 Mini Review
Mini ReviewABSTRACT
Purpose: Determine if gender differences exist in static and dynamic testing.
Design: Three hundred subjects, 173 males (29.1+13.7 Yrs) and 127 (31.5+14.6 Yrs) females, were administered a battery of 5 balance tests, 3 static and 2 dynamic tests.
Analysis: Mann-Whitney non-parametric and one-way ANOVA parametric tests were used to analyze the balance results comparisons between the two groups.
Results: Non-parametric Mann-Whitney results indicated significant superior static balance of males in both the dominant and non-dominant leg of the Stork test; and significant superior dynamic balance of males for the 5 Times Sit-to-Stand test.
Keywords: Balance; Stability; Static and Dynamic Balance; Coordination
Introduction
The need for mobility while maintaining stability is essential in everyday life. Programs have been developed to improve a subject’s stability and mobility through balance exercise programs that provide physical conditioning to major muscles used in specific movements and condition their associated stabilizing muscles [1]. A subject’s balance can be improved no matter the status of the subject [2]. As is the case for any conditioning program, assessments must be administered before a suitable program can be developed for the subject in question [3]. The ability to maintain control of body movement or to stay upright is called balance. There is static balance, and there is dynamic balance. Static balance is maintaining equilibrium when stationary while dynamic balance is maintaining equilibrium when moving. Eyes, ears, physical conditioning, and proprioception are used to help sustain balance [4].
Unique physiological gender differences exist to perform unique tasks efficiently, like childbirth. For example, women’s hips are generally larger than men. The reason for this is to facilitate giving birth. The wider hips also present a greater lateral force on the knee articulation (A greater Q angle), especially when they move laterally in an explosive manner [5]. This puts women at a greater risk for anterior cruciate ligament injury [6]. This structural deviation can cause different outcomes while performing the same task. That being the case, one must question if different gender physiology can also cause different balance outcomes. The purpose of this study is to determine if gender differences significantly affect balance appraisal results.
Design
Three hundred subjects, 173 males and 127 females, were administered a battery of 5 balance tests, 3 static tests and 2 dynamic tests. See Table 1 for the subjects’ physical characteristics. The IRB approved study consisted of a convenience sample of 300 subjects. Prior to administering the battery of tests, the subjects were informed of the battery of tests that were to be performed, the description of the tests, and that the subjects could stop at any time during the tests. The subjects signed a consent form prior to the beginning of testing. The tests were conducted by University of New Orleans exercise physiology undergraduate students who were CITI-certified for Human Subjects Testing and trained to administer the battery of balance tests. The battery of tests administered to the subjects consisted of the following tests. Brief descriptions of the tests are also included [4,7-11]:

Table 1: Physical Characteristics.
One-Leg Standing Balance Static Test (Right and Left Leg)
Stand on 1 leg without holding onto anything. Normal balance is one minute, less than 30 seconds will need some work.
Stork Balance Static Test (Right and Left Leg)
Place the hands on the hips, position the non-supporting foot against the inside knee of the supporting leg. The subject raises the heel to balance on the ball of the foot. The stopwatch is started as the heel is raised from the floor. The stopwatch is stopped if the hand(s) come off the hips, the supporting foot swivels or moves (hops) in any direction, the non-supporting foot loses contact with the knee, or the heel of the supporting foot touches the floor. Average time is 25 - 39 seconds. Poor is less than 10 seconds.
Timed Up-and-Go Dynamic Test
A chair is placed against a wall and a spot is measured and marked ten feet from the chair. The test is how long it takes to get up out of the chair, walk 10 feet, turn around, and sit back down. If it takes longer than 14 seconds, there is a high risk for falling.
The 5 Times Sit-to-Stand Dynamic Test
Sit in a chair. Whenever ready, stand up and down 5 complete times as fast as possible. Stand fully and sit down with the glutes touching the chair. Persons without balance problems can do this test in less than 13 seconds.
The Balance Error Scoring System Static Test [12]
There are six positions of the balance error scoring system static test. Three stances (double-leg support, single-leg support, and tandem) are held for 20 seconds on two surfaces (firm floor and foam pad) for six permutations. During the tandem stance, the dominant foot is in front of the nondominant foot. During the single-leg stance, the subject stands on the nondominant foot. During the test, the eyes are closed and the hands are held on the hips (iliac crests).
Subjects are told to keep as steady as possible, and if they lose their balance, they are to try to regain the initial position as quickly as possible. Subjects are assessed one point for the following errors: lifting the hands off the iliac crests; opening the eyes; stepping, stumbling, or falling; remaining out of the test position for five seconds; moving the hip into more than 30° of hip flexion or abduction; or lifting the forefoot or heel [6]. A trial is considered incomplete if the subject cannot hold the position without error for at least five seconds. The maximal number of errors per condition is 10. An incomplete condition is given the maximal number of points (10). The numbers of errors for all six conditions are summed into a single score. For example, ages 20-39 years, mean + SD=10.97+5.05 errors; 50-54 years, mean + SD=12.73 + 6.07 errors; and 65-69 years, mean + SD=20.38+7.78 errors.
Analysis
One-way analysis of variance (ANOVA) tests from the IBM Statistical Program for Social Sciences (SPSS) version 24 were used to compare the scores of the male subjects versus the scores of the female subjects. Levene’s tests were used to validate the comparisons of the data. If the Levene tests validated the homogeneity of the variances of the gender groups, One-Way ANOVA parametric analysis were used. The Mann-Whitney non-parametric tests were used to analyze the tests that were not validated by Levene’s homogeneity tests. The level of significance was set at 0.05. Pearson correlations were used to investigate any significant relationships between the balance tests and anthropomorphic variables.
Results
Levene’s homogeneity tests did not validate the results of the 5 balance tests. Because the parametric one-way ANOVA results were not validated for the balance tests, non-parametric Mann-Whitney tests were applied to analyze the results of the balance tests. The non-parametric results indicated that the males’ balance results times in the 5 Times Sit-to-Stand tests were significantly faster than the females’ balance results times in the same test; and the males’ Stork balance time results, in both the right and left leg, were significantly longer than the same balance time test results of the females. See Table 2 for the non-parametric results.
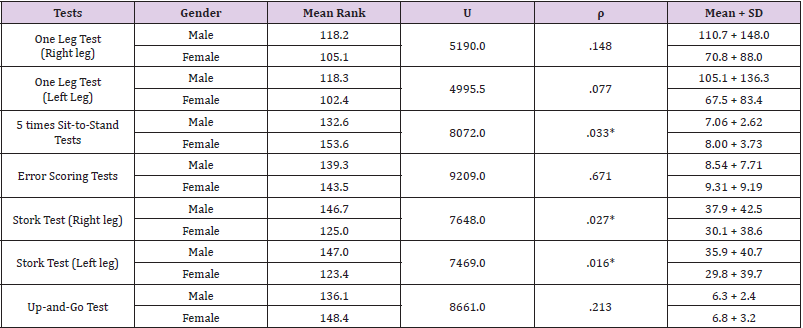
Table 2: Mann-Whitney Ranking Results.
*- Significant, Level of Significance ρ = 0.05
Discussion
The study revealed that the males in the study displayed significantly superior dynamic balance in the Five Times Sit and Stand test and significant superior static balance in the Stork test in both the dominant and non-dominant leg as compared to females in those studies. The males scored better in comparing the remaining dynamic test (Up and Go test) and the two static tests (One-leg tests and Error tests), but they were not significant. How can a subject score significant changes in one static balance test and not in another? Each test in the 5-test balance battery measures a different component of balance, and the differences in these tests provide an in-depth analysis about the balance components of the subject. The one-leg tests measure unipedal balance like the stork tests, but the one-leg tests allow the subjects to use the non-supporting leg, the upper appendages, and the torso to move and contort to maintain static unipedal balance. The stork tests also measure unipedal static balance, but they restrict the subjects from using their nonsupporting leg, their appendages, and/or their torso to assist them in maintaining their static balance. So, the subjects that display better proprioception and body coordination in the one-leg tests are at an advantage to those that do not. While the error scoring tests are also restrictive, only 2 of the six components of the test measure unipedal static balance, the remaining 4 measure bipedal static balance. The error scoring tests measure static balance in different orientation planes on different surfaces [13].
It would appear from the data that static or dynamic balance is not significantly dependent upon basic anthropomorphic variables alone. Two ways to improve the stability of a subject is to lower the subject’s center of gravity closer to his/her base and to increase the weight of the subject over its base. If there were strong negative associations regarding height, then that would favor females because, as a group, females are shorter than males; and if there were strong positive associations regarding weight that would favor males because, as a group, males are heavier than females. Neither of these anthropomorphic variables strongly correlated with balance. Pearson correlations of the balance results from the current study revealed weak associations between weight, height, and BMI (Body Mass Index). The current data also suggests that as subjects age balance will begin to wane. See Table 3.

Table 3: Anthropomorphic Pearson Correlations (ρ).
The 5 times sit-to-stand test measures the explosiveness of dynamic balance. The better dynamic balance of the males in the study could possibly be attributed to improved strength, agility, flexibility, and coordination due to increased training and conditioning. The Stork test measures restricted unipedal static balance. The study results could be indicative of the males in the study demonstrating better proprioception and body coordination. It may also be indicative of better conditioning of the males’ stabilizer muscles. Increasing the number of subjects in the convenience sample could improve the variances of the test subgroups, resulting in the Levene homogeneity test values validating the one-way ANOVA comparisons for the balance test battery. The parametric one-way ANOVA test is a much more sensitive test than the nonparametric Mann-Whitney test.
Conclusion
The study does not definitively demonstrate gender balance differences, but the resultant data sufficiently warrants the need for further investigation. The authors recommend additional testing to verify the results obtained from the study; and to secure larger samples that would include parametric analyses of all 5 balance tests used in the current study for a deeper insight into the balance skills regarding gender differences.
Acknowledgements
The authors would like to thank the certified UNO exercise physiology majors who participated as testers in this motor learning balance study. No grant or outside funding was provided for this project.
References
- Johnson B, Nelson J (1979) Practical measurements for evaluation in physical education. 4th (Edn.), Minneapolis: Burgess.
- Sackley S, Gladman J (1998) The evidence for rehabilitation after severely disabling stroke. Phys Ther Rev 3(1): 19-29.
- Streiner D, Norman G (1995) Health measurement scales: a practical guide to their development and use. 2nd (Edn). Oxford: Oxford Medical Publications.
- Miller T (2012) NSCA’s guide to tests and assessments. Champaign, IL: Human Kinetics.
- Heiderscheit B, Hamill J, Caldwell G (2000) Influence of Q-angle on lower-extremity running kinematics-Part 1. J Orthop Sports Phys Ther 30(5): 271-278.
- Hewitt T, Myer G, Ford K (2006) Anterior cruciate ligament injuries in female athletes Part 1, Mechanisms and Risk Factors. Sage 34(2).
- Collen F, Wade D, Bradshaw C (1990) Mobility after stroke; reliability of measures of impairment and disability. Int Disabil Stud 12(1): 6-9.
- Riemann B, Guskiewicz K, Shields E (1999) Relationship between clinical and force plate measures of postural stability. Sport Rehabilitation 8(2): 71-82.
- Goldie P, Matyas T, Spencer K, McGinley R (1990) Postural control in standing following stroke; test-retest reliability of some quantitative clinical tests. Phys Ther 70: 234-243.
- Bohannon R, Larkin P, Cook A, Gear J, Singer J (1984) Decrease in Timed Balance Test Scores with Aging Physical Therapy 64(7): 1067- 1070.
- Giorgetti M, Harris B, Jette A (1998) Reliability of clinical balance outcome measures in the elderly. Physiother Res Int 3(4): 274-283.
- Iverson G, Kaarto M, Koehle M (2008) Normative data for the balance error scoring system: Implications for brain injury evaluation. Brain Injury 22(8): 147-152.
- Bonis M, Tillery K (2021) Do collegiate athletes display better balance skills than their non-athlete counterparts? Biomed J Sci & Tech Res 34(4).
