherapy applications, the participants sat on a comfortable chair, with their knee and ankle at 90º (Figure 2).
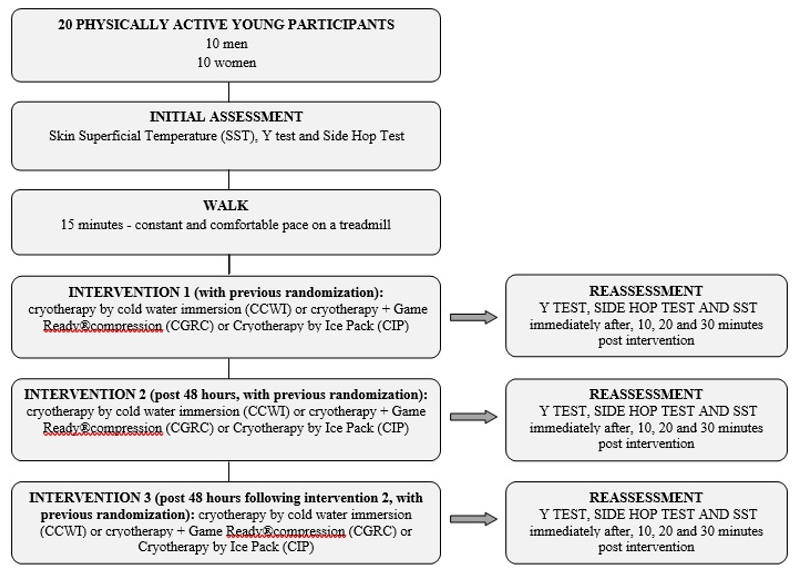
Figure 1: Flow chart depicting methodology for the assessments and interventions using cryotherapy.
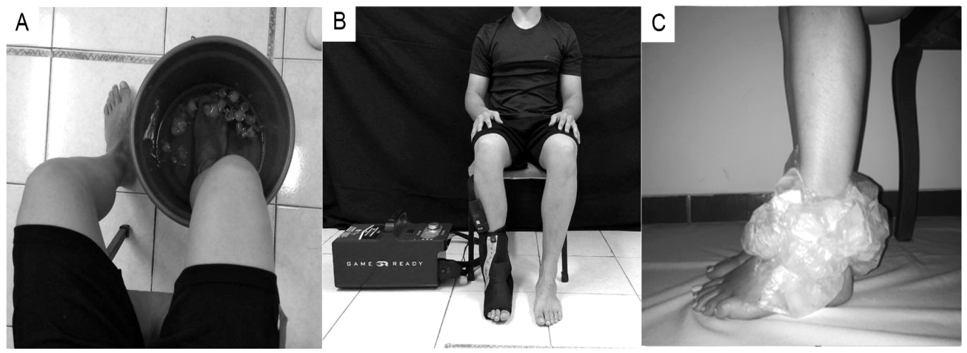
Figure 2: Cryotherapy techniques.
A. cryotherapy using cold water immersion
B. cryotherapy + Game Ready® compression; and
C. cryotherapy using an ice pack.
The same position was adopted for the three interventions to reduce the effects of the peripheral blood flow on the cooling and rewarming of the skin. The SST assessment was performed immediately after, 10 minutes, 20 minutes, and 30 minutes after the cryotherapy techniques. The same procedure was carried out for the functional tests. The participants attended data collection on three distinct days and were randomized into one of the three interventional groups each day. Statistical analysis was performed using SPSS software version 2.2 (SPSS Inc. Chicago, Ill, USA). The level of significance was set at 5%. The Shapiro Wilk test was used to establish the normality of the data. The values obtained were compared using a two-way repeated measure ANOVA, one-way ANOVA, and the Bonferroni post-test. To verify the effect size (d), the following formula was used: d= (x1−x2)/averages of the standard deviations (SDs), where x1 is the average of the analyzed variable in the initial assessment, and x2 is the average of the analyzed variable in the final assessment [23]. The average of the SDs was calculated through the arithmetic mean of the standard deviations related to the initial and final assessments: (SD1+ SD2)/2. The effect size was defined as ≤ 0.5 representing a small effect, between >0.5 and ≤ 0.8, a medium effect, and > 0.8, a large effect [23].
Results
Twenty physically active subjects (10 men and 10 women) with a mean age of 21.4±1.9 years, weight of 70.7±12.4kg, and height of 1.7±0.07 meters participated in this study. The subjects engaged in physical activities (gym, soccer, running and other exercises) three to five times a week and were present at the three different data collection moments; there were no sample losses. The three cryotherapy application techniques significantly decreased the SST in the anterior, lateral, and posterior regions of the ankle when the time periods (baseline, immediately post, post10, 20, and 30 minutes) were compared. However, the IP group showed no significant difference for cooling of the anterior region of the ankle 30 minutes after application. In addition, only the CWI group (anterior, lateral, and posterior region of the ankle) and the CGRC group(posterior region of the ankle) exhibited SST sunder 15ºC (Table 1), related to analgesic effects [24]. The comparisons between the three application techniques showed that the CWI induced lower SST values for the anterior and lateral regions of the ankle at up to 10 minutes after application.
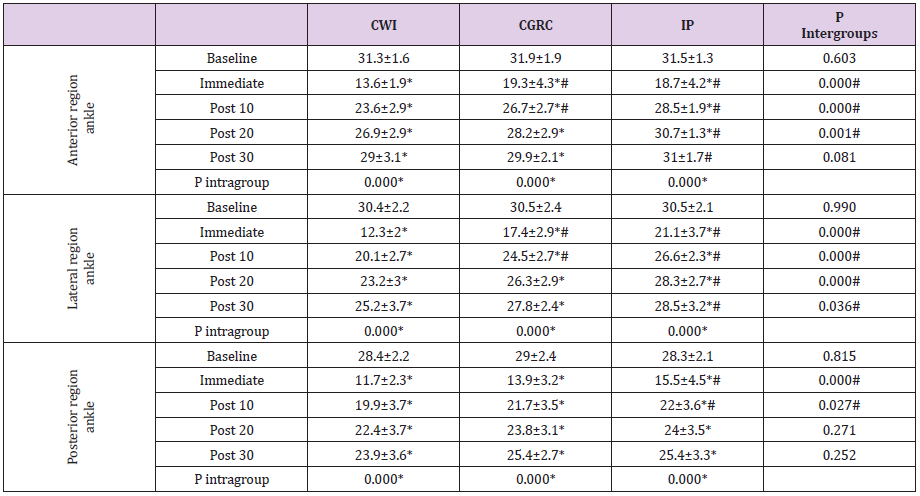
Table 1: Assessment of the SST for the anterior, lateral, and posterior regions of the ankle after the application of different cryotherapy techniques.
Note: SSP: superficial skin temperature. CWI: cold water immersion. CGRC: cryotherapy + Game Ready® compression. IP: Icepack. *Significant difference between baseline and rewarming time using the same cryotherapy technique established by repeated measures ANOVA. #Results established by one-way ANOVA for comparison between groups using CWI at different moments.
Both the CWI and CGRC applied to the posterior region of the ankle were equally effective in reducing SST at 10 minutes after the intervention. However, application of CWI produced the lowest temperature in the evaluated regions, except in the posterior region immediately after the ankle was removed from immersion (Table 1). Analysis of the effect size for SST of the anterior ankle demonstrated larger effect sizes for CWI (d = 0.90) and CGRC (d = 0.80), and a smaller effect (d = 0.20) for IP 30-minutes after application. For the lateral and posterior regions of the ankle all the application techniques demonstrated large effects (d > 0.8) for the reduction in SST at up to 30-minutes post-application. Functional performance based on the SHT indicated that the subjects in the CWI group performed worse immediately after application, with a significantly increased time. The subjects in the CGRC group showed improvement 30-minutesafter application, which was not expected. However, no performance differences were identified in the IP group (Table 2).
In addition, subjects in the IP group, even with no performance differences in the SHT at different moments, obtained better results when compared to the CWI group. For the Y test, no significant differences were identified at any moments or between the techniques used (Table 2). For the effect size produced by the different cryotherapy techniques, the CGRC group presented a large effect (d = 0.8) between the initial assessment and after 30 minutes, with improvement in agility performance (SHT). The CWI group demonstrated a large and negative effect (d = 1) between the baseline and immediately after assessments, with worse functional performance in the same test. The results obtained in the present study demonstrated significant differences between the techniques for the reduction in SST as well as changes in agility performance of the participants.
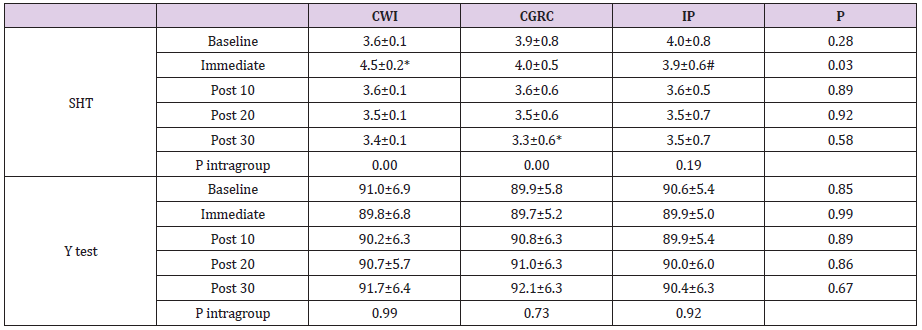
Table 2: Functional performance in the SHT and Y tests after applying different cryotherapy techniques.
Note: SHT: Side Hop Test. CWI: cold water immersion. CGRC: cryotherapy + Game Ready® compression. IP: Ice pack. *Significant difference between application times using the same cryotherapy technique established by repeated measures ANOVA. #Results established by one-way ANOVA for comparison between groups using CWI.
Discussion
The present study showed the cooling of the anterior, lateral and posterior ankle regions, and the posterior region of the ankle showed the lowest skin surface temperature (SST). All the cryotherapy techniques analyzed significantly decreased the SST; however, local cold water immersion (CWI) was better at decreasing SST when compared to cryotherapy + Game Ready® compression (CGRC) and ice pack (IP), up to 10 minutes after the end of the applications, in all regions. The importance of analyzing SST in different regions is justified by the different sites of injury in this joint (direct trauma, ligament injuries, Achilles tendon ruptures, inflammation of burses, etc.), which may respond unequally to the application of cold. The results revealed that the three techniques of cryotherapy applications significantly decreased the SST for up to 30-minutes of rewarming. The CWI group exhibited lower SST values in the anterior and lateral regions of the ankle (approximately 15 degrees immediately after application and better values at up to 10-minutes of rewarming), which is related to a local analgesic effect through inhibiting nerve conduction velocity [25].
However, 20-minutes after application in the anterior and lateral regions of the ankle, the subjects in the CWI and CGRC groups performed better than those in the IP group, which always exhibited higher SST values. These results contradict those by Kennet, Hardaker, Hobbs, & Selfe [26] and Hawkins, Shurtz, & Spears [9] who found lower temperatures after applying a ice pack compared to compression therapy. It is believed that greater rewarming after ice pack application may have occurred due to the lack of compression and worse contact between the skin and ice [21]. The cooling of the posterior region of the ankle demonstrated lower temperatures in all the techniques used, which may be justified by the decreased blood circulation of the Achilles tendon and bursa located in the posterior region of the ankle, since the connective tissue under the skin has less blood flow than the muscles, which does not favor the reheating of this place. It is worth noting that even after 10 minutes the CWI and CGRC groups presented better cooling results.
The best results associated with CWI application can be explained by the greater cooling area of contact [7], the hydrostatic pressure that redirected the skin blood flow to the central circulation [27], and the local vasoconstriction that reduces the fluid flux into the interstitial space. The intervention with CGRC provided satisfactory results that may be related to cooling associated with compression [12]. The results achieved for the effects of cryotherapy on agility performance, evaluated by SHT, confirmed the findings of previous studies, such as those reported by Macedo, et al. [22] and Furmanek, Słomka, & Juras [28] who showed worse functional performance immediately after CWI application. It has commonly been assumed that reduction in nerve conduction velocity may reduce the sensitivity of the afferent mechanoreceptors and the sensitivity of the muscle spindles with less afferent sensory information, causing damage to both the neuromuscular control and functional performance [4,25,29].
Moreover, Kilby, Molenaar, & Newell [30] and Oba, et al. [31] highlighted that the ankle joint capsule is more superficial than the majority of joints, and therefore, the receptors may be more influenced by cryotherapy application. However, after 10-minutes rewarming following CWI and at all intervention moments after CGRC and IP application, the agility performance returned to baseline values, which should be considered for the planning of physical and functional activities, training,and even for the return to sport after cryotherapy. These findings agree with those of Williams, Miller, Sebastianelli, & Vairo Williams, et al. [32] who reported that a 15-minute application of crushed ice on the ankle was not able to change the function of joint receptors. Finally, the Y test did not demonstrate any change after the application of the cryotherapy techniques, which may have occurred because this is a simple and easy test for young and healthy individuals, such as the participants of this study. Thus, we can infer that CWI was the best technique to reduce SST, followed by CGRC, and the IP provided the worst cooling.
This finding is important for clinical practice, since CWI application is widely used, low cost, and produced better results for the variables analyzed. For the posterior region of the ankle, CWI and CGRC were similar in cooling, and even at high cost the CGRC is an appropriate choice and can be used according to the preference of the physiotherapist or the patient. In addition, 10 minutes after the application of CWI, agility is worse and greater care must be taken. As limitations of this study it should be pointed out that healthy individuals were evaluated, intramuscular temperature analysis would be more reliable regarding the application of these techniques, and a force platform would be more appropriate to evaluate balance. Further research should complement the results obtained in this study.
Conclusion
The present study concluded that there is a difference in the application of the three cryotherapy techniques. The applications of CWI and CGRC were more effective in cooling and maintaining lower SST of the ankle. These two modalities should be the preferred treatment options for the anterior, lateral, and posterior regions of the ankle. CWI reduced agility performance at up to 10 minutes after cooling. Dynamic balance was not altered by any of the cryotherapy techniques tested. Ethics Committee of the State University of Londrina (UEL), Londrina, Paraná (Opinion No. 2.117.378). Clinical Trials (NCT03659474).
Conflict of Interest
None.
Abstract published in Physical Therapy in Sport 31 (2018) e2, as
an award-winning paper at the VI INTERNATIONAL CONGRESS OF
THE NATIONAL SOCIETY OF SPORTS PHYSIOTHERAPY (SONAFE)
- Brazil.
Acknowledgement
• Brazilian National Council for Scientific and Technological
Development (CNPQ)
• Coordination for the Improvement of Higher Education
Personnel (CAPES).
Funding Statement
No funding.
References
- Lin S, Xie J, Yao X, Dai Z, Wu W (2018) The Use of Cryotherapy for the Prevention of Wound Complications in the Treatment of Calcaneal Fractures. The Journal of Foot and Ankle Surgery 57(3): 436-439.
- Gillette CM, Merrick MA (2018) The Effect of Elevation on Intramuscular Tissue Temperatures. Journal of Sport Rehabilitation 27(6): 526-529.
- Ostrowski J, Purchio A, Beck M, Leisinger J, Tucker M, et al. (2018) Examination of Intramuscular and Skin Temperature Decreases Produced by the Power Play Intermittent Compression Cryotherapy. Journal of Sport Rehabilitation 27(3): 244-248.
- Houten D, Cooper D (2017) How does cryotherapy effect ankle proprioception in healthy individuals? Somatosensory and Motor Research 34(3): 158-171.
- Herrera E, Sandoval MC, Camargo DM, Salvini TF (2010) Motor and Sensory Nerve Conduction Are Affected Differently by Ice Pack, Ice Massage, and Cold Water Immersion. Physical Therapy 90(4): 581-591.
- Hunter EJ, Ostrowski J, Donahue M, Crowley C, Herzog V (2016) Effect of salted ice bags on surface and intramuscular tissue cooling and rewarming rates. Journal of Sport Rehabilitation 25(1): 70-76.
- Santos VB da C, Cardoso, C dos S, Figueiredo CP, Macedo, C de S G (2015) Effect of cryotherapy on the ankle temperature in athletes: ice pack and cold water immersion Fisioterapia Em Movimento 28(1): 23-30.
- Love HN, Pritchard KA, Hart JM, Saliba SA (2013) Cryotherapy Effects, Part 1: Comparison of Skin Temperatures and Patient-Reported Sensations for Different Modes of Administration. International Journal of Athletic Therapy and Training 18(5): 22-30.
- Hawkins J, Shurtz J, Spears C (2012a) Traditional Cryotherapy Treatments are More Effective than Game Ready® on Medium Setting at Decreasing Sinus Tarsi Tissue Temperatures in Uninjured Subjects. Journal of Athletic Enhancement 1(2): 2-6.
- Kraeutler MJ, Reynolds KA, Long C, McCarty EC (2015) Compressive cryotherapy versus ice-a prospective, randomized study on postoperative pain in patients undergoing arthroscopic rotator cuff repair or subacromial decompression. Journal of Shoulder and Elbow Surgery 24(6): 854-859.
- Murgier J, Cassard X (2014b) Cryotherapy with dynamic intermittent compression for analgesia after anterior cruciate ligament reconstruction Preliminary study. Orthopaedics & Traumatology: Surgery & Research 100(3): 309-312.
- Murgier J, Cailliez J, Wargny M, Chiron P, Cavaignac E, et al. (2017) Cryotherapy With Dynamic Intermittent Compression Improves Recovery From Revision Total Knee Arthroplasty. Journal of Arthroplasty 32(9): 2788-2791.
- Alfuth M, Strietzel M, Vogler T, Rosenbaum D, Liem D (2016) Cold versus cold compression therapy after shoulder arthroscopy: a prospective randomized clinical trial. Knee Surgery, Sports Traumatology, Arthroscopy 24(7): 2209-2215.
- Song M, Sun X, Tian X, Zhang X, Shi T, et al. (2016) Compressive cryotherapy versus cryotherapy alone in patients undergoing knee surgery: a meta-analysis. Springer Plus 5(1):
- Murgier J, Cassard X (2014a) Cryotherapy with dynamic intermittent compression for analgesia after anterior cruciate ligament reconstruction Preliminary study Orthopaedics and Traumatology: Surgery and Research 100(3): 309-312.
- Holwerda SW, Trowbridge CA, Womochel KS, Keller DM (2013) Effects of Cold Modality Application With Static and Intermittent Pneumatic Compression on Tissue Temperature and Systemic Cardiovascular Responses. Sports Health: A Multidisciplinary Approach 5(1): 27-33.
- Tomchuk D, Rubley MD, Holcomb WR, Guadagnoli M, Tarno JM (2010b) The Magnitude of Tissue Cooling During Cryotherapy With Varied Types of Compression. Journal of Athletic Training 45(3): 230-237.
- Hawkins J, Shurtz J, Spears C (2012b) Traditional Cryotherapy Treatments are More Effective than Game Ready® on Medium Setting at Decreasing Sinus Tarsi Tissue Temperatures in Uninjured Subjects. Journal of Athletic Enhancement 1(2): 2-6.
- Hawkins SW, Hawkins JR (2016) CLINICAL APPLICATIONS OF CRYOTHERAPY AMONG SPORTS PHYSICAL THERAPISTS. International Journal of Sports Physical Therapy 11(1): 141-148.
- Kami AT, Vidigal CB, Macedo C de SG (2017) Influência das fases do ciclo menstrual no desempenho funcional de mulheres jovens e saudá Fisioterapia e Pesquisa 24(4): 356-362.
- Tomchuk D, Rubley MD, Holcomb WR, Guadagnoli M, Tarno JM (2010a) The magnitude of tissue cooling during cryotherapy with varied types of compression Journal of Athletic Training 45(3): 230-237.
- Macedo C eS, Vicente RC, Cesário MD, Guirro RR (2015) Cold-water immersion alters muscle recruitment and balance of basketball players during vertical jump landing. Journal of Sports Sciences 34(4): 348-357.
- Cohen J (1990) Statistical power analysis for the behavioral sciences.
- STARKEY C (2001) Therapeutic resources in physical therapy.
- Algafly AA, George KP, Herrington L (2007) The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. British Journal of Sports Medicine 41(6): 365-369.
- Kennet J, Hardaker N, Hobbs S, Selfe J (2007) Cooling efficiency of 4 common cryotherapeutic agents. Journal of Athletic Training 42(3): 343-348.
- Murray A, Cardinale M (2015) Cold applications for recovery in adolescent athletes: a systematic review and meta analysis. Extrem Physiol Med 4: 17.
- Furmanek MP, Słomka K, Juras G (2014) The effects of cryotherapy on proprioception system. BioMed Research International 2014: 696397.
- Costello JT, Culligan K, Selfe J, Donnelly AE (2012) Muscle, Skin and Core Temperature after -110°C Cold Air and 8°C Water Treatment. PLoS ONE 7(11): e48190.
- Kilby MC, Molenaar PCM, Newell KM (2015) Models of postural control: Shared variance in joint and COM motions. PLoS ONE 10(5): 1-20.
- Oba N, Sasagawa S, Yamamoto A, Nakazawa K (2015) Difference in postural control during quiet standing between young children and adults: Assessment with center of mass acceleration. PLoS ONE 10(10): 1-11.
- Williams EE, Miller SJ, Sebastianelli WJ, Vairo GL (2013) Comparative immediate functional outcomes among cryotherapeutic interventions at the ankle. Int J Sports Phys Ther 8(6): 828-837.
