 Research Article
Research ArticleAbstract
Background: The epidemiological data of cancer cases provides vital scientific information to evaluate and estimate the burden of the disease in Libya.
Patient and Methods: A hospital-based registry of cancer was used to document the facts of 974 Libyan patients with different cancers, diagnosed at the National Cancer Institute, Misurata-Libya in the year of 2016. Results: Of the 974 cancer patients, 538 were females with a mean age of 53 years. The number of male cancer patients was 436 men, with an average age of 57.7 years. The data revealed that the most common types of cancer in women were breast (n = 222; 41.3%), colon (n = 69; 12.8%), lymphoma (n = 32; 5.9%), ovarian (n = 31; 5.8). %). and uterus (n = 27; 5%). On the other hand, the most common cancers in men were colon (n = 80; 18.3%), lung (n = 80; 18.3%), prostate (n = 55; 12.6%), lymphoma (n = 42; 9.6%), and leukemia (n = 22; 5%). Conclusion: To improve the cancer registry, it is necessary to have well-developed sources of epidemiological and clinical data in order to determine the cancer’s prevalence and assess any new instances. Second, data on cancer should be shared and used in Libya to enhance cancer management.Keywords: Cancer Incidence 2016; Breast Cancer; Colon Cancer; Epidemiology; National Cancer Institute-Misurata (NCIMisurata)
Introduction
Cancer is a collection of disorders defined by uncontrolled cell growth and spread. Cancer is becoming more common over the world as a result of an aging population and environmental conditions [1]. Cancer is becoming more prevalent in Africa as the population grows and develops, as well as the increased prevalence of risk factors associated with economic transition (such as smoking, alcohol, obesity, junk food, physical inactivity, and reproductive behaviors) and certain infectious agents that play a role in disease etiology [2]. According to the United Nations, Africa’s population is expected to grow from 1.03 billion to 1.63 billion between 2010 and 2030, with a growth rate of around 60%, and by 90% for those aged 60 and over, as the population in this age group is expected to grow from 55 million to 103 million, on the other hand, this is the age when most tumors occur [2]. The global burden of cancer continues to rise, owing mostly to population aging and expansion, as well as cumulative exposure to carcinogenic activities, particularly smoking, in economically developing countries. Despite the fact that cancer incidence in the developing world is around half that in the developed world, overall cancer mortality is often comparable [3,4].
Cancer survival is worse in underdeveloped nations, most likely due to a combination of late-stage detection and limited access to appropriate and standard health care [5]. Accurate data is required for proper strategic planning and strategy to scaling up health care services such as screening, prevention, early diagnosis, and treatment. As a result, cancer registries were established, which are used to determine the incidence and prevalence of cancer as a first step toward developing a national cancer prevention and treatment plan [6]. Because of a lack of cancer monitoring and screening methods, comprehensive studies in the field of cancer epidemiology are limited in developing nations. Due to the lack of a national cancer registry, the Libyan picture is further complicated by the lack of a defined system for capturing data and restricted monitoring for the formation of strategic plans for the health care program [7-9]. Libya was separated into five sections when the Ministry of Health began implementing a cancer registry program in 2007 (Figure1A).
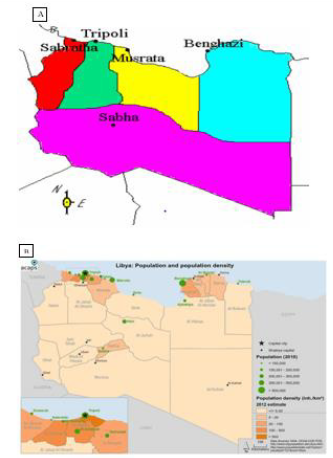
Figure 1: General map of Libya; A: the major regions of cancer registries. B: the Libya population density (2015).
The details of this registration software are shown in (Table 1). However, because the majority of these registers are still in their infancy and incomplete, Libya still lacks a population-based national cancer registry [7,8]. In Misurata, a hospital-based cancer registry was established in 2008, and the first report on hospital data from that year was published [10]. The analysis estimated the scope of the cancer problem in Libya’s central region, which has a population of more than a million people [1]. The current study’s goals are to assess some demographic data, cancer rates, and prevalence based on the hospital cancer registry at the National Cancer Institute- Misurata. The research could help to improve cancer control in the country as a whole. This is the first-time statistics on the prevalence of cancer in Libya’s central area has been published.
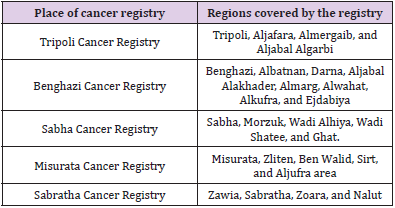
Table 1: Regions covered by Libyan cancer registry program.
Materials and Methods
Study Population
The clinical oncology services in most sections of central Libya are covered by the National Cancer Institute of Misurata (NCIMisurata). According to the Libyan incomplete census of 2012, there were 6, 278, 438 people in Libya, with 3,156, 745 men and 3,121, 693 women, and only 386,120 people living in Misurata city (Figure 1B) [11].
Ethical Approval
The study was approved by the Ethical Committee of the NCIMisurata. All personal identifiers were stripped from the data and only medically significant parameters were analyzed out.
Data collection
The data of cancer incidences was obtained from the patients’ records of the department of Medical Oncology at the NCI-Misurata/ Libya. All patients were diagnosed at the same institute during the period from January 1, 2016, to December 31, 2016.The patients were diagnosed through various procedures. The histopathological examinations and radiological diagnosis of cancer patients were included in this study; however, uncertain diagnosed cases are excluded. The collected data from the patients’ medical records included age, gender, city, and types of cancer. All cancer cases were coded using the International Classification of Diseases (ICD) [12]. Duplicate entry checking was done by comparing the data obtained from the department of pathology and laboratory for all cancer cases with that received from the clinical units of the hospital.
Statistical Analysis
Microsoft Excel 2007 was applied to drawn graphs and to evaluate relationships between variables.
Results and Discussion
A total of 974 cancer cases were recorded at the department of registry in the NCI-Misurata, during the year 2016. Among them 45 % (n= 436) were males and 55% (n=538) were females (Figures 2 & 3). The most common cancer (overall) was found to be breast cancer (23.2%, n 226), followed by colon cancer (15.2%, n = 149) and lung cancer (9.3 %, n = 91) (Figure 4). In North Africa, it was pragmatic that the overall cancer rate, e.g., age standardized on world population ranged in men from 94.0/100,000 to 162.9/100,000, and in women from 84.7 to 164.0/100,000. The most common cancers are comparable to those found in Europe, i.e., lung, breast, colon, and prostate but different from sub-Saharan Africa where infection-related cancers are the main common cancers [6,8]. The overall mean age of cancer patients at the onset of complaint (n = 974) was 55.15 ± 16.30 years, ranging from 1 to 99 years. For male patients, (n = 436), the mean age was found to be 57.76 ± 13.43 years, ranging from 1 to 92 years, while for female patients (n = 538), the mean age was 53.03 ± 15. 51 years, ranging from 17 to 99 years old. In this study we can clearly see that there are highest of cancers in females particularly at the age group of 41-50 years (see table 2).
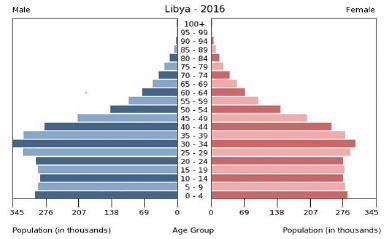
Figure 2: Pyramid pattern of the Libyan resident population (2016) according to age and sex [11].
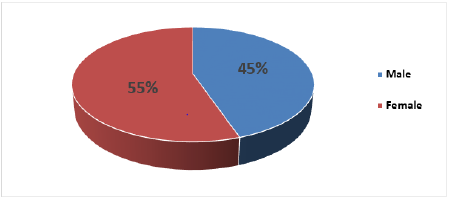
Figure 3: Distribution of cancers in NCI-Misurata 2016 (n=974) according to the gender of patient.
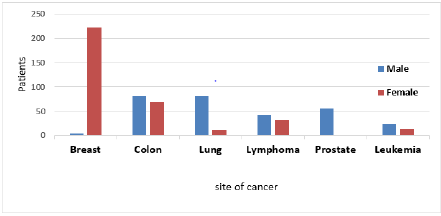
Figure 4: The most common types of cancers in NCI-Misurata 2016.
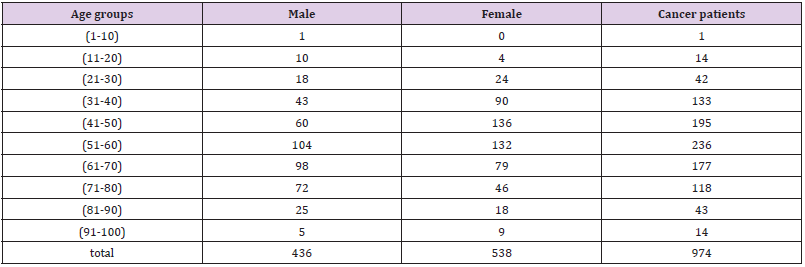
Table 2: Cancer distribution among gender type and age groups.
While women in general constitute the majority of cancer patients, this is due to the high prevalence of breast cancer among them. As the incidence of breast cancer peaks at the age below fifty (Figures 5 & 6 and Tables 2 & 3), the average age of cancer incidence among women is lower than the average age for men. On the other hand, prostate and lung cancer in males, both are occurred in male after the age of sixty (Figures 5 & 7 and Table 3). This reflects the nature of cancers affecting both sexes, while male primary malignancies tend to occur at a later age, and female primary cancers occur earlier. Another potential factor is that men tend to hide symptoms and delay seeking medical care, especially in developing countries [4,8]. In the present study, the most common cancers in males were colorectal (18.3%), lung (18.3%), prostate (12.6%), lymphoma (9.6%), leukemia (5%) and brain & CNS (4.1%).
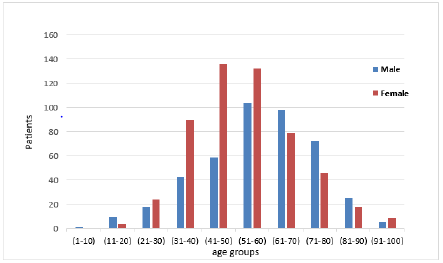
Figure 5: The number of cancer patients (n=974) in different age groups.
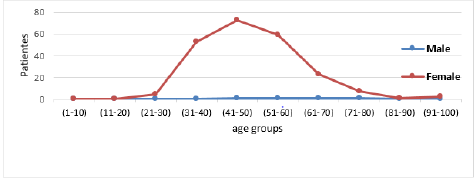
Figure 6: Age distribution of breast cancers in males and females.
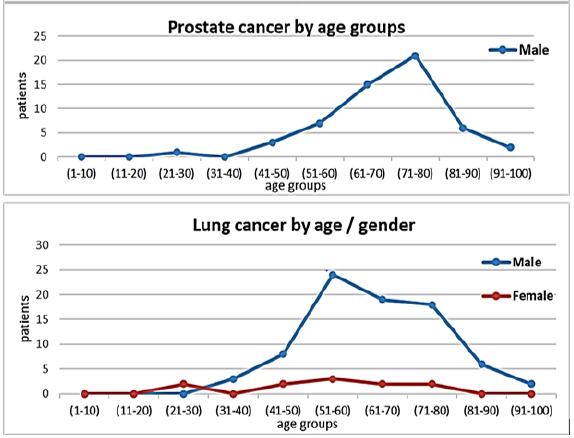
Figure 7: Age distribution of prostate cancer in males, and lung cancer in both males and females.
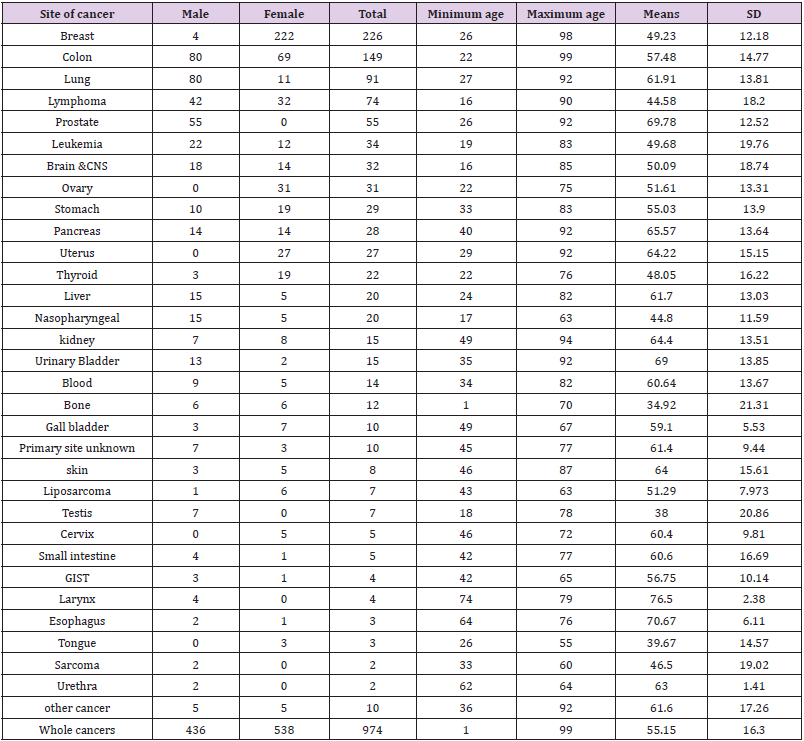
Table 3: Cancer incidences registered in NCI-Misurata 2016.
Note: SD: Standard deviation
While in females, they were breast cancer (41.2%), colorectal
(12.8%), lymphoma (5.9%), ovary (5.7%) uterus (5%), and
stomach (3.5%). This data is similar to cancer cases registered in
the western region of Libya 2008 [7]. They found that the most
common cancers in males were lung (15.6%), colorectal (12.3%),
prostate (9.9%), urinary bladder (7%) and stomach (5.5%) (Figure
4). While in females, they were breast cancer (23.7%), colorectal
(9.4%), uterus (8.6%), soft tissues (5.3%) and stomach (5.2%).
Furthermore, a study conducted in eastern Libya 2012 [9] which
observed that in men cancer of colon accounted for 22.3%, followed
by lung (20.3%), prostate (16.1%), pancreas (4.2%) and liver
(4.2%). In women, breast cancer was (41.5%), remained the most
common followed by colon cancer (16.4%), uterine (8%), ovary
(5.5%) and pancreas (3.1%). The most common types of cancers
found in the central region of Libya were breast, colorectal, lung,
leukemia, and lymphoma.
Compared with the western and eastern regions of Libya, there
was a similarity that lung, breast, and colon cancers were the most
common in the three regions. However, pancreatic, and ovarian
cancers were more common in the eastern region, but stomach and
bladder cancers were more common in the western regions. While
lymphomas and leukemias appeared more in the middle region. On
the other hand, colorectal, lung and prostate cancers were the most
common cancers diagnosed in men, while breast, colon and uterine
cancers were the most common types of cancer among women in
the three regions of Libya [7-9]. Breast cancer remains the most
common cancer for females in both the western and eastern
regions of Libya, rises in occurrence with age [6]. However, when
comparing average age of some cancers like breast among Libyan
patients with patients from the sub-Saharan Africa (e.g., Nigeria)
and Northern Europe patients (e.g., Finland), it was found to occur
at earlier ages in Libya and Nigeria than in Finland [8,13]. In this
study, we clearly saw that breast cancer occurred more in females
at the age of 41-50 years. The incidence of colon cancer in NCIMisurata
was the second highest in the central region.
It is suspected that there is a strong relationship between
this high rate of colon cancer and diet, as well as the absence of
weight control and changing lifestyle habits of the Libyan people.
The dramatic increase in the incidence of colorectal cancer may be
explained by the better availability of endoscopic techniques for
early detection and diagnosis [14,15]. The incidence of lung cancer
in NCI - Misurata occupied the third rank in the incidence of cancers
in the central region, and males showed 8 times more prevalence
than females (Figures 6-8 and Table 3). It is suspected that there is
a strong relationship between this high rate of lung cancer and the
smoking habits of Libyan males. This increase in the incidence of
lung cancer was noticed in Libya and all over the world. There were
1.82 and 1.59 million new lung cancer cases and deaths worldwide,
respectively [1]. The increase in the incidence of lung cancer can be
explained by the continuous improvement in radiological diagnostic
tools and methods of cytological and histological examination
for early detection of lung cancer. There is a significant lowering
trend for non-Hodgkin lymphoma in female patients than males,
however, it has remained fourth principal malignancy in women
and fifth malignant tumour in men after prostatic cancer (Figure
9 and Table 3).
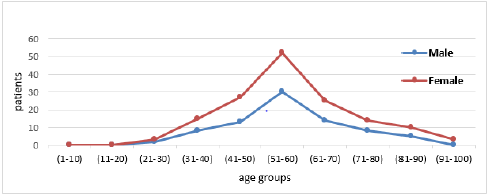
Figure 8: Age distribution of colorectal cancers in males and females.
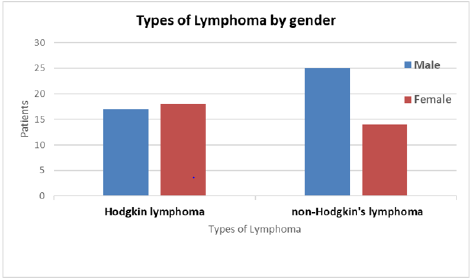
Figure 9: Gender distribution within both types of Lymphoma (HL and NHL).
Conclusion
Using a hospital-based cancer registry, this study determined the prevalence of cancer cases in Libya’s central area. Although the data was limited in various ways, such as the precise geographical data of the research locations, the cancer patient’s family history, and the patients’ lifestyle and habits, it was nevertheless useful. The presence of certain epidemiological data on patients, on the other hand, has given us with crucial information regarding the size and scope of malignant diseases in Libya. Despite the fact that the prevalence of cancer is higher in industrialized countries, cancer mortality is often higher in developing countries due to a lack of early detection and treatment. As a result, future research should include fatality rates as well as probable carcinogenic risks. Despite the fact that people have been displaced to Misurata from the eastern and southern areas of Libya, this study reflects the reality of cancer cases diagnosed and treated at the National Cancer Institute in Misurata in the center region of Libya (which is the third largest population city in Libya). This is the sole hospital in the area that provides medical services to oncology patients.
Acknowledgement
The authors grateful to the administration staff of the National Cancer Institute- Misurata for the support during this study.
Competing Interests
Authors have declared that no competing interests exist.
References
- Torre L, Bray F, Siegel R, Ferlay J, Lortet Tieulent J, et al. (2015) Global cancer statistics2012. CA Cancer J Clin 65(2): 87-108.
- Parkin D, Bray F, Ferlay J, Jemal A (2014) Cancer in Africa 2012. Cancer Epidemiol Biomarkers Prev 23(6): 953-966.
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, et al. (2015) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136(5): 359-386.
- Jemal A, Bray F, Center M, Ferlay J, Ward E, et al. (2011) Global Cancer Statistics. CA Cancer J Clin 61(2): 69-90.
- Ermiah E, Abdalla F, Buhmeida A, Larbesh E, Pyrhönen S, et al. (2012) Diagnosis delay in Libyan female breast cancer. BMC Res Notes 5(1): 452.
- Elzouki I, Benyasaad T, Altrjoman F, Elmarghani A, Abubaker KS, et al. (2018) Cancer incidence in western region of Libya: Report of the year 2009 from Tripoli pathology-based cancer registry. Libyan Journal of Medical Sciences 2(2): 45-50.
- (2008) Sabratha Cancer Registry. First annual report, 2006. Edited by African Oncology Institute, Sabratha, Libya.
- Boder J, Abdalla F, Elfageih M, Abusaa A, Buhmeida A, et al. (2011) Breast cancer patients in Libya: Comparison with European and central African patients. OncolLett 2(2): 323-330.
- Bodalal Z, Azzuz R, Bendardaf R (2014) Cancers in Eastern Libya: First results from Benghazi Medical Center. World Journal of Gastroenterology 20(20): 6293-6301.
- Mohamed Greesa, Musbah Alfege, Mohamed Alawni, Ebtisam Elshweehdi, Elham Abufalga, et al. (2008) Hospital based cancer registry report of Misurata Cancer Centre, Misurata, Libya.
- http://populationpyramid.net/libya/2016
- (2013) World Health Organization. International classification of diseases for oncology (ICD-O). (3rd)., 1st revision.
- Alragig M, Awaid R, Elsaghayer W, Boder J, Abdulmalek F, et al. (2015) Clinico-pathological characteristics of colon cancer in Libya MMSJ 2(2): 107-113.
- Juwid A, Alragig M, Eshtiwii A, Boder J, Abdalla F (2015) Different Colonoscopy Presentation Patterns with Clinicopathological Features of Colonic Cancer Patients Admitted in Misurata Cancer Center, Libya. Int J Curr Res Biosci Plant Biol 2(7): 107-113.
- Abdalla F (2012) Application of morphometry, static DNA ploidy analysis, and steroid receptor expression in diagnosis and prognosis of Libyan breast cancer. Doctoral thesis, University of Turku, Finland. Painosalama, ser D 1043: 128.
