 Review Article
Review ArticleAbstract
Objective: Neonatal sepsis remains a public health issue in the world and Nigeria is not excepted. As a prelude to evaluation of the situation in a Bayelsa state community, the objective of this review was to establish what is already known with regards to epidemiological and socioeconomic factors.
Method: A narrative method was adopted. On epidemiology, Nigeria was compared with in Sub-Saharan region and the world. Also, 10 years progress was assessed. On socioeconomic factors, focus was on determinants of neonatal infections and mortality.
Results: There is evidence of approximately 0.2% decline in neonatal mortality in Nigeria relative to a global 0.5%. The decline has been consistent decline in global average, but not in Nigeria. In terms of socioeconomic determinants, the age, educational level, and residence of mother as well as birthing place are among the factors.
Conclusion: In terms of what is known versus unknown regarding infectious control principles in NICU: there is evidence that enforcement among the healthcare workers improves compliance by staff and reduces neonatal nosocomial infections. What is unknown includes level of compliance in Bayelsa State NICUs and potential for improvement.
Keywords: Epidemiological Determinants; Neonatal ICU; Infection Control
Epidemiological Views of Neonatal Sepsis
Epidemiology is the study of determinants and distribution of diseases occurring in human population and it revolves around the questions of who, where, when, what and how about a disease. This has been a special theme of focus of research work in the department of department of public and community of the university [1-4]. Thereby, this section focuses on the global distribution as well as trends of neonatal sepsis and compared with Nigeria. The incidence and prevalence of neonatal sepsis varies between the developed world and developing countries alike. It differs from one healthcare facility to another. Studies indicates that the prevalence rate is 3-10 times higher in preterm than in full-term neonates. Similarly, the incidence is higher in low birth weight than normal weight babies, and in males than in females. Other factors in association are levels of obstetric and nursery care available, the presence of determinant factors like sanitation, water supply, poor socioeconomic status, delivery at home or unhygienic environment [5]. Neonatal intensive care units which cater for high risk and extremely low birth weight babies had their survival longer, Also, the risk of repeated infections especially nosocomial infections was higher. According to the United Nations and WHO, the global burden of neonatal sepsis is quite difficult to ascertain due to paucity of reliable information. It is only estimated that annually.
a. over 30 million people are affected worldwide.
b. 6 million deaths are attributable.
c. 3 million newborn and 1.2 million children suffer from sepsis globally every year, and about 3/10 deaths are due to neonatal sepsis and are thought to be caused by resistant pathogens [6-8].
d. One in ten deaths are associated with maternal sepsis with majority occurring in LMIC [6].
10 Years’ Landmark Review
The United Nation Children’s Fund (UNICEF) reports that levels are dropping both globally and in Nigeria [7]. Indeed, review of database show decline in neonatal mortality (Table 1). Other research report corroborates that the infection rates have modestly decreased in NICU, although there remain problematic cases among hospitalized preterm children. For instance, in 2013, 7.6 million children less than five years old died due to infections including sepsis [8]. Thus, despite major advances in NICU services and increasing research, neonatal sepsis still constitutes a global public health issue [9-12]. In a study carried out in the medical unit in south eastern Mexico to assess the risk and prognostic factors for neonatal sepsis prevailing at the medical unit, through the use of historic cohort design to assess the association between a series of neonates and mothers in admission to hospital evaluation, found that, 514 of 11,790 (4.3%) newborns: 387 of these cases were early-onset sepsis (<72h) (75.3%) and 127, as late-onset (>72h) (24.7%). Epidemiological ‘risk’ factor was emphasized to include age of onset, APGAR Score, birth weight, and length of hospital stay [13]. Yet, another report emphasizes gender and geographical location as additional risk factors, especially in South Asia, Sub- Saharan Africa, and Latin America [14].
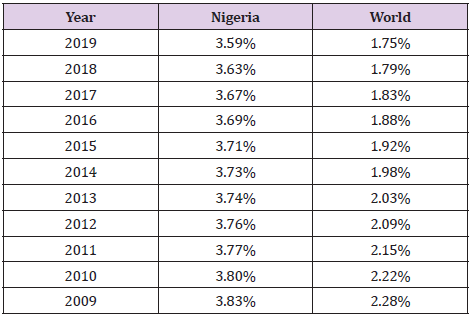
Table 1: Neonatal mortality rate decline in both Nigeria and global [7,11,12].
Many other research reports including some from Nigeria have these risk factors. Also, pathogens that causes neonatal sepsis vary by geographical region. In LMIC, gram-positive organisms were nearly as frequent as gram-negative in African countries, streptococcus algalaciae (GBS) was uncommon in South Asia region and streptococcus aureus was found less common in both Latin America and East Asia when compare with other regions [15-17]. The United Nations Inter-Agency Group Mortality Estimates states that, the first 28 days of live which is the neonatal period most vulnerable time for their survival, most children face the highest risk of dying at the first month, and an average global rate of 18 deaths per 1000 live births in 2018. Globally, 2.5 million children died in the first month of life in 2018 - approximately 7,000 neonatal deaths every day most of which close to three quarters dying with one third dying on the first day. With particular interest on Nigeria, Figure 1 below shows estimated neonatal sepsis deaths caused by bacteria resistance against first-line antibiotics in highburden countries.

Figure 1: Estimates of neonatal sepsis deaths antibiotic resistance in high-burden countries [18].
Africa/Sub-Saharan
Considering Nigeria being among the top 5 high-burden countries, a critical review of the decline in Nigeria’s neonatal mortality was compare with the global trend. It is observed that the extent or level of global decline has been quite consistent, whereas that of Nigeria was much at a slower pace until 2018 and now seems to be declining at a better rate than global as at 2019 (Figure 2). A study one the prevalence and risk factors of neonatal sepsis in Tanzania has report mortality rate of 69% [19], which is higher than that of Nigeria. Their findings underscored the importance of routine assessment and close monitoring of neonates as preventive measures. Also, together with the Nigerian trend, the observation is in line with a previous report that “on average, the pace of the decline across the sub-Saharan region has been too slow to meet up with the MDG 4 target” [20].
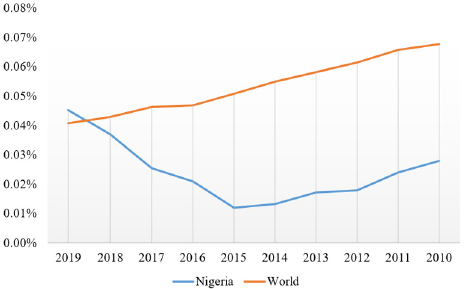
Figure 2: Neonatal death rates’ decline – consistent in global but not Nigerian [11,12].
Socioeconomic Determinants of Neonatal Sepsis in Nigeria
This section reviews the empirical literatures of Nigeria in regards on socioeconomic determinates of neonatal sepsis. A study carried out to determine the impact of the predominant socioeconomic factors that may contribute to neonatal sepsis in Jos University Teaching Hospital (JUTH), Nigeria, with mothers, care givers and case notes of 218 neonates. The result shows that the most common isolates were Klebsiella pneumonia, Staphylococcus aureus and Escherichia coli. It reports that delivery at home had the highest percentage of culture proven sepsis (52.2%). They however, observed that mothers with no formal education and those with only primary education also had high proportions of culture proven sepsis (41.1% and 58.8% respectively). Place of domicile, level of education of mother and poor feeding were factors that contributed significantly to neonatal sepsis by odds ratio [21].
In a study carried out in Northern part of Nigeria, among healthcare workers shows that inadequate workers knowledge, environmental related problems and lack of protective materials, equipment and utilities required to ensure safety was an issue. Noncompliance to the universal precaution of infection control practice was said to be because of non-availability of equipment [22]. A similar study carried out in University of Jos, North central Nigeria to determine the impact of the predominant socio-economic factors that may contribute to neonatal sepsis in the environment shows that delivery at home has the highest percentage of culture proven sepsis (52.2%). Uneducated mother and those with only primary school also had high proportions of culture of culture proven sepsis (41.1% and 58.8%), the environment where they live and poor feeding were factors that contributes seriously to the occurrence of neonatal sepsis. To get it right, it was imperative to get an accurate information on the etiology of infections responsible for the incidence of neonatal sepsis in Nigeria [21]. Similarly, study carried out on determinants of neonatal mortality in Nigeria: evidence from the 2008 demographic and health survey, found a higher birth order of newborns with a short birth interval ≤ 2 years (hazard ratio [HR] = 2.19 and newborns with a higher birth order with a longer birth interval > 2 years HR = 1.36, were significantly associated with neonatal mortality [23]. Other significant factors that affected neonatal deaths included were:
a. Neonates born to mothers younger than 20 years.
b. Neonates born to mothers residing in rural areas compared with urban residents.
c. Male neonates.
d. neonates with body size to be smaller than the average size.
e. Neonates delivered by caesarean section.
In a systematic review of studies from 1987 to 2017 for neonatal sepsis in Nigeria, out of which 24% (2,280) cases were selected for final review. The incidence of neonatal sepsis was 1.8% livebirths with range from 7-55/1000 livebirths while, the GBS incidence was 0.06/1000 livebirths with range from 0-2/1000 live births. They associated the incidence and mortality rates to poor parental education and low-income factors [16]. Another report indicated neonatal mortality rate for Nigeria as 36 deaths per 1,000 live births in the year 2018. According to the report, neonatal mortality rate has fallen gradually from 68.3 deaths per 1,000 live birth in 1969 to 36 deaths per 1,000 live births in 2018. Figure 3 below shows significant risk factors for sepsis in neonates reported at Lagos State University Teaching Hospital (LUTH). It shows data on four factors which are inborn of healthcare facility vs. out born (outside healthcare facility) and changes of antibiotics vs. maintaining one antibiotic [24].
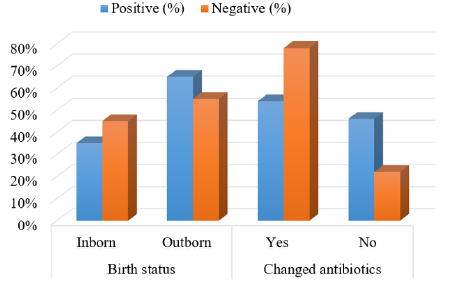
Figure 3: Comparative impact of risk factors for sepsis in neonates [24].
Sepsis is one of the most common causes of neonatal hospitalization and is estimated to cause 20% of all neonatal deaths worldwide. Between 2011 to 2013, a study was carried out on causative organisms of neonatal sepsis in Niger Delta University Teaching Hospital (NDUTH), Bayelsa State, 233 (49.6%) of 450 neonates admitted in the hospital were screened for sepsis. 97 (43.5%) of them were blood culture positive, with 52 (53.6%) of isolated organisms are Gram positive and 45 (46.4%) are Gram negative. The most frequently isolated organisms were staphylococcus aureus (51.5%) followed by Escherichia coli (16.5%) and Klebsiella Pneumonia (14.4%). All the isolated organisms show highest sensitivity to quinolones (an antibiotic derived from quinoline used chiefly against gram-negative organisms [25]. Most hospitals in Nigeria about 97% (28/29) are having adequate triage systems, but only 60% (16/27) follow some form of guideline for sepsis management in Nigeria. There was no consensus national guideline of pediatric sepsis. Over 50% of the respondents identified were deficit in parental education, poor access to healthcare service, failure to diagnose sepsis at referring institutions, lack of medical equipment and lack of definitive protocol for managing pediatric sepsis. Also, assessing baseline prevalence of sepsis and septic shock in Nigeria is challenging due to inadequate epidemiological data on sepsis and septic shock [26]. However, they observed that literature reviews between 1980 and 2008 did not show studies of prevalence, incidence, mortality, or case-fatality from sepsis in developed countries.
A related study carried out to determine the mobility and mortality of neonatal admission within 2015 to 2016, in the special care baby unit in Federal Medical Centre Birnin Kudu, Jigawa State, Nigeria, a total of 205 neonates were admitted to SCBU during the study period with the ratio of the males to females admitted was 2:1, the result shows that, the major cause of mobility was neonatal sepsis (32.2%), birth asphyxia (29.3%) and prematurity (18.5%). And overall mortality rate was 7.16% with birth asphyxia accounting for 13 (40.6%) of the total deaths [27]. Further, in a retrospective evaluation of 453 neonates to determine organisms present in early and late onset of neonatal sepsis and their antimicrobial susceptibility pattern in University of Port-Harcourt Teaching Hospital (UPTH) Nigeria between January to December 2007 [28]; it was reported that Klebsiela spp was the most common pathogen, accounting for 37.8% for the total isolates. Staphylococcus aureus (28.4%), Escherichia coli (11.8%), unclassified coliforms (8.3%), Pseudomonas spp (4.9%), Enterococcus spp (2.9%), Coagulase -negative Staphylococcus (2.5%) and Proteus spp (3.4%).
Conclusion
This review evaluated what is known about the behaviour of NICU healthcare workers and mothers of babies as determinants of neonatal sepsis. It is apparent to state that epidemiologically, neonatal sepsis is a serious public health and economic burden plaguing human race globally. Nigeria being the most populous country in Africa has one of the highest neonatal sepsis incident rates and third in the world (after India and China), which is responsible for about 30% of neonatal deaths. Effective prevention including regular periodic surveillance is imperative, and substantial achievements have been recorded over the past 10years. However, more efforts are still required, especially at the primary care levels where data are lacking such as in Bayelsa State. Hence the justification of proposed study. It will enable health planners and policy makers to improve the standard of healthcare facilities for preventive management of neonatal sepsis including providing information that could advance maternal and child health services in Nigeria.
References
- Agege EA, Nwose EU, Nwajei SD (2020) Epidemiology and health consequences of early marriage: focus on Delta State Nigeria. Int J Community Med Public Health 7: 3705-3710.
- Akuirene OA, Nwajei SD, Adjene JO, Ezekiel UN (2020) Epidemiology of respiratory distress in pregnancy and the newborn in Delta state Nigeria. International Journal Of Community Medicine And Public Health 7: 4631-4638.
- Odoko JO, Nwose EU, Nwajei SD, et al. (2020) Epidemiology of malaria as it relates to utilization of insecticide treated nets among pregnant women and under five years children in South-South Nigeria. Int J Community Med Public Health 7(10): 4157.
- Moyegbone JE, Nwose EU, Nwajei SD, Joseph OO, Emmanuel AA, et al. (2020) Epidemiology of visual impairment: focus on Delta State, Nigeria. Int J Community Med Public Health 7(10): 4171-4179.
- Pius S, Bello M (2017) Neonatal septicaemia in poor resource settings. Pediatric Infect Dis 2: 34.
- Bonet M, Souza JP, Abalos E, Bukola F, Marian K, et al. (2018) The global maternal sepsis study and awareness campaign (GLOSS): study protocol. Reproductive health 15: 16-16.
- (2020) United Nations. Levels and trends in child mortality: 2020 report.
- Wynn JL (2016) Defining neonatal sepsis. Curr Opin Pediatr 28: 135-140.
- Afroza S (2006) Neonatal sepsis - a global problem: an overview. Mymensingh medical journal: MMJ 15(1): 108-114.
- Procianoy RS and Silveira RC (2020) The challenges of neonatal sepsis management. J Pediatr 96 (1): 80-86.
- (2020) UN Inter-agency Group for Child Mortality Estimation. Neonatal mortality rate estimates: World.
- (2020) UN Inter-agency Group for Child Mortality Estimation. Neonatal mortality rate estimates: Nigeria.
- Leal YA, Álvarez-Nemegyei J, Velázquez JR (2012) Risk factors and prognosis for neonatal sepsis in southeastern Mexico: analysis of a four-year historic cohort follow-up. BMC pregnancy and childbirth 12: 48.
- Seale AC, Blencowe H, Manu AA, H Nair, R Bahl, et al. (2014) Estimates of possible severe bacterial infection in neonates in sub-Saharan Africa, south Asia, and Latin America for 2012: a systematic review and meta-analysis. Lancet Infect Dis 14(8): 731-741.
- Belizán JM, McClure EM, Goudar SS, O Pasha, Fabian E, et al. (2012) Neonatal death in low- to middle-income countries: a global network study. Am J Perinatol 29(8): 649-656.
- Medugu N, Iregbu K, Iroh Tam PY (2018) Aetiology of neonatal sepsis in Nigeria, and relevance of Group b streptococcus: A systematic review. PLOS ONE 13(7): e0200350.
- Medugu N, Iregbu KC, Parker RE, J Plemmons, P Singh, et al. (2017) Group B streptococcal colonization and transmission dynamics in pregnant women and their newborns in Nigeria: implications for prevention strategies. Clin Microbiol Infect 23(9): e679-673.
- Miller-Petrie M, Pant S, Laxminarayan R (2017) Drug-Resistant Infections. Major Infectious Diseases. 3rd (edn). Washington (DC): The International Bank for Reconstruction and Development / The World Bank.
- Jabiri A, Wella H, Seminolo A, Adellah Saria, Joyce Protas (2016) Prevalence and factors associated with neonatal sepsis among neonates in Temeke and Mwananyamala Hospitals in Dar es Salaam, Tanzania. Tanzania Journal of Health Research 18(4).
- Kinney MV, Kerber KJ, Black RE, B Cohen, Francis N, et al. (2010) Sub-Saharan Africa's mothers, newborns and children: where and why do they die? PLoS Med 7: e1000294.
- Onyedibe KI, Utoh-Nedosa AU, Okolo M, KIO O, O Ita, et al. (2012) Impact of socioeconomic factors on neonatal sepsis in Jos, Nigeria. Jos Journal of Medicine 6(2): 54-58.
- Amoran OE, Onwube OO (2013) Infection control and practice of standard precautions among healthcare workers in northern Nigeria. Journal of global infectious diseases 5(4): 156-163.
- Ezeh OK, Agho KE, Dibley MJ, John H, Andrew N, et al. (2014) Determinants of neonatal mortality in Nigeria: evidence from the 2008 demographic and health survey. BMC Public Health 14: 521.
- Shobowale EO, Ogunsola FT, Oduyebo OO, VI Ezeaka (2016) Aetiology and risk factors for neonatal sepsis at the Lagos University Teaching Hospital, Idi-Araba, Lagos, Nigeria. S Afr J Child Health 10(3): 147-150.
- Peterside O, Pondei K, Akinbami FO (2015) Bacteriological profile and antibiotic susceptibility pattern of neonatal sepsis at a Teaching Hospital in Bayelsa State, Nigeria. Trop Med Health 43(3): 183-190.
- Nwankwor OC, McKelvie B, Frizzola M, Krystal H, Hamila SK, et al. (2019) A national survey of resources to address sepsis in children in tertiary care centers in Nigeria. Frontiers in pediatrics 7: 234.
- Otu A, Elston J, Nsutebu E (2015) Sepsis in Africa: practical steps to stem the tide. The Pan African medical journal 21(323).
- Adedokun AA, Onosakponome EO, Nyenke CU (2020) Early onset and late onset of neonatal sepsis in a tertiary hospital, South-South, Nigeria. Journal of Advances in Microbiology 20: 19-29.
