 Research Article
Research ArticleAbstract
Objective: To evaluate the control of bleeding with the use of tranexamic acid (ATX), administering a single dose of venous tranexamic acid 20mg per kg of weight after anesthetic induction in patients undergoing primary total knee arthroplasty.
Methods: This prospective cohort study evaluated 40 patients with tricompartmental gonarthrosis from December 2018 to December 2019. Of these only 20 used ATX and were included in these group. The others are related in the control group. Inclusion criteria were idiopathic gonarthrosis, age between 53 and 65 years, aligned lower limb axis, body mass index less than 35 kg / m2 and joint stability. In order to characterize the aligned lower limb, the pre-operative radiological angle measurement was used, considering the aligned limb measured between 7° of varus to 7° of knee valgus. Exclusion criteria were non-idiopathic gonarthrosis, age less than 53 years and over 65, lower limb deformity, body mass index greater than 35kg / m2 and joint instability. We compared the mean per operative and post-operative bleeding of both group sand evaluated the effectiveness of ATX in reducing bleeding. Perioperative control was accounted for through the aspirator collectors during the surgery and the bleeding absorbed by the surgical compresses. Postoperative control was assessed by suction drainage debit in the first 48 postoperative hours. We also evaluated the need for blood transfusion between the groups.
Results: The variables investigated in the study: Weight of Dirty Compresses, Collec to rand Pre Bleeding, Post Bleeding and Total Bleeding presented statistically significant values, at the 5% significance level they rejected the hypothesis that the Control and Test groups had the same bleeding. With this we can say that at a level of 5% of significance the drug Transamin has effect in reducing the variables that represent the bleeding of patients, except the variable Quantity of Dirty Compresses.
Conclusion: The use of intravenous ATX was effective in reducing bleeding in patients undergoing primary total knee arthroplasty.
Keywords: Tranexamic Acid; Primary Total Knee Arthroplasty; Bleeding
Abbreviations: ATX: Tranexamic Acid; TKA: Total Knee Arthroplasty; T-PA: Tissue Plasminogen Activator
Introduction
Total knee arthroplasty (TKA) has been more prevalent due to the increase in life expectancy and is already one of the most common elective procedures performed in the United States. Considering TKA to be a major surgery and predicting blood loss, the need for blood transfusion becomes a reality in some settings. Both allogeneic transfusion and blood loss can potentially result in substantial increases in costs and significant complications such as postoperative infection, delayed physical recovery, increased hospital stay and increased mortality [1]. Peroperative blood loss can vary from 300ml to 2000ml in primary TKA procedures [2,3]. These complications may be more evident in patients with pre-existing medical comorbidities, including degree of deformity, heart, lung, kidney disease and surgical time [4,5].
Although there is a very large number of rigorous tests, blood transfusion causes significant inherent risks including hemolytic reactions, inflammatory tissue damage, infection, among other blood-borne diseases, as well as the immune modulation caused by allogeneic transfusion, contamination and immunological reactions [6,7]. In view of the higher financial cost and these possible complications and adverse events associated with blood loss and blood transfusion, it is necessary to investigate and discover strategies to reduce bleeding in TKA. ATX is an antifibrinolytic, inhibits the dissolution of clots by blocking the formation of plasma by not activating the coagulation cascade, reducing the intensity and risks of bleeding [8-10]. The objective of this study was to evaluate the influence of ATX in reducing bleeding in primary knee total arthroplasty surgeries and to evaluate the decrease in the need for blood transfusion.
Methods
It is a prospective cohort where 40 patients were evaluated, from December 2018 to December 2019, with gonartrosetri compartmental. The work was approved by the Research Ethics Committee of the Center for Biological and Health Sciences at the Federal University of the State of Rio de Janeiro (UNIRIO). CAAE 80969517.0.0000.5258. Inclusion criteria were idiopathic gonarthrosis, age between 53 to 65 years, aligned lower limb axis and body mass index less than 35 kg / m2 and joint stability. The exclusion criteria were non-idiopathic gonarthrosis, age less than 53 years and more than 65, deformity of the lower limb and body mass index greater than 35kg /m2 and joint instability. To characterize the aligned lower limb, we used the measurement of the preoperative radiological angle, considering the limb aligned between 7° of Varus and 7° of valgus of the knee. The perioperative bleeding estimated in the study was that counted in the surgical site aspirators during the surgery plus the bleeding absorbed by the surgical compresses.
Postoperative bleeding was also considered and estimated by the flow of vacuum drains installed during the first 48 hours after surgery. Only one team participated in the surgery of the selected patients. The surgical technique involved a cutaneous incision in the knee midline, followed by soft tissue dissection and sub vastus medial patellar arthrotomy, known as Southern, with joint debridement, soft tissue balance followed by femoral, tibial and patellar cuts. Hemostasis care was observed. No pneumatic tourniquet was used. Vacuum suction drains were positioned to allow adequate drainage of the surgical wound in the postoperative period for 48 hours. Tranexamic acid was used in each patient after anesthetic induction, intravenously, in a single dose (20 mg per kg of weight). Patients who met the selection criteria were divided into two groups. In group A (test), with 20 patients, 20 mg per kg of weight, intravenous, of ATX was administered after anesthetic induction. In group B (control), with 20 patients, ATX was not administered.
The patients involved in the study remained hospitalized for 48 hours postoperatively, in order to identify possible complications related to the use of the drug, especially those resulting from thromboembolic events, such as venous thrombosis, pulmonary embolism, arterial occlusions, renal failure, etc. After this period, we started periodic outpatient monitoring. The results were expressed as means. For comparisons, Student’s t-test or Mann-Whitney test was used, when appropriate. The statistically significant results were accepted with p <0.05. To verify homogeneity in the researched samples, the Shapiro-Wilk test was performed.
Results
The variables investigated in this study were: surgery side, age, number of dirty compresses, weight of dirty compresses (in grams), preoperative collector (in ml), blood in the compress (in ml), preoperative bleeding (in ml) , postoperative bleeding (in ml) and total bleeding (in ml).
Exploratory Analysis (Tables 1-3)
Based on the data above, the distributions of the variables were similar. Viewing this same data in the form of boxplots, in Figure 1, both sides had a similar distribution of bleeding, generating an indication that there is no difference in bleeding between the operated sides excluding the use of the medicine (Figure 1). We observed that the test group on both sides operated on had less bleeding than the control group (Figure 2).
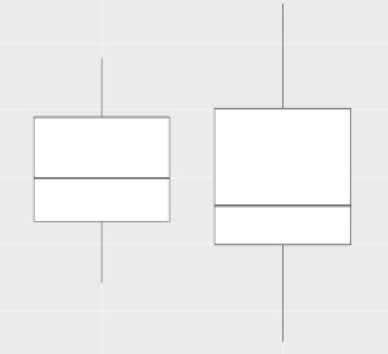
Figure 1: Total bleeding per operated side.
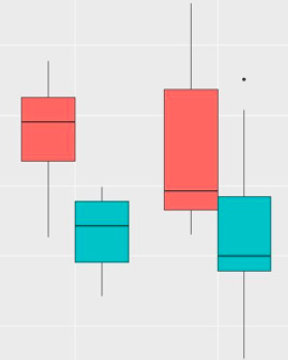
Figure 2: Total bleeding per side Operated according to treatment groups.
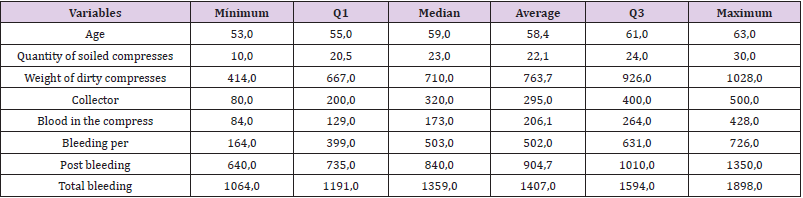
Table 1: Summary measures of control group variables.
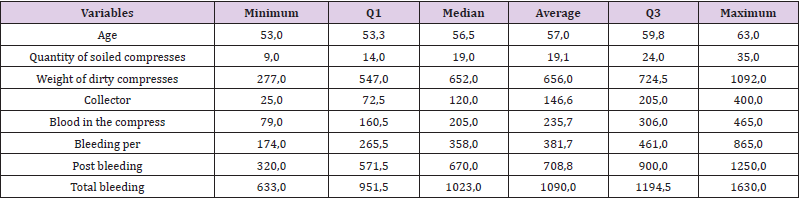
Table 2: Summary measures of the variables in the Test group.

Table 3: Summary measures of Total Bleeding per operated side.
For the age analysis, we created the Age Range variable from the median age. We obtained a median of 59 and two new options for a new variable created: “Age group from 59 years old” and “Age group below 59 years”. Analogously to the analysis of the operated sides, we observed that the Age Group variable has differences in distributions between the Age Group classes (Table 4) and (Figure 3). The older group had greater total bleeding than the younger group (Figure 3 & Table 5).
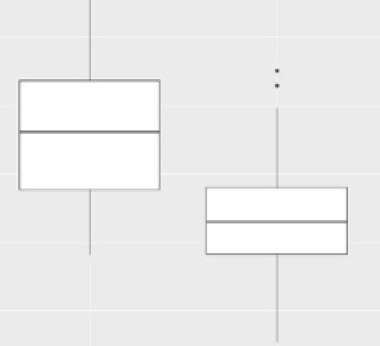
Figure 3: Total Bleeding by Age Group

Table 4: Summary measures of the variable Total Bleeding according to Age category.

Table 5: Summary measures of the Total bleeding variable by age group according to treatment group.
We found that again the groups in which the drug was tested were those that obtained lower medians compared to their peers in the Control Group (Figure 4).

Figure 4: Boxplots of the Total bleeding variable by Age according to treatment group.
Evaluating only the differences in the total bleeding variable between treatments, that is, between the Control group and the Test group, the Test group had a lower amount of total bleeding when compared to the Control group. Table 6 shows the summary measures of these two groups (Table 6). The Figure 5 representing the measures in Table 6.
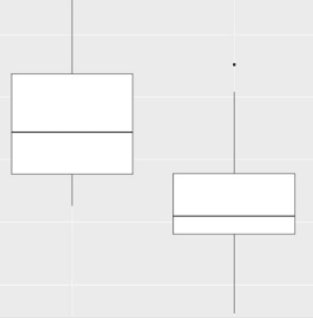
Figure 5: Total Bleeding by Treatment used.

Table 6: Summary measures of Total Bleeding per treatment.
Statistical Tests
Table 7: Student’s T test result for comparisons of means of the response variables of the Control group versus Test group (Table 7).
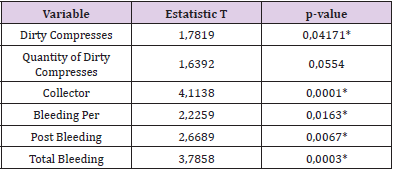
Table 7: T-statistic and P-value of Student’s T test according to variables.
*statistically significant value at the 5% level.
We note that the variables Weight of Dirty Compresses, Collector and Per Bleeding, Post Bleeding and Total Bleeding showed statistically significant values, that is, at the 5% level of significance, they rejected the hypothesis that the means of the Control and Test groups were the same. With this we can affirm that at the level of 5% of significance, the drug Transamin had an effect in reducing the variables that represented the bleeding of the patients with the exception of the variable Quantity of Dirty Compresses. The Blood Bag variable, which represented the amount of blood transfused to the patient, had an expected response, where a patient who loses more blood needs more transfusion, increasing the average amount of blood received. In the database, the Control group presented 5 patients who used a blood bag obtaining an average of Total Bleeding of 1753.4 ml and needing an average of 1.6 blood bags. In the Test group only one patient who had 1491ml Total Bleeding needed a blood bag.
Discussion
Approximately 450 thousand total knee arthroplasties are performed annually in the United States [11]. Each year we will have an increase in the number of TKA due to improvements in techniques, good results and increased life expectancy [12]. An estimate made by Kurtz et al. [13] shows a substantial increase in the number of TKA performed annually in the United States, approximately 670% increase in the year 2030. This gives us an approximate total of 3.5 million knee arthroplasties that same year. Other important data are the large blood loss from the TKA procedure [2,3] and the high rate of blood transfusion resulting from this loss [14]. Based on these data, we were able to predict the size of the economic impact arising from hospital costs. Considering that in the United States the average cost of a red blood cell concentrate is approximately 158 times greater than just one ampoule of tranexamic acid [14,15], the positive effect in reducing bleeding in a TKA using ATX would bring considerable savings to the system of health. With surgical trauma, an activation of the fibrinolytic system occurs at the expense of the release of tissue plasminogen activator (T-PA).
The main enzyme that acts in the conversion of plasminogen to plasmin is T-PA. In association, thrombin is also responsible for releasing T-PA in the vascular endothelium, activating fibrinolysis [16]. During surgery there is an increase in fibrinolysis due to greater release of plasmin at the site of vascular damage, caused by surgical stress. Resulting in increased blood loss. Based on this knowledge, the use of tranexamic acid (synthetic inhibitor of fibrinolysis) acts by making a competitive inhibition of plasminogen activation receptors in plasmin [17,18], and due to the non-formation of plasmin, we achieve a delay in fibrinolysis which results in a clot stabilization [19]. The choice of this drug for the study was based on its safety profile and on its effectiveness reported in the literature. Even after several authors have studied the effect of using tranexamic acid in order to reduce bleeding and the need for transfusion of blood products in primary TKA, we still have disagreements regarding the dose and ideal time for the administration of the drug in studies [20,21].
In the present study, we observed that there was no difference in bleeding when comparing the operated side. Our results showed that the group that used ATX had a lower mean of perioperative bleeding. Other studies have analyzed this relationship and obtained similar results [22,23]. No complications related to the use of the drug were observed. The Blood Bag variable was proportional to the patient who lost more blood. Analyzing the Age Group variable that was created from the median of ages, we observed that the older group had greater total bleeding than the younger group, but this finding will not be explored by this study. The variables Weight of Dirty Compresses, Collector and Pre Bleeding, Post Bleeding and Total Bleeding showed statistically significant values and with this we can say that the drug Transamin had an effect in reducing the variables that represented the bleeding of patients with the exception of the variable Quantity of Dirty Compresses.
Conclusion
We concluded that intravenous ATX applied at a dose of 20mg / kg after anesthetic induction was effective in satisfactorily reducing blood losses resulting from TKA surgery, which consequently resulted in a reduction in the need for blood transfusion.
References
- Spahn DR (2010) Anemia andpatientblood management in hip andkneesurgery: A systematic review of the literature. Anesthesiology 113(2): 482-495.
- Barsoum WK, Klika AK, Murray TG, Higuera C, Lee HH, et al. (2011) Prospectiv erandomized evaluation of the need for blood transfusion during primary total hip arthroplasty with use of a bipolar sealer. J Bone Joint Surg Am 93(6): 513-518.
- Seo JG, Moon YW, Park SH, Kim SM, Ko KR (2013) The comparative efficacies of intra articular and IV tran examic acid for reducing blood loss during total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 21(8): 1869-1874.
- Cushner FD, Friedman RJ (1991) Blood loss in total knee arthoplasty. Clin Orthop Relat Res (269): 98-101.
- Orpen NM, Little C, Walker G, Crawfurd EJP, et al. (2006) Tranexamic acid reduces early post-operative blood loss after total knee arthoplastiy: a prospective randomised controlled trial of 29 patients. The Knee 13(2): 106-110.
- Kirkley SA, Cowles J, Pellegrini VD, Harris CM, Boyd AD, et al. (1998) Blood transfusion and total joint replacement surgery: T helper 2 (TH2) cytokine secretion and clinical outcome. Transfus Med 8(3): 195-204.
- Klein HG (2010) How safe is blood, really? Biologicals 38(1): 100-104.
- Hynes M, Calder P, Scott G (2003) The use of tranexamic acid to reduce blood loss during total knee arthoplasty. The knee 10(3): 375-377.
- Kagoma YK, Crowther MA, Douketis J, Bhandari M, Eikelboom J, et al. (2009) Use of antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic surgery: a systematic review of randomized trials. Thromb Res 123(5): 687-696.
- Gandhi R, Evans HMK, Mahomed SR, Mahomed N (2013) Tranexamic acid and reduction of blood loss in total knee and hip arthroplasty: a meta-analysis. BMC Research Notes 6: 184.
- Rockville (2009) Healthcare Cost and Utilization Project (HCUP). HCUP Facts and Figures: Statistics on Hospital-Based Care in the United States, 2007 [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US).
- Ritter MA (2009) The anatomical graduated component total knee replacement: along-term evaluation with 20-year survival analysis. J Bone Joint Surg Br 91(6): 745-749.
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M (2007) Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 89(4): 780-785.
- Wong J, Abrishami A, El Beheiry H, Mahomed NN, Roderick Davey J, et al. (2010) Topical application of tranexamic acid reduces postoperative blood loss in total knee arthroplasty: a randomized, controlled trial. J Bone Joint Surg Am 92(15): 2503-2513.
- Shander A, Hofmann A, Ozawa S, Theusinger OM, Gombotz H, et al. (2010) Activity-based costs of blood transfusions in surgical patients at four hospitals. Transfusion 50(4): 753-765.
- Jansen AJ, Andreica S, Claeys M, D'Haese J, Camu F, et al. (1999) Use of tranexamic acid for an effective blood conservation strategy after total knee arthroplasty.Br J Anaesth 83(4): 596-601.
- Mac Gillivray RG, Tarabichi SB, Hawari MF, Raoof NT (2011) Tranexamic acid to reduce blood loss after bilateral total knee arthroplasty: a prospective, randomized double blind study. J Arth 26(1): 24-28.
- Mc Connel JS, Shewale S, Munro NA, Shah K, Deakin AH, et al.(2012) Reducing blood loss in primary knee arthroplasty: a prospective randomised controlled trial of tranexamic acid and fibrin spray. The Knee 19(4): 295-298.
- Hynes M, Calder P, Scott G (2003) The use of tranexamic acid to reduce blood loss during total knee arthroplasty. The Knee 10(4): 375-377.
- Charoencholvanich K, Siriwattanasakul P (2011) Tranexamic acid reduces blood loss and blood transfusion after TKA: a prospective randomized controlled trial. Clin Orthop Relat Res 469(10): 2874-2880.
- Gandhi R, Evans HMK, Mahomed SR, Mahomed NN (2013) Tranexamic acid and the reduction of blood loss in total knee and hip arthroplasty: a meta-analysis. BMC Research Notes 6: 184.
- Almeida MDC, Albuquerque RP, Palhares GM, Almeida JPC, Barreto JM, et al. (2018) Evaluation of the use of tranexamic acid in total knee arthroplasty. Res Bras Ortop 53(6): 761-767.
- Volquid D, Zardo RA, Winkler BC, Londero BB, Zanelatto N, et al. (2016) Use of tranexamic acid in primary total knee arthroplasty: repercussions on perioperative blood loss. Rev Bras Anestesiol 66(3): 254-258.
