 Review Article
Review ArticleAbstract
Angioleiomyoma (ALM) is a rare benign, vascular smooth muscle tumor originating from the tunica media of the vessel wall. It typically arises in the cutaneous, subcutaneous tissue of the lower extremities in middle-aged women. In this article, the author will review the characteristic vascular status of subtype of ALM on color and power Doppler US along with magnetic resonance imaging (MRI) appearances. Given the occurrence location, close to or in contact with dermis, it is strongly suggested that angioleiomyoma may contain vessel components in the tumor. It is plausible that estimations of vascular pattern, density, distribution, and spectral Doppler analysis on high-resolution ultrasonography (US) contribute to make an accurate diagnosis of the subtype of ALM. In solid (or capillary) subtype, little vascularity and adjacent vascular features on color and power Doppler US and enhancing structures on one or both ends of the mass on MRI may be the potential diagnostic findings.
Keywords: Subtype of Angioleiomyoma; Adjacent Vessel; Painful and Vascular Superficial Tumor; Color and Power Doppler Ultrasonography; MRI Appearance
Abbreviations: MRI: Magnetic Resonance Imajing (MRI);INF: Intradermal Nodular Fasciitis;RTE: Real-Time Tissue Elastography; STIR:Short Tau Inversion Recovery
Introduction
ALM is a rare tumor that arises from the tunica media of small arteries and veins [1]. ALM typically occurs in the cutaneous, subcutaneous tissue of the lower extremities in middle-aged women. Histological appearances show a proliferation of smooth muscle cells and vascular channels and the classification into three histological subtypes such as solid (or capillary), cavernous, and venous types has been defined [1]. The author has previously described the solid (or capillary) subtype of ALM as a painful and vascularized subcutaneous tumor, probably in close to the dermis [2] and indicated that all painful cutaneous and subcutaneous tumors including ALM used as the acronym “ENGLAND” or “LEND an EGG”[3], especially, angioleiomyoma, eccrine spiradenoma, schwannoma, and glomus tumor show vascularlized appearances on high-resolution color Doppler US [4]. Recently, US findings of ALM based on pathologic subtypes have been described [5] and Kang et al. [6] have reported ALM findings on US and MRI. In this article, the current knowledge of the characteristic vascular status of subtype of subcutaneous ALM on color and power Doppler US along with MRI appearances will be reviewed.
Ultrasound in Dermatology
The international working group, namely DERMUS (Dermatologic Ultrasound) provided the guidelines [7] and proposed for an assessment training program [8]. A 15 MHz is the minimum frequency recommended for performing dermatologic examination by DERMUS [7, 8]. Hwang et al. [9] have reported the diagnostic value of gray-scale and color Doppler ultrasonography (US) with 5-15 MHz probe in benign subcutaneous lesions. The author usually performs US studies for dermatologic fields with a high-resolution, broad-band (5MHz-18MHz) linear transducer (Nobulus Hitachi, Ltd.Tokyo, Japan) and described knowledge including ALM reports and several studies in the dermatologic area [2, 4, 10-20].
Angioleiomyoma
Cutaneous leiomyoma are benign smooth muscle neoplasms that comprise three types such as piloleiomyoma, angioleiomyoma (ALM), and genital leiomyoma [21]. ALM is a rare tumor that arises from the tunica media of small arteries and veins and clinically represents a solitary, firm, well-circumscribed tumor measuring less than 20 mm in size [1]. Histological appearances show a proliferation of smooth muscle cells and vascular channels. Based on the size of the vascular channel and the degree of muscular thickness, the classification into three histological subtypes such as solid (or capillary), cavernous, and venous types has been defined. The solid (or capillary) subtype of ALM generally represents a painful nodule on the limbs and occurs more frequently in females, whereas venous subtype tends to occur on the head and neck location in male [1]. The report indicated that the etiology of the pain may be caused by the local tissue anoxia or to compression of the nerves by the nodule [1]. It has been also hypothesized that muscle contraction may be central to the induction of pain [21]. The ALM on the auricle is frequently painless [22, 23]. The author has previously described the solid (or capillary) subtype of ALM as a painful and vascularized subcutaneous tumor, probably in close to the dermis [7] and indicated that all painful cutaneous and subcutaneous tumors used as the acronym “ENGLAND” or “LEND AN EGG” [3], especially, angioleiomyoma, eccrine spiradenoma, schwannoma, and glomus tumor show vascularlized appearances on high-resolution color Doppler US [4].
Gray-Scale and Color Doppler US Features
US features of ALM have been reported as an oval shape, well-demarcated margin, homogeneously hypoechoic nodule with moderate or rich vascularity status [24-26]. Park et al. [26] mentioned that gray-scale US features represent a homogeneous hypoechoic mass with a well-defined margin and there are 3 categories of vasculature patterns including type 1 representing several clustered linear vessels that converge to a single point, type 2 showing scattered distribution of irregular vessels, and type 3 presenting as 1 or more vessels that are centrally located on color Doppler US. In addition, vascularity is further classified as little (covering less than 20% of the mass), moderate (20%^50%), and rich (covering more than 50% of the mass) status. They suggested that the most commonly detected vascular pattern was type 1 with moderate vascular density. Zhang et al. [27] mentioned that US appearances of ALM as subcutaneous nodule, especially in contact with the dermis, a small size less than 20 mm, an oval shape, solid, homogeneously hypoechoic pattern and low or moderate vascular density was seen on color Doppler US.
They noted that 75.8% of subcutaneous ALM was in a superficial location, close to or in contact with the dermis [27]. The author previously mentioned that intradermal nodular fasciitis represents vascular components on color Doppler US due to rich capillary vessels of dermis in histology [11, 12, 17]. Similar to intradermal nodular fasciitis (INF), as ALMs tend to occur in the subcutaneous layer, close to or in contact with dermis which contains rich capillary vessels, they show the vascular features on color Doppler US. Kim et al. [5] have described the relationship between US appearances and pathologic features of subtypes in the subcutaneous angioleiomyoma in the extremities. Both venous and cavernous subtypes on gray-scale US appear as welldefined, homogeneously hypoechoic tumor, while capillary type shows well-defined, homogeneously isoechoic mass similar to the muscle. Concerning to the color Doppler appearances, cavernous ALM represents abundant vascular flow accompanied with several feeding vessels reflecting the pathology of the dilated vascular channels with minimal smooth muscle. Venous subtype represents moderate vascular flow signal accompanied with several feeding vessels representing pathologically non-compacted smooth muscle bundles and vascular channels with thick muscular walls, whereas capillary type shows little vascular flow signal with linear feeding vessels reflecting pathologically scattered small, slit-like vascular channels surrounded by numerous compacted smooth muscle bundles [5].
Given the studies in the literature, the most of ALM are venous and capillary type. The report by Kim et al. [5] suggested that capillary type is likely to show isoechoic similar to the muscle with little vascular status on gray-scale and color Doppler US due to the collapse of intratumoral vessels and a higher proportion of smooth muscle components in the mass. On the contrary, venous type is more likely to represent hypoechoic and hypervascular pattern caused by internal, thick, muscularly walled-vessels and the preservation of the vessel lumen [5]. While, Kang et al. [26] described the findings of the ALM on US and MRI and indicated the enhancement of the protruding structure from one or both ends, suggesting probably adjacent vessel on enhanced MRI. Recently, the author reported a solid (or capillary )subtype of ALM using high-resolution ultrasound including gray-scale US, power Doppler US, and Real-Time Tissue Elastography (RTE) and described that vascular flow signals were observed at central and peripheral portions on power Doppler US and Fine Flow, suggesting a solid (or capillary) type of ALM [2]. An oval shape, well-defined, homogeneously hypoechoic nodule without posterior echo enhancement on gray-scale US and hard nature on RTE also represent solid tumor reflecting pathologically numerous compacted smooth muscle bundles with scattered small, slit-like vascular channels in solid (or capillary) subtype [2]. In addition, the evaluation of spectral Doppler analysis for previous case showed low blood flow velocity suggesting benign type [2].
Due to the development of high-resolution multifrequency transducers and multichannel color Doppler apparatus, it will be possible to make an accurate diagnosis of subtype of ALM on US. The author suggests that with respect to the color Doppler appearance, the rich vascularity status may be consistent with cavernous type, moderate vascularity feature may correspond to venous type, and little flow in central and adjacent flow in periphery appearances may be consistent with solid (or capillary) type. In addition, although extradigital glomus tumors represent high speed and high resistance profile on spectral Doppler analysis [28], spectral Doppler analysis for blood flow velocity is very important in differential diagnosis between benign and malignant lesion. Central and peripheral blood flow signals were detected on Fine Flow in ALM on the lower extremity pathologically confirmed in a 69-year-old female (Figure 1). Little flow in central and adjacent flow in periphery were observed on power Doppler US. Peripheral flow on power Doppler US was suggested to correspond to adjacent vessel (Figure 2).
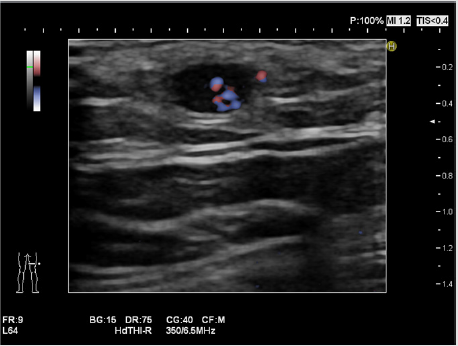
Figure 1: Angioleiomyoma on the lower extremity in a 69-year-old female. Central and peripheral blood flow signals were detected on Fine Flow.

Figure 2: Little flow signal in central and adjacent flow signal in periphery were detected on power Doppler US. Peripheral flow signal on power Doppler US was suggested to be consistent with the adjacent vessel.
Magnetic Resonance Imaging Features
Some reports described that the MRI appearances of ALM have been observed as a well-circumscribed mass with an isointense or slightly high signal intensity relative to the muscle on T1-weighted images and a heterogeneous and high signal intensity on T2- weighted and STIR images [29, 30]. With respect to the study of the correlation between subtype MRI findings and pathological features, a few reports have been studied [29, 31]. Hwang et al. [31] could not differentiate between the different subtypes in ALM on MRI appearances. Gupte et al. [29] described that MRI findings were not able to differentiate between the different histological subtypes in ALM. Yoo et al. [30] noted that ALM should be regarded as a possible diagnosis when a well-demarcated subcutaneous mass of isointense signal on T1-weighted image, heterogeneous high signal intensity on T2-weighted images with homogeneous enhancement, and an adjacent tortuous vascular structure are observed on the extremities. Kumar et al. [32] mentioned that diffuse homogeneous enhancement of the mass lesion with a vessel converging on the superior pole of the mass lesion was shown on postcontrast fat suppressed T1-weighted images. Neurogenic tumors generally represent well-demarcated masses of high signal intensity on T2- weighted image without a tortuous vascular structure. Maura et al. [33] described that an intramuscular ALM shows iso signal intensity (SI) to muscle on T1W1 and high signal intensity on T2/STIR (short tau inversion recovery) with a T2 hypointense rim. Kang et al. [6] described that slightly high signal intensity on T1-weighted image, a heterogeneous and high signal intensity on T2-weighted and STIR images, and heterogeneous enhancement on enhanced T1-weighted image were shown. In addition, enhancing structures on one or both ends of the mass on MRI has been reported. Differential diagnosis of ALM can include vascularized superficial benign soft-tissue tumors ultrasonographically regarded as eccrine spiradenoma, dermatofibroma, schwannoma, vascular leiomyoma, glomus tumor, pilomatricoma, chondroid syringoma, hemangioma [34]. Especially, neurogenic tumors mimic angioleiomyoma representing well-defined hypoechoic oval mass with internal vascularity on US. However, they show the characteristic finding of connection to a nerve namely eccentric type of the nerve-tumor position [32]. Reynolds et al. suggested that schwannoma have been classically described as eccentric at both MRI and histology [34]. Lee et al. [35] described that peripheral nerve sheath tumor (PNST) such as schwannomas and neurofibromas shows isointese SI with muscle on TIWI and T2W1 represents heterogeneously hyperintense SI than muscle. Enhancement pattern was heterogeneous [35]. As it is also important to differentiate between ALM and giant cell tumor of the tendon sheath (GCTTS), the author previously mentioned the characteristic appearances of GCTTS on US and MRI [20,36]. It is suggested that US study shows hypoechoic nodule with vascularity and low signal intensity on T1 and T2 weighted MR images due to the hemosiderin were observed in GCTTS [20,37].
Conclusion
Given the occurrence location, close to or in contact with dermis, it is strongly suggested that angioleiomyoma may contain vessel components in the tumor.
It is plausible that estimations of vascular pattern, density, distribution, and spectral Doppler analysis on high-resolution ultrasonography contribute to make an accurate diagnosis of the subtype of angioleiomyoma.
In solid (or capillary) subtype, little vascularity and adjacent vessel features on color and power Doppler Ultrasonography and enhancing structures on one or both ends of the mass on magnetic resonance imaging may be a potential diagnostic findings.
Acknowledgement
The author appreciates Dr. Akira Fujioka, Dr. Minoru Oishi, Dr. Ken Hayashi, and Dr. Masahiro Okada for their kind support.
Conflicts of Interest
The author declares that I have no conflicts of interest.
References
- Tejasvl BR, Pai K, Rao R (2014) Painful nodule on the leg. Clin Exp Dermatol 39: 542-543.
- Fujioka K, Fujioka A, Oishi M, Hayashi K, Nakayama T (2018) High-resolution ultrasound imaging for angioleiomyoma: a painful and vascularized superficial tumor. Biomed J Sci & Tec Res 9(5).
- Naversen DN, Trask DM, Watson FH, Burket JM (1993) Painful tumors of the skin: “LEND AN EGG” J Am Acad Dermatol 28: 298-300.
- Fujioka K (2019) Painful cutaneous and subcutaneous tumors accompanied with vascularized appearance using high-resolution ultrasound in dermatology: the acronym “ENGLAND” or “LEND AN EGG”. Biomed J Sci & Tec Res 12(4).
- Kim DG, Lee SJ, Choo HJ, Kim SK, Cha JG, et al. (2019) Ultrasoongrapihc findings of subcutaneous angioleiomyomas in the extremities based on pathologic subtypes. Korean J Radiol 19: 752-757.
- Kang BS, Shin HS, Kim JH, Kim YM, Bang M, et al. (2019) Angioleiomyoma of the extremities: findings on ultrasonography and magnetic resonance imaging. J Ultrasound Med 38: 1201-1208.
- Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Martorell A, et al. (2016) Guidelines for performing dermatologic ultrasound examinations by the DERMUS group. J Ultrasound Med 35: 577-580.
- Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Martorell A, et al. (2016) Proposal for an assessment training program in dermatologic ultrasound by the DERMUS group. J Ultrasound Med 35: 2305-2309.
- Hwang EJ, Yoon HS, Cho S, Park HS (2015) The diagnostic value of ultrasonography with 5-15 MHz probes in benign subcutaneous lesions. Int J Dermatol 54: e469-75.
- Fujioka K, Fujioka A, Eto H, Suzuki K, Sanuki E, et al. (2006) Nodular fascitis in the thigh followed up using ultrasonography. J Med Ultrason 33: 49-53.
- Fujioka K, Fujioka A, Oishi M, Eto H, Tajima S, et al. (2017) Ultrasonography findings of intradermal nodular fasciitis: a rare case report and review of the literature. Clin Exp Dermatol 42: 335-336.
- Fujioka K, Fujioka A, Tajima S, Oishi M, Hayashi K, et al. (2018) Characteristic power Doppler sonographic imaging of nodular fasciitis from a dermatological perspective: another case and review of three cases. J Clin Case Rep 8: 1165.
- Fujioka K (2018) Presentations of clinical, ultrasonographic and pathological features of nodular fasciitis from an established cytogenetic viewpoints: review of the case series. J Carcinog Mutagen 9: 326.
- Fujioka K (2018) Usefulness of comprehensive high-resolution ultrasound imaging in dermatologic field: epidermal cyst. Biomed J Sci & Tec Res 12(1).
- Fujioka K (2019) Real- time Tissue elastography in epidermal cyst: along with enhanced MRI and elasticity features of peripheral rim. Biomed J Sci & Tec Res 16(5).
- Fujioka K (2019) A comparison between superficial and deep-seated lipomas on high-resolution ultrasonography: with RTE and MRI appearances. Biomed J Sci & Tec Res 19(2).
- Fujioka K (2019) Characteristic appearances of nodular fasciitis on high-resolution ultrasonography: with vasculature status from a lesion-seated perspective. Biomed J Sci & Tec Res 20(4).
- Fujioka K. Fujioka A, Oishi M, Okada M (2019) A new application in dermatological ultrasound. Biomed J Sci & Tec Res 22(5).
- Fujioka K. Fujioka A, Okada M (2019) Utility of high-resolution ultrasonography by using acoustic coupler in dermatology. Biomed J Sci & Tec Res 23(5).
- Fujioka K, Fujioka A, Okada M (2020) High-resolition ultrasonographic appearances in superficial fibromatoses: palmar and plantar diseases. Biomed J Sci & Tec Res 27(2).
- Malhotra P, Walla H, Singh A, Ramesh V(2010) Leiomyoma cutis: a clinicopathological series of 37 cases. Indian J Dermatol 55: 337-341.
- Chen YA, Chuang WY, Hsuceh S, Chan KC (2012) Solitary nodule on the auricle. Int J Dermatol 51: 1427-1428.
- Kimura R, Sugita K, Goto H, Yamamoto O (2019) A small nodule on the auricle. Clin Exp Dermatol 44: 203-205.
- Smith J, Wisniewski SJ, Lee RA (2006) Sonographic and clinical features of angioleiomyoma presenting as a painful Achilles tendon mass. J Ultrasound Med 25:1365-1368.
- Gormez-dermir V, Gallardo E, Landeras R, Echevarri F, Garcta Barredo R (2006) Subcutaneous angioleiomyoma: gray-scale and color Doppler sonographic appearances. J Clin Ultrasound 34: 50-54.
- Park HJ, Kim SS, Lee SY, Choi YJ, Chung EC, et al. (2012) Sonographic appearances of soft tissue angioleiomyomas: differences from other circumscribed soft tissue hypervascular tumors. J Ultrasound Med 31:1589-1595.
- Zhang JZ, Zhou J, Zhang ZC(2016) Subcutaneous angioleiomyoma: clinical and sonographic features with histopathologic correlation. J Ultrasound Med 35:1669-1673.
- Catalano O, Roldan FA, Solivetti FM, Scotto di Santolo M, Bouer M, et al. (2017) Color Doppler sonography of extradigital glomus tumors. J Ultrasound Med 36:231-238.
- Gupte C, Butt SH, Tirabosco R, Saifuddin A (2008) Angioleiomyoma: magnetic resonance imaging features in ten cases. Skeletal Radiol 37: 1003-1009.
- Yoo HJ, Choi JA, Chung JH, Oh JH, Lee GK, et al. (2009) Angioleiomyoma in soft tissue of extremities: MRI findings. AJR 192: W291-W294.
- Hwang JW, Ahn JM, Kang HS, Suh JS, Kim SM, et al. (1998) Vascular leioma of an extremity: MR imaging-pathology correlation. AJR Am J Retogenal 171: 981-985.
- Kumar S, Hasan R, Maddukuri SB, Mathew M (2014) Angioleiomyoma presenting as a painful subcutaneous mass: a diagnostic challenge. BMJ Case Rep 2014.bcr2014206606.
- Maurya V, Ravikumar R, Sarkar K, Ranjan R (2019) Imaging in a rare case of intramuscular angioleiomyoma around the knee joint Indian J Radiol Imaging 29: 438-441.
- Jin W, Kim GY, Park SY, Chun YS, Nam DH, et al. (2010) The spectrum of vascularized superficial soft-tissue tumors on sonography with a histopathologic correlation: part 1, benign tumors. AJR 195: 439-445.
- Reynolds DL, Jackson JA, Inampudi P, Jamadar DA, Ebrahim FS, et al.(2004) Sonographic characteristics of peripheral nerve sheath tumors. AJR Am J Roentgenol 182: 741-744.
- Lee SK, Kim JY, Jeong HS (2020) Benign peripheral nerve sheath tumor of digit versus major-nerve: comparison of MRI findings. Plos One: 15(3): e0230816.
- Wang C, Song R, Kuang PD, Wang LH, Zhang MM (2017) Giant cell tumor of the tendon sheath: magnetic resonance imaging findings in 38 patients. Oncology Letters 13: 4459-4462.
