 Research Article
Research ArticleAbstract
Background: The 2020 Global Nutrition Report by UNICEF highlights the high rate of deaths among children under five years of age, with India being one of the top five countries. Studies suggest that more than half of these early child deaths are attributable to malnutrition and its associated diseases, particularly in the case of countries with extreme poverty, scarcity of essential resources, lack of appropriate education, and wide disparities of wealth.
Objective: While several studies highlight the general nutritional determinants, literature lacks empirical investigation on details of the influencing factors. In this paper we address this gap and specifically explore the variables of wealth and maternal influences.
Methods: Using the Demographic and Health Survey (DHS) data set of 1,40,471 observations of children 2-5 years old, we employ Dietary Diversity Score (DDS) and Multiple Linear Regression (MLR) analysis to investigate the association between various influencing factors.
Result: The findings suggest that the wealth index of the household does not directly impact the DDS of children. Rather, in high wealth index households, the DDS of a female child tend to be lower than that of a male child. However, this difference tends to narrow with mothers’ higher levels of education. Further, we found maternal health to be a key determinant of the nutritional status of children.
Conclusion: These findings together bring out the fact that the wealth index of households does not contribute to the nutritional status of children unless the mothers have formal education and awareness to leverage the available wealth to provide adequate and diverse food to the children irrespective of their gender. Besides, maternal education would result in enhancing maternal health which would in turn influence a child’s nutritional status positively. Lastly, we conclude that facilitation of various health care facilities to women, indirectly and eventually leads to better nutritional intake for the child. These contributions are all the more significant in the current context of COVID-19 as poor countries face worsening of food security for underprivileged children.
Keywords: Malnutrition; Children; Dietary Diversity; Maternal Physical Health; Maternal Mental Health; Maternal Education; Gender
Introduction
Children malnutrition, like many other health outcomes, forms a multifaceted problem appear in triple burden namely undernutrition, micronutrient deficiencies, and overweight or obesity [1]. Malnutrition in its all forms primarily occurs due to the lack of nutritional adequacy in terms of limited or absence of consumption of diverse nutrients on a regular basis, characterized as imbalanced or bulky diet [2-4]. Malnutrition or lacking nutritional diet impairs the activity of immune cells and antibodies (HARVARD, 2021). This in turn reduce a child’s immunological outcomes to tackle infectious diseases such as acute respiratory infections and diarrheal diseases, alongside with weight loss, mucosal damage, invasion by pathogens and further cause reduced dietary intake which could hamper a child’s growth and overall development [5,6]. Furthermore, the prevalence of malnutrition in a child might result in mental illness including eating disorders such as anorexia nervosa (AN) and bulimia nervosa (BN) [7-9], and malabsorption and maldigestion of the food consumed [10,11]. Consequently, malnutrition in a child, if not addressed appropriately, could lead to severe damage to a child’s health and even mortality. Hence, malnutrition gets regarded as one of the major impediments to child well-being affecting all areas of a child’s physical and mental health, body immunity, growth, and development [12,13].
The adverse consequences of malnutrition on health status of children compel us to understand the influencing factors of malnutrition in children. Existing literature demonstrates malnutrition and its associated diseases to occur due to factors like maternal health, faulty childcare, less access to health care facilities, lack of sanitation, and hygienic facilities and large economic disparities [14-17]. In this paper we investigate the maternal factors that influence the dietary adequacy and further, nutritional status of children. Evidence shows that maternal adverse physical health associated diseases such as anemia during pregnancy are strongly associated with a child’s poor nutritional status and developmental outcomes [18,19]. Maternal malnutrition poses serious health effects on fetus or intrauterine growth retardation and increase the risk of poor pregnancy outcomes such as premature or low-birthweight babies and impairs the innate host defense mechanism, and further, diminishing the immune system of the body. This in turn leads to increasing susceptibility to infections associated with decreasing appetite, and consequently, causing child’s poor dietary intake which aggravate the risk of malnutrition in a [20-23]. Moreover, a child’s dietary pattern, particularly at the young age, is primarily similar to the maternal dietary intake in a household [24]. Hence, due to this similarity in dietary patterns consumption, a malnourished mother with restricted nutritious or poor-quality dietary pattern strongly increases the risk of poor nutritional dietary consumption of a child and further increase the risk of malnutrition and its associated diseases in every phase of the childhood life [25,26]. Studies also emphasize the importance of maternal education as an essential intervention in promotion of a child’s optimal health outcomes and nutritional status [27].
While several studies highlight the general determinants in maternal characteristics for children, existing literature lacks an empirical investigation on details of the maternal influencing factors including inequalities in terms of maternal health, healthcare activities, and maternal knowledge. This study attempts to address this gap and specifically explore the influence of inequalities in maternal characteristics in association with factors such as gender, wealth index, and child’s anthropometric measurements on the nutritional status of a child, in the context of India.
Materials and Methods
Data from the Demographic and Health Survey (DHS) were utilized. The data set includes key information for 2.5 lakhs children in India, including each child’s household and maternal characteristics, among others. 1340 variables were investigated, and 219 variables included as relevant for the study. Missing values in the data set are included using predictive mean matching which replaces the missing values according to the distribution of each datapoint. In the final analysis 1,40,471 data points were taken, which consisted of children in the age range of 2-5 years.
Dietary Diversity Score (DDS) forms the indicator for nutritional adequacy status. Dietary Diversity is defined as the number of different foods or food groups consumed in the previous day [28]. DDS was calculated by summing the number of times a unique food group was consumed during the last 24 hours. Food groups considered were cereals/roots, vegetables, fruits, legumes/lentils, high protein food, and milk/dairy products. DDS takes into account the quantity of any food group eaten that day. In other words, DDS gets calculated by considering the number of times a food group is eaten that day and not considers a minimum intake for that food group. The DDS ranges from 0 to 6. As an effective indicator of nutritional status, DDS forms the dependent variable in our study. The independent variables in the study have been presented in Table 1.
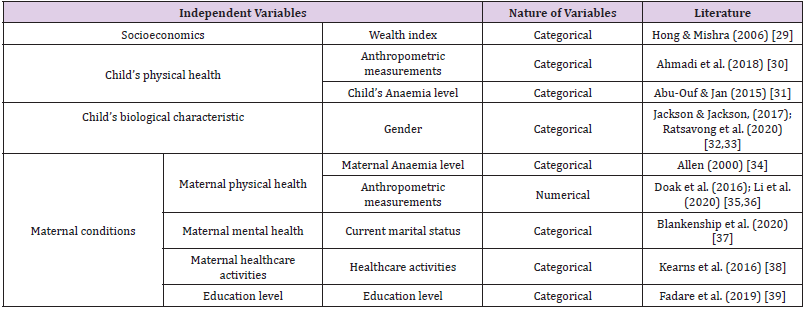
Table 1: Independent variables used in the regression model.
Statistical Analysis
Multiple Linear Regression (MLR) analysis investigates the association between the DDS and the independent variables presented in Table 1. The assumptions of normality, linearity and homoscedasticity were checked in order to ensure the validity of all the regression models. Further, as the number of variables is high, Akaike Information Criteria (AIC) was used to narrow down to a set of uncorrelated variables, thereby avoiding the issue of multicollinearity. Backward and forward stepwise regression analysis on all the variables with DDS as the dependent variable gave 78 variables as uncorrelated and has some influence on DDS. To address the research objective of the present study we adopted the variables presented in Table 1, among the 78 independent variables. Moreover, to ensure that the stepwise regression extracted variables were uncorrelated, bivariate correlation analysis was run as well. The correlation analysis suggested no significant correlation between any pair.
Result
Three regression models were constructed to understand the interaction of the variables (Table 1) with DDS. We probe the association in two ways, first in the presence of all the variables represented by an overall model and second, through the interaction of independent variables with various sub-groups of children through DDS. These sub-groups include gender and anthropometric measurements (height for age, weight for height, weight for age). The independent variables are regressed with DDS of 1,40,471 children.
Table 2 shows the association between DSS and the maternal physical health in terms of anemia level and anthropometric measurements. Variables are regressed for an overall analysis and specific interaction of maternal physical heath factors with various sub-groups of children, including gender, wealth index and anthropometric measurements (height for age, weight for height, weight for age). Table 3 shows that the association between the maternal mental health in terms of marital status, and the DDS of children. An overall model and a model for interaction of maternal mental health factors with various sub-groups of children is developed. These sub-groups include gender, wealth index, and anthropometric measurements (height for age, weight for height, weight for age). Table 4 shows that the association between the maternal healthcare activities in terms of pregnancy duration, number of antenatal visits during pregnancy, baby’s postnatal check-up within 2 months, during pregnancy given or bought iron tablets syrup, and maternal knowledge in terms of highest educational level (primary, secondary, or higher) and the DDS of children. An overall model and another model to see the interaction of maternal healthcare activities and knowledge factors with various sub-groups of children is developed. These sub-groups include gender, wealth index, and anthropometric measurements (height for age, weight for height, weight for age).
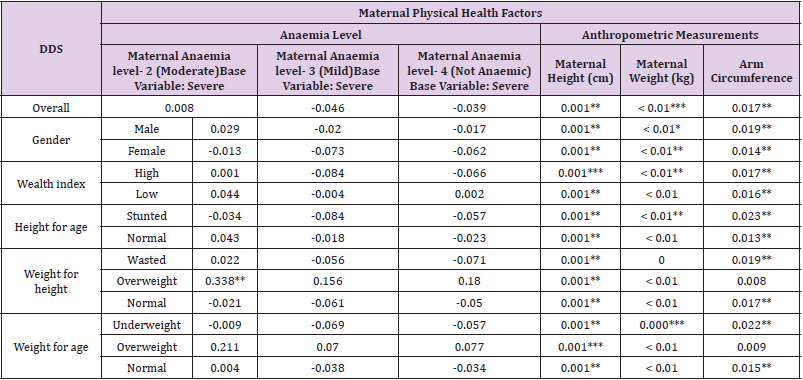
Table 2: Regression Analysis for maternal physical health factors.
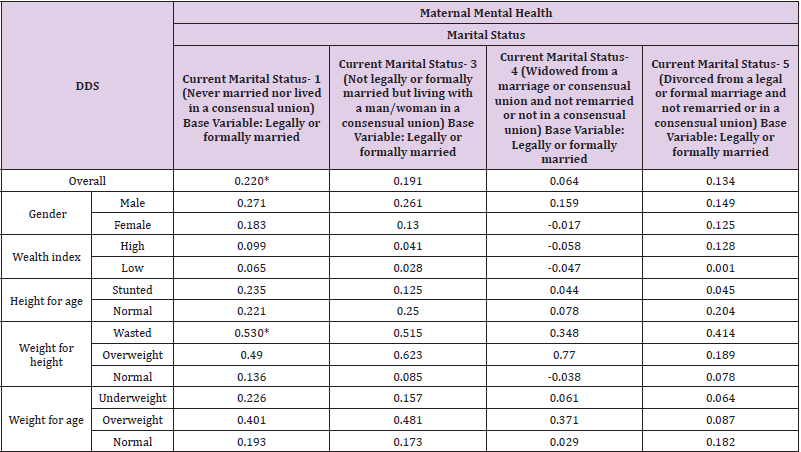
Table 3: Regression analysis for maternal mental health factors.
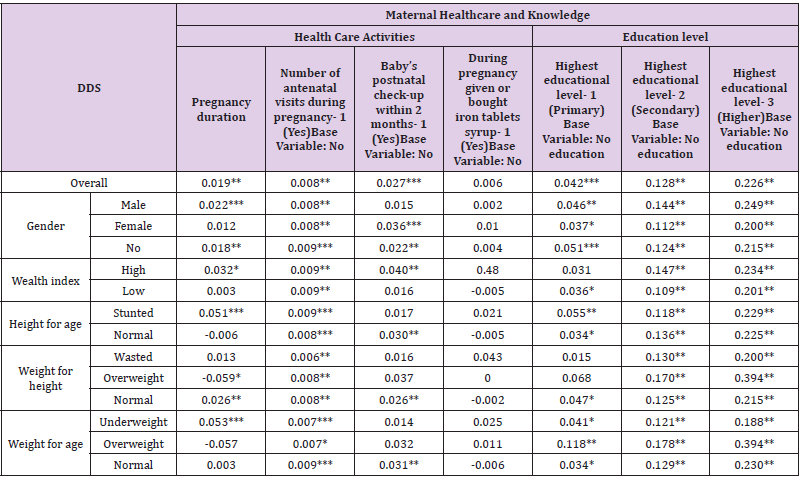
Table 4: Regression analysis for maternal mental health factors.
Discussion
An overall significant relationship exists between a maternal physical health in terms of mother’s anthropometric measurements including height, weight, and arm circumference, and the child’s nutritional diversity. While the mother’s level of anemia (long term health status) does not significantly impact the child height and weight, but the maternal anthropometric measurements are significantly related to indicators of her nutritional status which in turn exclusively indicates a child’s nutritional status. Maternal weight and DDS of children belonging to high wealth index households have a positive significant association. High wealth index contributes to better diet quality due to affordability of varied diverse food. Thus, inclusion of diverse nutritional food in a mother’s diet, significantly increases the likelihood of a child consuming these nutrients, which would eventually lead to a better DDS [40,41]. However, in case of low wealth index households, even when the mother demonstrates good health, food insecurity and low affordability persists, depriving a child of necessary nutrients, influencing their DDS negatively. With regard to a child’s postnatal check-up, we see a positive influence on the DDS of children belonging to high wealth index households. Higher wealth index provides better accessibility and availability to health care services, contributing to beneficial health outcome for children. On the other hand, low wealth index households have difficulty in affording quality health care and thus, post-natal health care access does not significantly contribute to better nutritional outcomes in terms of DDS.
Moreover, the results indicates that the baby’s postnatal check-up positively effect on the DDS of children with normal anthropometric measurement (height for age, weight for height, weight for age). The postnatal check-up helps to ensure the child’s optimal health status through measuring and record of weight, height, growth and development progress and other important health information. Hence, the health check-up used to monitor a child growing process and in the certain conditions of a child’s illness help to prevent and treat health complications including maternity services support related to breastfeeding and childcare practices [42,43]. Consequently, this can contribute to maintain and improve a child’s health status as well as nutritional status and thus, leading to better DDS, rooted in proper dietary intake of healthy children.
As compared to married marital status, an unmarried mother is more likely to positively influence a child’s DDS. This corroborates the findings of some studies [44] that unmarried mothers spend equivalent amounts of time on childcare activities including feeding, healthcare and rearing and less time on housework compared to married mothers. Number of antenatal visits during pregnancy are important in improving the DDS of children. The WHO recommends at least eight antenatal visits during pregnancy to treat problems and for immunization. The antenatal visits ensure health of a mother and in turn promote the nutritional status of a baby. Further, the baby’s postnatal check-up and DDS have a positive association. Postnatal care ensures a baby’s optimal care as well as the health practices like vaccination. This contributes to improving a child’s health with positive long-term consequences.
Maternal education is significantly positively associated with a child’s DDS. Maternal education influences a positive attitude towards health-seeking behaviour including awareness of child’s immunization, causes of illness, and essential awareness of prevention, and treatment of diseases. Therefore, maternal knowledge regarding nutritious diet also significantly helps to maintain a child’s heath.
Conclusion and Implications
The findings together clearly bring out the fact that the wealth index of households does not contribute to the nutritional status of children unless the mothers have formal education and awareness to leverage the available wealth to provide adequate and diverse food to the children irrespective of their gender. Moreover, the findings affirm the significance of maternal health on a child’s nutritional status. Thus, combined together, these finding asserts the importance of welfare of mothers in terms of facilitation of proper health care and quality education for better nutritional status of children. Hence, an urgent call for policies promoting the health and education of women across the country gets highlighted. The benefits of such policies would be two folds including promotion of health and well-being of mothers which would ultimately result in them providing better health care to the children thereby improving their nutritional status.
Lastly, the results contends that a mother’s accessibility to healthcare facilities have a considerable impact on a child’s DDS as it helps in tackling various health issues that might lead to poor nutritional intake and hence poor DDS. Thus, health policies nationwide must lay an exclusive focus on providing better accessibility to healthcare facilities for women in order to improve the nutritional intake of a child. Hence, in the essence our study contributes to the health policy by implying the importance of maternal health and education, proper environmental condition, and better accessibility to health care facilities in ensuring better nutritional intake of children and thus, tackling the alarming situation of malnutrition in India.
Funding Statement
This research is funded by a grant from the Akshaya Patra Foundation, India. The grant number is: SP/APRL-19-0001. The data that support the findings of this study are available on request from the corresponding author [Bita Afsharinia].
Disclosure of Interest
The authors report no conflicts of interest.
References
- (2016) UNICEF. The faces of malnutrition | Nutrition | UNICEF.
- (2021) Children for Health Malnutrition Information Sheet | Children for Health. Children for Health.
- Ananya Mandal M (2019) Causes of malnutrition. News Medical Life Science.
- (2020) WHO Fact Sheets-Malnutrition. WHO.
- Childs CE (2019) Diet and immune function. British Journal of Biomedical Science 51(3): 252-259.
- Katona P, Katona-Apte J (2008) The interaction between nutrition and infection. Clinical Infectious Diseases, 46(10): 1582-1588.
- Bravender T, Bryant-Waugh R, Herzog D, Katzman D, Kriepe RD, et al. (2010). Classification of eating disturbance in children and adolescents: Proposed changes for the DSM-V. European Eating Disorders Review 18(2): 79-89.
- (2019) Narayana Health Eating disorders in children and what you can do about it -Narayana Health. Narayana Health.
- Rethink MentalIllness (2021) Eating Disorders. In Rethink Mental Illness.
- Murphy JL, Badaloo AV, Chambers B, Forrester TE, Wootton SA, et al. (2002) Maldigestion and malabsorption of dietary lipid during severe childhood malnutrition. Archives of Disease in Childhood 87(6): 522–525.
- Suda M, Nagamitsu S, Kinosita M, Matsuoka M, Ozono S, et al. (2017) A child with anorexia nervosa presenting with severe infection with cytopenia and hemophagocytosis: A case report. BioPsychoSocial Medicine11(1): 1-4.
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE, Group, the W. C. H. E. R (2005) WHO estimates of the causes of death in children. National Center for Biotechnology Information (NCBI): 1147-1152.
- Ijarotimi OS (2013) Determinants of Childhood Malnutrition and Consequences in Developing Countries. Current Nutrition Reports: 129-133.
- Mittal A, Singh J, Ahluwalia S (2007) Effect of maternal factors on nutritional status of 1-5-year-old children in urban slum population. Indian Journal of Community Medicine 32(4): 264.
- Shyam AG, Fuller NJ (2020) Is child undernutrition associated with antenatal care attendance in Madhya Pradesh, India? Journal of Family Medicine and Primary Care 6(2): 169-170.
- Singh A (2020) We are Intech Open, the world’ s leading publisher of Open Access books Built by scientists, for scientists TOP 1 % Childhood Malnutrition in India. In Perspective of Recent Advances in Acute Diarrhea. IntechOpen, 7th floor 10 Lower Thames Street London, EC3R 6AF, UK.
- (2021) UNICEF Malnutrition in Children - UNICEF DATA. UNICEF.
- Imdad A, Bhutta ZA (2012) Maternal nutrition and birth outcomes: Effect of balanced protein-energy supplementation. Paediatric and Perinatal Epidemiology 26(SUPPL. 1): 178-190.
- Leddy MA, Power ML, Schulkin J (2008) The impact of maternal obesity on maternal and fetal health. Reviews in Obstetrics & Gynecology 1(4): 170-178.
- Khattak UK, Iqbal SP, Ghazanfar H (2017) The Role of Parents’ Literacy in Malnutrition of Children Under the Age of Five Years in a Semi-Urban Community of Pakistan: A Case-Control Study. Cureus 9(6).
- Rytter MJH, Kolte L, Briend A, Friis H, Christensen VB (2014) The immune system in children with malnutrition - A systematic review. PLoS ONE 9(8).
- Schaible UE, Kaufmann SHE (2007) Malnutrition and infection: Complex mechanisms and global impacts. PLoS Medicine 4(5): 0806-0812.
- (2018) UNICEF Canada (2018) Malnutrition | UNICEF Canada: For Every Child. UNICEF Canada.
- (2012) USAID Maternal dietary diversity and the implications for children’ s diets in the context of food security. In Infant & young child nutrition project (Issue January).
- Savage JS, Fisher JO, Birch LL (2007) Parental infulence on eating behavior. The Journal of Law, Medicine & Ethics 35(1): 22-34.
- Scaglioni S, Cosmi V De, Ciappolino V, Brambilla P, Agostoni C (2018) Factors Influencing Children’ s Eating Behaviours. Nutrients: 1-17.
- Van Ansem WJC, Schrijvers CTM, Rodenburg G, Van de Mheen D (2014) Maternal educational level and children’s healthy eating behaviour: Role of the home food environment (cross-sectional results from the INPACT study). International Journal of Behavioral Nutrition and Physical Activity 11(1): 1-12.
- Rathnayake KM, Madushani P, Silva K (2012) Use of dietary diversity score as a proxy indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Research Notes 5: 2-7.
- Hong R, Mishra V (2006) Effect of wealth inequality on chronic under-nutrition in Cambodian children. Journal of Health, Population and Nutrition 24(1): 89-99.
- Ahmadi D, Amarnani E, Sen A, Ebadi N, Cortbaoui P, et al. (2018) Determinants of child anthropometric indicators in Ethiopia. BMC Public Health 18(1): 1-9.
- Abu-Ouf NM, Jan MM (2015) The impact of maternal iron deficiency and iron deficiency anemia on child’s health. Saudi Medical Journal 36(2): 146-149.
- Jackson RT, Jackson RT (2017) Some Factors Influencing Variation in Nutritional Needs and Requirements of Children Some Factors Influencing Variation in Nutritional Needs and Requirements of Children. Journal of Children’s Health: 7069(March).
- Ratsavong K, Van Elsacker T, Doungvichit D, Siengsounthone L, Kounnavong S, et al. (2020) Are dietary intake and nutritional status influenced by gender? The pattern of dietary intake in Lao PDR: A developing country. Nutrition Journal 19(1): 1-16.
- Allen LH (2000) Anemia and iron deficiency: Effects on pregnancy outcome. American Journal of Clinical Nutrition 71(5 SUPPL.): 1280-1284.
- Doak CM, Campos Ponce M, Vossenaar M, Solomons NW (2016) The stunted child with an overweight mother as a growing public health concern in resource-poor environments: A case study from Guatemala. Annals of Human Biology 43(2): 122-130.
- Li Z, Kim R, Vollmer S, Subramanian SV (2020) Factors Associated with Child Stunting, Wasting, and Underweight in 35 Low- and Middle-Income Countries. JAMA Network Open 3(4): e203386.
- Blankenship JL, Gwavuya S, Palaniappan U, Alfred J, DeBrum F, et al. (2020) High double burden of child stunting and maternal overweight in the Republic of the Marshall Islands. Maternal and Child Nutrition 16(S2): 1-8.
- Kearns AD, Caglia JM, Ten Hoope-Bender P, Langer A (2016) Antenatal and postnatal care: A review of innovative models for improving availability, accessibility, acceptability and quality of services in low-resource settings. BJOG: An International Journal of Obstetrics and Gynaecology 123(4): 540-548.
- Fadare O, Amare M, Mavrotas G, Akerele D, Ogunniyi A (2019) Mother’s nutrition-related knowledge and child nutrition outcomes: Empirical evidence from Nigeria. PLoS ONE 14(2): 1–17.
- Broilo MC, Vitolo MR, Stenzel LM, Levandowski DC (2017) Mothers’ perceptions of their own diets and the diets of their children at 2-3 years of age. Psicologia: Reflexao e Critica 30(1).
- Hart CN, Raynor HA, Jelalian E, Drotar D (2010) The association of maternal food intake and infants’ and toddlers’ food intake. Child: Care, Health and Development 36(3): 396-403.
- Australia H (2019) Health checks for babies. Pregnancybirthbaby; Healthdirect Australia.
- Urakami T (2018) Importance of Growth Monitoring by a Health Checkup in Detecting Growth Disorders in Young Children. Biomedical Journal of Scientific & Technical Research 11(3): 8489–8491.
- Joanna R Pepin, LCS (2018) Marital Status and Mothers’ Time Use: Childcare, Housework, Leisure, and Sleep. Physiology & Behavior 176(10): 139-148.
