 Case Report
Case ReportABSTRACT
Introduction: Intramural pregnancy (IMP) is a rare type of ectopic pregnancy. At present, the role of serum β-hCG and imaging, including transvaginal ultrasound (TVS) and magnetic resonance (MR) imaging in monitoring IMP has not been elaborated.
Case Presentation: We present a case of a 34-year-old female patient whose serum β-hCG level had a steady decline later without intervention, however, the lesion in TVS keep growing. A 40mm diameter mass was detected by TVS and 3-D MR reconstructions confirmed the diagnosis of intramural pregnancy. Local mass resection by laparoscopy was performed and postoperative histopathology also confirmed it.
Discussion/Conclusion: Our observation nicely illustrates serum β-hCG level should combined with image for suspected intramural pregnancy monitoring.
Keywords: Intramural Pregnancy; Serum β-hCG; Imaging; Monitoring
Abbreviations: IMP: Intramural Pregnancy; TVS: Transvaginal Ultrasound; MR: Magnetic Resonance; HCG: β-Human Chorionic Gonadotropin; GTN: Gestational Trophoblastic Neoplasia
Introduction
Intramural pregnancy (IMP) is a rare type of ectopic pregnancy and described as a pregnancy that is partially or completely located within the myometrium of the uterine wall without communication with the endometrial cavity [1]. The cause of IMP remains unclear, endometrial, and uterine serosa damage or defect [2], adenomyosis and in vitro fertilization [3] are considered to increase the risk of IMP. The clinical symptoms are a history of amenorrhea with high serum β-human chorionic gonadotropin (HCG) levels, abdominal pain, irregular bleeding of the vagina, even the rupture of the uterus led to hemorrhagic shock [2-3]. However, the clinic typical are non-specificity in the early, similar to early pregnancy, other types of ectopic pregnancy and gestational trophoblastic neoplasia (GTN), resulting in difficult to diagnose. Serum β-hCG and imaging, transvaginal ultrasound (TVS) and magnetic resonance (MR) imaging, have been used for diagnosis of IMP recent years, however, their role in monitoring IMP has not been elaborated. Herein, we report a patient whose serum β-hCG level had a steady decline later without intervention, however, the lesion in TVS keep growing.
Case Report/Presentation
A 34-year-old female patient (G5P2), who had a history of induced abortion 14 days ago, was with prolonged vaginal bleeding underwent TVS and pregnancy test, and the result showed that a 12mm lesion was within the myometrium (Figure 1(A1)), and the serum β-hCG was positive (5203 mIU/ml) (Figure 1E). And then her serum β-hCG level had a steady decline later without intervention (Figure 1E), however, the lesion keeps growing (Figures 1(A1-D1) & 1F) with the enhancement of color Doppler signals (Figures 1(A2-D2)). One week later, her serum β-hCG level was 3299 mIU/ mL (Figure 1E) while the lesion embedded into the myometrium in the right-side wall of the uterine increased to 24 mm (Figure 1(B1)). Then a 40mm diameter mass was detected by TVS after 28 days (Figures 2A & 2B), and 3-D MR reconstructions confirmed the diagnosis of intramural pregnancy (Figure 2C). Thereafter, the patient was admitted to hospital, local mass resection by laparoscopy was performed. Intraoperative freezing showed spindle cell tumor, and postoperative histopathology confirmed it. Her β-hCG decreased to 50.4 mIU/mL 10 days after surgery with no vaginal bleeding and returned to normal 2 months after surgery (Figure 1G).
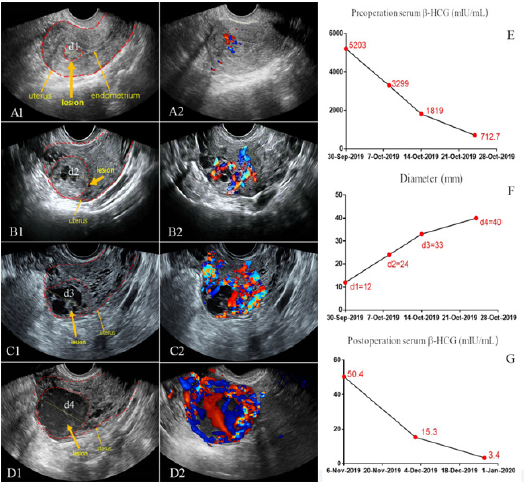
Figure 1: Image and serum β-hCG change for suspected intramural pregnancy monitoring
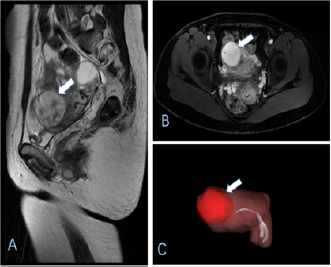
Figure 2: MR image and 3-D MR reconstructions for 40mm diameter mass in uterine.
Discussion/Conclusion
IMP accounting for less than 1% of all ectopic pregnancies [4],
which is increased significantly in recent years. The main symptoms
of IMP are menopause, mild vaginal bleeding, abdominal pain and
increasing of serum β-hCG [5], however, they are seldom specific
in early, which make IMP is too difficult to diagnose. Numerous
patients are not diagnosed IMP until uterine rupture [6]. Thus, early
diagnosis and monitoring are the key to prevent complications.
Nowadays, TVS is considered as the first-line imaging technique
for diagnosis of ectopic pregnancy, however, the data to monitor
intramural pregnancy is absent [7]. MR imaging has been reported
be useful in the early diagnosis of IMP [8] by providing a clear
definition of the relationship between the identified lesion and the
endometrial cavity, however, imaging features are very similar to
GTN, resulting in especially challenging in diagnosis. The treatment
for patients with IMP should be individualized, depending on the
size of the lesion, patient status and the desire for future fertility.
At present, the major treatment is surgery and medical therapy.
Firstly, surgery for IMP include mass resection by laparoscopy or
hysterectomy by laparoscopy or open surgery [4]. In our case, we
found a lesion was within the myometrium 14 days after induced
abortion. Besides, the diameter of lesion increased with time, thus
mass resection by laparoscopy was performed. Secondly, verghese,
et al. [9] reported the successful management of IMP with systemic
methotrexate administration. A number of patients reached
clinically cured by methotrexate.
Besides, a few treatments using UAE in the literature also
has been reported [10]. LONG, et al. reported the successful
management of an intramural pregnancy in the second trimester
with individualized and combined [11]. In summary, our
observation nicely illustrates serum β-hCG level should combined
with image for suspected intramural pregnancy monitoring. Early
diagnosis of intramural pregnancy is often difficult, and image
change may help to make an accurate diagnosis.
Statement of Ethics
The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Acknowledgement
The authors want to thank Shun-ping Shen for his contribution in editing (Figure 2).
Disclosure Statement
The authors have no conflicts of interest relevant to this article.
Funding Sources
This work was supported by the Bureau of Science and Technology Nanchong City Program (No. 18YFZJ0012). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Contributions
FXT: Planning, Data collection, analyzing and writing the manuscript. DL: Data collection, planning, data collection. ZPZ: Analyzing and writing the manuscript. HQH: Planning, data collection. FX: Conception, planning, data collection and revising the manuscript. YT: Conception, planning, data collection and revising the manuscript. All authors have read and approved the manuscript.
References
- Su S, Chavan D, Song K, Chi D, Zhang GY, et al. (2017) Distinguishing between intramural pregnancy and choriocarcinoma: A casereport. Oncol Lett 13(4): 2129-2132.
- Vlahos NF, Theodoridis TD, Partsinevelos GA (2017) Myomas and Adenomyosis: Impact on Reproductive Outcome. Biomed Res Int 2017: 5926470.
- Kurian NK, Modi D (2019) Extracellular vesicle mediated embryo-endometrial cross talk during implantation and in pregnancy. J Assist Reprod Genet 36(2): 189-198.
- Zhang Q, Xing X, Liu S, Xie X, Liu X, et al. (2019) Intramural ectopic pregnancy following pelvic adhesion: case report and literature review. Arch Gynecol Obstet 300(6): 1507-1520.
- Bannon K, Fernandez C, Rojas D, Levine EM, Locher S (2013) Diagnosis and management of intramural ectopic pregnancy. J Minim Invasive Gynaecol 20: 697-700.
- You SH, Chen PC, Chueh HY, Huang KG, Wang HS, et al. (2019) Perforating Scar of Intrauterine Device with Subsequent Intramural Pregnancy and Uterine Rupture. J Minim Invasive Gynecol 26(4): 591-592.
- Yoshigi J, Yashiro N, Kinoshita T, O’uchi T, Kitagaki H (2006) Diagnosis of ectopic pregnancy with MRI: efficacy of T2*weighted imaging. Magn Reson Med Sci 5: 25-32.
- Ramkrishna J, Kan GR, Reidy KL, Ang WC, Palma Dias R (2018) Comparison of management regimens following ultrasound diagnosis of nontubal ectopic pregnancies: A retrospective cohort study. BJOG 125: 567-575.
- Verghese T, Wahba K, Shah A (2012) An interesting case of intramyometrial pregnancy. BMJ Case Rep 2012: bcr1120115187.
- Wang S, Dong Y, Meng X (2013) Intramura ectopic pregnancy: Treatment using uterine artery embolization. J Minim Invasive Gynecol 20(2): 241-243.
- Kong L, Mao N, Shi Y, Ma H, Xie H (2017) Diagnosis and management of intramural ectopic pregnancy in the second trimester—a case report. BJR Case Rep 3(4): 20160095.
