 Research Article
Research ArticleABSTRACT
Background: Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a widespread disease among the elderly population worldwide. Skeletal imaging is essential for the diagnosis of the disease and the complications that occur. Of these, Conventional Radiography (CR) is most commonly used due to the occurrence of characteristic changes of diagnostic significance and the low cost of the examination compared to Computed Tomography and (CT) and magnetic nuclear tomography (MRI).
The Aim: The aim of the study was to analyze the results established by CR and their correlation with biochemical results in patients with diffuse idiopathic skeletal hyperostosis.
Materials and Methods: The results of the CR of the axial and peripheral skeleton in 225 patients with DISH, who meet the classification criteria of Resnick et Niwayama and the Mata-score system, are analyzed. The patients were treated at the Rheumatology Clinic of “St. George” University Hospital, Plovdiv and the “St. George” Rheumatology Diagnostic Center. The radiographs were analyzed by two independent radiologists and the results were completed in specially made slips. The biochemical parameters were studied in the Central Laboratory, University Hospital “St. George”, Plovdiv. The statistical processing was carried out through the statistical program SPSS ver 24.
Results: Comparison of the Resnick et Niwayama criteria with the Mata-score system shows that the former criteria are significantly less sensitive and the use of the latter is recommended in routine rheumatology practice (p <0.01). A significant correlation was found between Mata-score in patients with DISH with the age of patients, the duration of complaints, Visual analog scale for pain assessment by the patient, elevated serum blood sugar levels, glycated hemoglobin, C-peptide, uric acid, total cholesterol and triglycerides (p <0.001).
Conclusion: Our results described in detail the findings found in patients with Diffuse Idiopathic Skeletal Hyperostosis and demonstrated the benefits of using Matacriteria in the diagnosis of DISH. Significant correlations were found between CR results and biochemical data. We recommend that rheumatologists use Mata-criteria in routine clinical practice to diagnose DISH.
Keywords: Diffuse Idiopathic Skeletal Hyperostosis; Conventional Radiography; Classification Criteria
Abbreviations: DISH: Diffuse Idiopathic Skeletal Hyperostosis; CR: Conventional Radiography; ALL: Anterior Longitudinal Ligament; CT: Computed Tomography
Introduction
Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a widespread disease among the elderly population. It is observed in the different ethnic groups, from 2-3% of the eastern peoples [1-3], to 10-20% among the caucasian race [4-6], however, a number of aspects regarding the course and diagnosis of the disease are not clarified [7-9]. Imaging studies - Conventional Radiography (CR), computed axial tomography (CT) and magnetic Resonance Imaging (MRI) are essential for diagnosis, complications and the distinction of DISH from other related diseases [10-12]. Of these, CR is most commonly used due to the occurrence of characteristic radiological changes in the axial and peripheral skeleton. Some authors consider that “Chest radiograph is a gold screening test for diagnosing DISH” [2,13,14]. Resnick et Nivayama, 1976, described the changes found by CR in patients with DISH and demonstrated that the disease is not limited to the spine [15]. In subsequent years, these findings were confirmed by other authors [16-21]. The authors note that changes initially occur in the lower right thoracic segment (around Th 9, 8, 7, 10). Slight fine calcification of the cortex of the anterolateral surface of the vertebrae is observed, with the newly formed bone having a linear shape and uneven contours [15]. Later, this calcification intensifies and can be found in the bodies of the vertebrae and their edges.
The contours of the vertebrae are uneven (bumpy). Along their anterolateral edge, broad, horizontal growths are observed, which grow, bend slightly upwards and resemble a candle flame (flowing candle wax), can merge and form bone bridges, causing ankylosis of the affected area. Calcification and ossification of the Anterior Longitudinal Ligament (ALL) is also found, which is seen as a contrast strip located on the anterolateral part of the vertebrae, which passes over the interdiscal space. This strip can be narrow (about 2 millimeters), but can also be wider (up to 20 millimeters), coarser and with uneven edges. Its shape is wavy (flowing ossification}, and the waves are visible above the interdiscal space. In about 20% of patients with lateral radiography can find a narrow gap (enlightenment, gap) between the vertebral bodies and the ossified ligament. affect other spinal ligaments. The interdiscal space (especially at the onset of the disease) is completely preserved, and the apophyseal and sacroiliac joints are not altered [22,23].
Radiographic changes can be found at all sites of the peripheral skeleton and the soft tissues around it [20,21]. In the peripheral skeleton hyperostoses are observed especially on the diaphysis, tubers, trochanters, ossification of the ribs and pelvis, and in the soft tissues thickening, calcification or ossification and irregularities. In the field of entheses (especially in the pelvis) these changes are more pronounced, often in the form of a small broom (whistering ossification) [15,24-26]. A significant problem in patients with DISH is that the diagnosis is made when there are already various manifestations such as fractures, a consequence of minimal trauma, back pain, non-response to treatment, dysphagia and dyspnea, the appearance of pseudoarthrosis [27-32], neurological and orthopedic complications of abrupt movement of the spine, which is not clear what disease they are associated with [33-35]. The currently used diagnostic criteria for DISH are from the last century. They are based on radiological changes mainly of the spine: criteria of Julkunen, et al. [36], criteria of Resnick et Niwayama [15], criteria of Utsinger, 1985 [37,38]. These radiological criteria are visible only 10-15 years after the onset of the disease and cannot be used for early diagnosis [32], so it is recommended to look for new, more modern ones [2]. In the routine rheumatologists practice, the criteria of Resnick et Niwayama [15] are most often used.
According to Julkunen, et al. [36], the diagnosis of DISH can be confirmed by the presence of bridges connecting between two or three vertebral bodies, at least at two sites of the thoracic spine [36]. Utsinger, et al. [38], held that the diagnosis of DISH could be made by involving three consecutive thoracic vertebral bodies in the disease process, to which should be added the presence of peripheral enthesopathies [36]. According to Mata and co-authors, Mata’s score 1-3 is assumed that the patient has initial changes for DISH, 4-6 is considered a moderate form and more than 7 - a severe form of the disease [39,40]. Mader, et al. [2] recommend that all researchers be “encouraged” to seek new diagnostic criteria for DISH that include constitutional, demographic, and metabolic factors.The Aim
The aim of the study was to analyze the results established by CR, as well as the results of the assessment of Mata score in patients with DISH from the Bulgarian population.
Materials and Methods
The results of the CR of the axial and peripheral skeleton in 425 patients with DISH, are analyzed. The patients were treated at the Rheumatology Clinic of “St. George” University Hospital, Plovdiv and the “St. George” Rheumatology Diagnostic Center, Bulgaria. The radiographs were analyzed by two independent radiologists and the results were completed in specially made slips. The biochemical parameters were studied in the Central Laboratory, University Hospital “St. George”, Plovdiv. The control group included 150 patients, healthy individuals, without complaints of pain and stiffness in the musculoskeletal system, similar in sex and age to the monitored group of patients who visited the University Clinic of Rheumatology “St. George”, Plovdiv, after being invited by researchers through general practitioners. The control group has no diseases and does not accept therapy. The statistical processing was carried out through the statistical program SPSS ver 24.
Including criteria for patients in the study:
a. Age over 18 years.
b. Confirmed diagnosis of DISH according to the criteria of Resnik, et al. [15] and / or criteria of Julkunen et al., with documented radiographic evidence of the disease.
c. Different duration of the disease.
d. Patients who assist in the study and provide medical documentation for concomitant diseases and previous hospitalizations.
e. Excluding criteria for patients in the study:
f. Presence of psoriasis or family history of psoriasis and ankilosing spondylitis, HLA B27+.
g. Presence of inflammatory bowel disease.
h. History of hematological and renal diseases.
i. Cognitive impairment.
j. Presence of a neoplasm manifested in the last 5 years.
Research Approach
a. Prospective approach for suitable patients from 2013- 2020. The study included patients hospitalized in the Clinic of Rheumatology, University Hospital “St. George”, Plovdiv, Bulgaria or visited a rheumatological practice, DCC “St. George”, Plovdiv
b. Collection of comprehensive information on clinical complaints for patients, which were coded and available to the research team, of which patients were informed. The individual results from the obtaine
c. Determination of biochemical parameters -glucose, glycated hemoglobin, C-peptide, uric acid, total cholesterol and triglycerides.
d. Readings are the results of conventional radiography performed on the thoracolumbar spine and peripheral areas of patients in the study.
e. Statistical data processing by computer program. SPSS ver 24.
CR Examination
The CR examination were taken at the Department of Radiology, Medical University, Plovdiv, using a conventional digital CR machine with the possibility of scopic and graphic examinations. All CR imaging tests comply with the national standard in Imaging Diagnostics and have minimal radiation exposure for the patient. A Siemens AXIOM Iconos R200 digital Japanese CR machine, a CR system for universal use in hospitals, a system for digitization of conventional CR and disk recording were used. The CR examination were analyzed sequentially by two radiologists and were reflected in a special slip adapted for the purpose of new followup. The analysis of radiological findings of the spine includes manifestations characteristic of the disease: hyperostosis of the vertebral bodies and edges, calcification and ossification of the Anterior Longitudinal Ligament (ALL) with a wavy character (flow ossification), the presence of osteophytes, vertically intervertebral vertically apophyseal and sacroiliac joints, etc.
The criteria of Resnick et Niwayama [15] include the following three findings:
a. Presence of abundant calcification or ossification of the ALL on the anterolateral surface of at least 4 vertebral bodies of the thoracic spine (flowing ossification), with the presence or absence of bone growths.
b. Preserved height of the intervertebral space and lack of major radiographic changes for degenerative disc diseases, including vacuum phenomenon and marginal vertebral sclerosis.
c. Lack of apophyseal joint changes (degenerative, ankylosing) and sacroiliac inflammatory manifestations (erosions, sclerosis, fusion).
According to Julkunen, et al. [36], the diagnosis of DISH can be confirmed by the presence of bridges connecting between two or three vertebral bodies, at least at two sites of the thoracic spine [36].
The Mata’s score (1998) is defined as:
a. In the absence of ossification,
b. In ossification without bone bridges,
c. Ossification and incomplete bone bridges,
d. In ossification with full bridges
e. In severe ossification with increasing width of the bridges [39].
In the peripheral skeleton, the presence of enthesitis (thickening, irregularities and ossification of the soft tissues of the enthesion), ligamentitis (thickening and calcification of the ligaments and their insertion sites), tendinitis (the same changes in the tendons), the presence of joint calcification are sought, hyperostosis or exostosis of the bones (especially of the diaphysis), their edges, tubers and trochanters, the presence of characteristic osteophytes (mainly of the heel and olecranon), compaction and calcification of the joint capsules and surrounding soft tissues, width of the joint space and etc. 66.93% of the patients with DISH, radiographs of the peripheral skeleton were performed due to the respective disease manifestations.
Patients
The study of the demographic indicators of the patients are presented in Table 1.
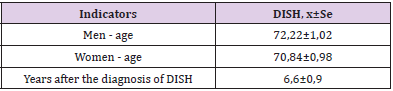
Table 1: Mean age, time from onset of complaints to diagnosis and time after placement and in years in the surveillance group, x ± Sd.
Statistical Data Processing
The collected information was checked, coded and entered into a computer database for further statistical grouping, recoding and analysis. The following statistical methods for analysis and processing were used: variation analysis to describe quantitative variables with normal or close to normal distribution. With the Kolmogorov-Smirnov test the variation series were checked for normality of the distribution, alternative analysis for estimation of frequency distributions in qualitative and grouped data, correlation analysis - calculated by ANOVA-test and Fischer coefficient and software products - statistical data processing was performed using SPSS ver. 24, with significance p> 0.05.
Results
Hyperostosis of the 4 vertebral bodies of the thoracic and lumbar spine was demonstrated in 89.64% of the observed patients with DISH. They are located mainly on the edges of the vertebrae, which is why their contours are often uneven. Calcification and ossification of the ALL is observed mainly in the thoracic spine, which is seen wavy, like a crest of wool above the interdiscal space and a depression in the middle area of the vertebrae. Rarely, ossification is diffuse, focal changes are more often seen, and the individual areas of ossification are seen denser, with an elongated shape, 0.5-1.5 cm in size (Figure 1). Affection of the apophyseal and sacroiliac joints is rare, as they are not always well visualized (15.05%). Mild degenerative changes of the intervertebral disc were found in 44.94% of the monitored patients (Table 2). 89.64% of all observed patients fully met the criteria of Resnick et al. for the disease, 10.36 % do not cover them and despite the visible CR finding involving 3 vertebral bodies in these patients. At the first visit to the rheumatologist of all patients was calculated Mata’s score. The next visits were every 2 years and CR was also performed. The radiographs were re-evaluated to Mata’s score and the results are presented in Table 3.
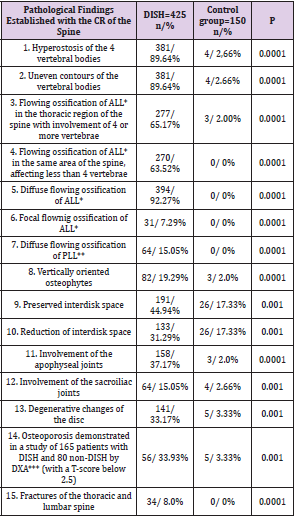
Table 2: Pathological findings in patients with DISH established by conventional radiography of the spine and in control group, (n,%).
Note: *ALL - anterior longitudinal ligament
**PLL – posterior longitudinal ligament
***Dual-energy X-ray absorptiometry

Table 3: Distribution of patients with DISH by gender and Mata-score (n / p ± Sp).
Note: P1- gender significance; P2 - significance by weight.
At the first visit to a rheumatologist 15.76% of all patients have Mata’s score 1-3, which means an initial diagnosis, in the following years this percentage decreases, and at 4 visits only 1.03% were with Mata’s score 1-3. In contrast to these results, 20.70% of patients have a Mata’s score > 7, at the last visit they were 53.10%. We observed for 8 years deterioration in Mata’s score 32.4%, which shows the rate of development of the disease (Table 3). Correlation between CR results in patients with DISH, Mata’s score, and biochemical parameters is by ANOVA-test and Fischer coefficient (Table 4). Additional radiographs were taken in 118 patients with a history of peripheral skeletal complaints. Characteristic changes were found (ossification of the edges, especially of the long bones, tubers and trochanters, ligaments, tendons, joint capsules; osteophytes, most already on the spotted bone, olecranon and patella, irregularities at the sites of insertion of tendons and ligaments, thickening of soft tissues. Most often such changes were observed in the knee joint (20.96%), followed by the hip (12.79 %), distal interphalangeal joints (9.67%), ankle joints (8.06%), shoulder joints (7.25%), etc. from all patients.
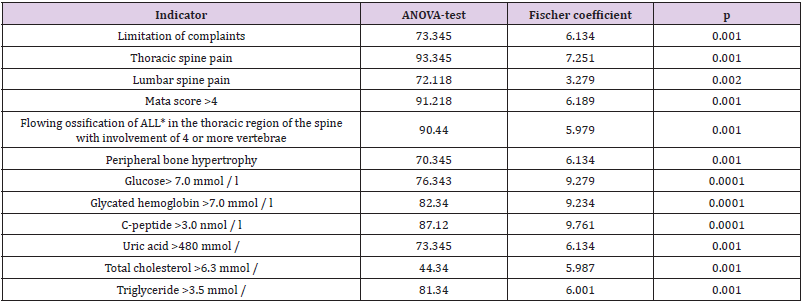
Table 4: Correlation relationships between Mata-score and some clinical findings and biochemical parameters (ANOVA-test and Fischer coefficient).
Discussion
The clinical diagnosis at the onset of the disease of DISH is difficult and sometimes impossible due to the lack of typical symptoms of the disease and characteristic imaging changes [18,28,41]. The disease is suspected in patients over 50 years of age, men who complain of prolonged diffuse back pain, in the area of various entheses, tendons, joints, bone edges and tubers, in normal or slightly altered routine laboratory tests [1-3]. This suspicion is exacerbated by the establishment of muscle rigidity and restriction of movement around the pain region. Sometimes the disease is painless [5,12,42] and is suspected in vague dysphagia, especially dry food and head strain, accompanied by dysphonia, dyspnoea, pre-existing myelopathy with quadriparesis or quadriplegia, cauda equina syndrome, palpation of bone thickening and spines, spine fractures with minimal trauma [43-48]. DISH can be suspected in the presence of various risk factors: obesity, elevated BMI, type II diabetes mellitus or impaired glucose tolerance, hypertension, gout (hyperuricemia), hyperinsulinemia, impaired lipid metabolism (increased cholesterol, triglycerides), fatty acids, etc. [2,5,10]. In case of any suspicion of the disease, it is necessary to provide a CR of the affected area and the middle and lower part of the thoracic spine, where usually the earliest characteristic radiological changes occur [49-52].
Nowadays, conventional radiography is the main method for diagnosing DISH and their complications in Bulgaria. The authors emphasize the characteristic changes in the CR of the axial and peripheral bone skeleton [50, 51]. CR proves hyperostosis on the edges and bodies of the vertebrae, flowing ossification of ALL, especially in the thoracic spine, the presence of characteristic vertically directed osteophytes, often with the formation of bone bridges, preserved intervertebral space, unaltered apophyseal and sacroiliac joints, characteristic changes in the peripheral skeleton and soft tissues around [7,14]. For the diagnosis of DISH, classification criteria are used based on the findings in the CR of spine, mostly those of Resnick et Niwayama, but they are valid in the advanced, late phase of the disease. The authors recommend looking for new criteria for this [2]. Osteoporosis was detected by DXA in 33.93% of patients with DISH, despite the fact that some authors reported increased or normal bone mineral density, which according to them was most likely due to the superimposition of the effect of ossified soft tissues around the studied bones [53,54].
Upon admission to a hospital in Bulgaria, all patients undergo routine tests, which include assessment of carbohydrate, protein and lipid metabolism. We believe that glucose’s contract values are> 7.0 mmol /l, glycated hemoglobin> 7.0 mmol/l, C-peptide> 3.0 nmol/l, uric acid> 480 mmol/L, total cholesterol> 6.3 mmol/L, triglyceride>3.5 mmol/L, will help doctors to detect the presence of Diffuse idiopathic skeletal hyperostosis and to refer patients for diagnosis and treatment. The study of the correlations between Mata’s score and some clinical and laboratory parameters studied by ANOVA-test and Fischer’s coefficient showed that there is a reliable relationship between the two groups of findings, which once again confirms the importance of Mata’s score and CR. After sequential analysis of 63 parameters of patients with DISH Mader, et al. [2] concluded that only 4 of them were admitted by multiple rheumatologists and orthopedic surgeons with consensus for the diagnosis of the disease: pronounced abundant (exuberant) formation of new bone, prolonged, enlarged bone bridges of the cervical spine, thoracic spine or lumbar spine [2]. Other manifestations (thoracic pain, shoulder pain, provoked rotator cuff pain, BMI>30, diabetes mellitus, hypertension, obesity) were not significantly accepted as diagnostic criteria [2]. This raises the question for discussion - if only pronounced bone changes are relevant for the diagnosis of DISH, and this occurs in an advanced, late phase of the disease, it is of little benefit to the patient and their attending physicians could not prevent the disease. In our study, we used routine DISH imaging methods. The changes detected by the CR of the spine, peripheral skeleton and soft tissues around it in patients with DISH correspond to the data of the authors [3-5,24]. We found calcification and ossification of the ALL, preserved intervertebral spaces, no degenerative changes of the disc, hyperostosis changes of the vertebrae, preserved apophyseal, costovertebral and sacroiliac joints. These changes are best expressed in the thoracic region and not coincidentally Mata et al. note that “Chest radiograph” is a screening test for DISH. Early diagnosis (which can be made 10 years before the full development of the disease) helps to recommend preventive measures for the underdevelopment of the disease [2], which is the goal of rheumatologists.
Conclusion
Our results described in detail the findings found in patients with Diffuse Idiopathic Skeletal Hyperostosis and demonstrated the benefits of using Mata’s score in the scoring of DISH. Significant correlations were found between CR results and biochemical data. We recommend that rheumatologists use Mata’s score in routine clinical practice to follow-up the patients.
References
- Belanger T, Rowe E (2001) Diffuse idiopathic skeletal hyperostosis: musculoskeletal manifestations. J Am Acad Orthop Surg 9(4): 258-267.
- Mader R, Verlaan J, Buskila D (2013) Diffuse idiopathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nat Rev Rheumatol 9(12): 741-750.
- Bakker J, Kuperus J, Kuijf H, Oncer FC, Jong PAD, et al. (2017) Morphological characteristics of diffuse idiopathic skeletal hyperostosis in the cervical spine. PLoS One 12(11): e0188414.
- Westerveld A, Van Ufford HME, Verlaan JJ, Oncer FC (2008) The prevalence of diffuse idiopathic skeletal hyperostosis in an outpatient population in the Netherlands. J Rheumatol 35(8): 1635-1638.
- Smith J, Littlejohn G (1994) Diffuse idiopathic skeletal hyperostosis. In: Klipper J, Dieppe PA (Eds.)., Rheumatology (Edn.)., pp. 7.9.1. -7.9.6.
- Hukuda S, Mochizuki T, Ogata M, Shichikawa K (1983) The pattern of spinal and extraspinal hyperostosis in patients with ossification of the posterior longitudinal ligament and the ligamentum flavum causing myelopathy. Skeletal Radiol 10(2): 79-85.
- Beyeler C, Schlapbach P, Gerber N, Sturzenegger J, Fahrer H, et al. (1990) Diffuse idiopathic skeletal hyperostosis (DISH) of the shoulder: a cause of shoulder pain? Br J Rheumatol 29(5): 349-353.
- Resnick D, Shapiro RF, Wiesner KB, Niwayama G, Utsinger PD, et al. (1978) Diffuse idiopathic skeletal hyperostosis (DISH) [ankylosing hyperostosis of Forestier and Rotes-Ouerol, Semin Arthritis Rheum 7(3): 153-187.
- Forestier J, Lagier R (1971) Ankylosing hyperostosis of the spine. Clin Orthop Rel Res 74: 65-83.
- Forestier J, Rotes-Querol J (1950) Senile ankylosing hyperostosis of the spine. Ann Rheum Dis 9(4): 321-330.
- Baraliakos X, Listing J, Buschmann J, Recke AVD, Braun J (2011) Comparing new bone formation in ankylosing spondylitis and diffuse diffuse idiopathic skeletal hyperostosis patients - a retrospective cohort study over 6 years. Arthritis Rheum 64(4): 1127-1133.
- Kuperus J, De Gendt EA, Oner F, Jong PAD, Buckens SCF M, et al. (2017) Classification criteria for diffuse idiopathic skeletal hyperostosis: a lack of consensus. Rheumatology 56(7): 1123-1134.
- Cammisa M, Serie AD, Guglillmi G (1998) Diffuse idiopathic skeletal hyperostosis. Eur J Radiol 27(1): 7-11.
- Quagliano P, Hayes C, Palmer W (1994) Vertebral pseudoarthrosis associated with diffuse idiopathic skeletal hyperostosis. Skeletal Radiol 23(5): 353-355.
- Resnick D, Niwayama G (1976) Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 119(3): 559-568.
- Resnick D, Guerra J, Robinson C, Vint VC (1978) Association of diffuse idiopathic skeletal hyperostosis (DISH) and calcification and ossification of the posterior longitudinal ligament. AJR Am J Roentgenol 131(6): 1049-1053.
- Littlejohn G, Urowitz M (1982) Peripheral entesopathies in diffuse idiopathic skeletal hyperostosis (DISH). J Radioilogy 9(4): 569-579.
- Sarzi-Puttini P, Atzeni F (2004) New developments in our understanding of DISH (Diffuse idiopathic skeletal hyperostosis). Curr Opin Rheumat 16(3): 287-292.
- Kuperus J, Oudkerk S, Foppen W, Mohamed Hoesein FA, Gielis WP, et al. (2019) Criteria for Early-Phase Diffuse Idiopathic Skeletal Hyperostosis: Development and Validation. Radiology 291(2): 420-426.
- Ehara S, Shimamura T, Nakamura R, Yamazaki K (1998) Paravertebral ligamentous ossification: DISH, OPLL and OLF. Eur J Radiol 27(3): 196-205.
- Ono K, Yonenobo K, Miyamoto S, Okada K (1999) Pathalogy of ossification of the posterior longitudinal ligamentr and ligamentum flavum. Clin Orthop Rel Res 359: 18-26.
- De Peretti F, Sane J, Dran G, Razafindratsiva C, Argenson C (2004) Ankylosed spine fractures with spondylitis or diffuse idiopathic skeletal hyperostosis: diagnosis and complications [in French]. Rev Chir Orthop Repar Appar Mot 90(5): 456-465.
- Diederichs G, Engelken F, Marshall L, Peters K, Black DM, et al. (2011) Diffuse idiopathic skeletal hyperostosis (DISH): relation to vertebral fractures and bone density. Osteoporos Int 22(6): 1789-1797.
- Childs S (2004) Diffuse idiopathic skeletal hyperostosis. Forestier’s disease. Orthopaedic Nursing 33(6): 375-382.
- Chiba H, Annen S, Shimada T, Imuraq S (1992) Atlantoaxial subluxation complicated by diffuse idiopathic skeletal hyperostosis: a case report. Spine 17(11): 1414-1417.
- Dar G, Peleg S, Masharawi Y, Steinberg N, Rothschild BM, et al. (2007) The association of sacroiliac joint bridging with other enthesopathies in the human body. Spine 32(10): E303-E308.
- Colina M, Govoni M, De Leonardis F, Trotta F (2006) La iperostosiscelentri-caidipatica diffusa (D.I.S.H.). Rheumatismo 58(2): 104-111.
- Haller J, Resnick D, Miller C, Schils JP, Kerr R, et al. (1989) Diffuse idiopathic skeletal hyperostosis: diagnostic significance of radiographic abnormalities of the pelvis. Radiology 172(3): 835-839.
- Gonzalez-Beicos A, Nuñez D, Fung A, Sanchez M, Gahbauer H (2007) Trauma to the ankylotic spine: imaging spectrum of vertebral and soft tissue injuries. Emerg Radiol 14(6): 371-378.
- Giger R, Dulguerov P, Payer M (2006) Anterior cervical osteophytes causing dysphagia and dyspnea: an uncommon entity revisited. Dysphagia 21(4): 259-263.
- Battaglia M, Zompatori M, Nassetti C, Rimondi MR, Sciascia N (1996) An unusual cause of nocturnal orthopnea: Forestier's cervical hyperostosis spondylopathy. Radiol Med (Torino) 92(1-2): 135-137.
- Mader R (2004) Diffuse idiopathic skeletal hyperostosis: isolated involment of cervicalk spine in a young patient. J Rheumatol 31(3): 620-621.
- Nakhoda K, Chew F (2011) Imaging in DISH (diffus idiopathic skeletal hyperostosis. Medscape, pp. 388-973.
- Hendrix R, Melany M, Miller F, Rogers L (1994) Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR 162(4): 899-904.
- Olivieri I, D'Angelo S, Cutro M, Padula A, Peruz G, et al. (2007) Diffuse idiopathic skeletal hyperostosis may give the typical postural abnormalities of advanced ankylosing spondylitis. Rheumatology 46(11): 1709-1711.
- Julkunen H, Heinonen O, Knekt P, Matela J (1975) The epidemiology of hyperostosis of the spine together with symptoms and related mortality in general population. Scand J Rheumat 4(1): 23-29.
- Utsinger P, Resnick D, Shapiro R (1976) Diffuse skeletal abnormalities in Forestier's disease. Arch Intern Med 136(7): 763-768.
- Utsinger P (1985) Diffuse idiopathic skeletal hyperostosis. Clin Rheum Dis 11: 325-351.
- Mata S, Hill R, Kaplan P, Dussault R, Watts CS, et al. (1993) Chest radiographs as a screening test for diffuse idiopathic skeletal hyperostosis. J Rheumatol 20(11): 1905-1910.
- Mata S, Chem R, Fortin P, Joseph L, Esdaile JM (1998) Comprehensive radiographic evaluation of diffuse idioipathic skeletal hyperostosis: development and interrater reliability of a scoring system. Semin Arthritis Rheumatol 28(2): 88-96.
- Kim S, Choi B, Kim C (2004) The prevalens of diffuse idiopathic skeletal hyperostosis in Koree. J Rheumatology 31(10): 2032-2035.
- Strohm P, Zwingmann J, Bley T, Kostler W, Sudkamp NP (2006) Injuries of the cervical spine with Forestier's disease: problems in the diagnostic and surgical management. Unfallchirurg 109(10): 905-909.
- Callahan E, Aguillera H (1993) Complications following minor trauma in a patient with diffuse idiopathic skeletal hyperostosis. Ann Emerg Med 22(6): 1067-1070.
- Eser P, Bonel H, Seitz M, Villiger PM, Aeberli D (2010) Patients with diffuse idiopathic skeletal hyperostosis do not have increased bone mineral density. Rheumatology 49(5): 977-981.
- Olivieri I, D'angelo S, Palazzi C, Padula A, Mader R, et al. (2009) Diffuse idiopathic skeletal hyperostosis: differentiation from ankylosing spondylitis. Curr Rheumatol Rep 11(5): 321-328.
- Paley D, Schwartz M, Cooper P, Harris WR, Levine AM (1991) Fractures of the spine in diffuse idiopathic skeletal hyperostosis. Clin Orthop Relat Res 267: 22-32.
- Le Hir P, Sautet A, Le Gars L, Zeitoun F, Tubiana JM, et al. (1999) Hyperextension vertebral body fractures in diffuse idiopathic skeletal hyperostosis: a cause of intravertebral fluidlike collections on MR imaging. AJR 173(6): 1679-1683.
- Sreedharan S, Li Y (2005) Diffuse idiopathic skeletal hyperostosis with cervical spinal cord injury: a report of 3 cases and a literature review. Ann Acad Med Singapore 34(3): 257-261.
- Robinson P, Wordworth B, Reveille J, Broun M (2013) Axial spondyloarthritis: a new disease entity, not nesessarily early ankylosing spondylitis. ARD 72(2): 162-164.
- Rao S, Wasyliw C, Nunez DB (2005) Spectrum of imaging findings in hyperextension injuries of the neck. Radio Graphics 25(5): 1239-1254.
- Tsukamoto Y, Onitsuka H, Lee K (1977) Radiologic aspects of diffuse idiopathic skeletal hyperostosis in the spine. AJR Am J Roentgenol 129(5): 913-918.
- Taljanovic M, Hunter T, Wisneski R, Seeger JF, Friend CJ, et al. (2009) Imaging characteristics of diffuse idiopathic skeletal hyperostosis with an emphasis on acute spinal fractures: review. AJR Am J Roentgenol 193(3): S10-S19.
- Westerveld L, Verlaan J, Lam MGE H, Scholten WP, Bleys RLA W, et al. (2009) The influence of diffuse idiopathic skeletal hyperostosis on bone mineral density measurement of the spine. Rheumatology 48(9): 1133-1136.
- Gregson C, Hardcastele S, Cooper C, Tobias JH (2013) Frend or foe: high bone mineral density on routine bone density scaning (DXA), a review of causes and menаgiment. Rheumatology 52(6): 968-985.
