 Case Report
Case ReportSummary
Exogenous lipoid pneumonia is an uncommon disease that occurs by the accidental ingestion of lipid material. The radiological manifestations tend to be heterogeneous and must correlate with the amount and characteristics of the aspirated material. The diagnosis is established by histopathology.
Clinical Case: We report the radiological characteristics of an infant female patient of one year of age with severe exogenous lipoid pneumonia secondary to oil aspiration.
Conclusions: The radiological manifestations include ground-glass pattern, consolidation regions with air bronchogram predominantly toward the bases, and posterior segments. The thoracic x-ray and CT scan may fundament the suspected diagnosis in some pediatric centers that do not have a bronchoscopy and can be a prognostic factor in seriously ill patients.
Keywords: Oil; Lipoid Pneumonia; Bronchoalveolar Lavage; Cat; Interstitium; Ground- Glass
Introduction
Accidental inhalation or aspiration of mineral, vegetable, or animal oil is the most common form of exogenous lipoid pneumonia that represents a severe accident in the pediatric patient [1,2]. Exogenous lipoid pneumonia is caused by lipid accumulation inside alveolar macrophages that causes alveolar occupation, interstitial and proliferative inflammation of the pulmonary parenchyma [3]. Patients may present respiratory distress data in a sudden manner according to the quantity, type of intake and duration of the aspirated material in the alveoli, and/or respiratory failure and death [4,5]. The radiological manifestations are unspecific, however the computer axial tomography (CAT) is a useful and specific tool while not the diagnosis, if it is to see the damage to the lung parenchyma [7,8]. The diagnosis is based on performing a bronchoscopy with bronchoalveolar lavage and reporting lipidloaded macrophages [9,10].
Clinical Case
This report presents the case of a female infant patient of one year and one month of age with a history of gastroesophageal reflux, treated with prokinetic from birth until six months of age, who referred seven days prior to her admission a picture of upper respiratory infection after having swallowed accidentally, and in the presence of an older sister, ten milliliters of a handmade product referred to as oil for body massage. At the time of the intake, the patient experienced choking and vomiting of gastric contents. She also presented dry cough, nausea, and respiratory distress data characterized by intercostal and sternal retractions and increased work of breathing, which is why she was taken to be assessed at the urgent care of a second-level hospital. Here, the patient remained only under observation in urgent care and was discharged without treatment. The patient persisted with respiratory symptoms, and was transferred 24 hours later to a private children’s hospital to complete treatment. In the emergency room at 75% ambient saturation, irritable, pale, with severe breathing difficulty data characterized by nasal flaring, intercostal retractions, and thoracoabdominal dissociation. The posteroanterior and lateral thoracic x-ray at admission (Figure 1). It was decided to perform an endoscopy of the airways for suspected bronchoaspiration, observing granular oropharyngeal mucosa, trachea with hyaline mucus secretion, and mucosal edema. A bronchial aspiration was performed (Figure 2). Treatment was started with antibiotics, systemic steroids, nebulizations with a bronchodilator, inhaled steroid, and oxygen therapy.
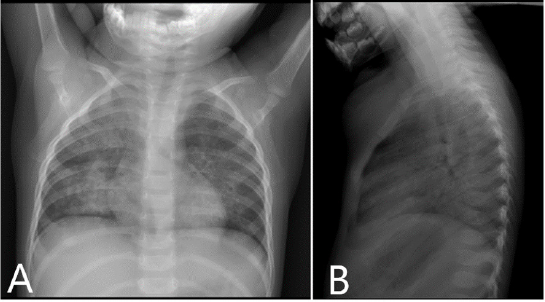
Figure 1:
(A) Posteroanterior and
(B) lateral thoracic x-ray.
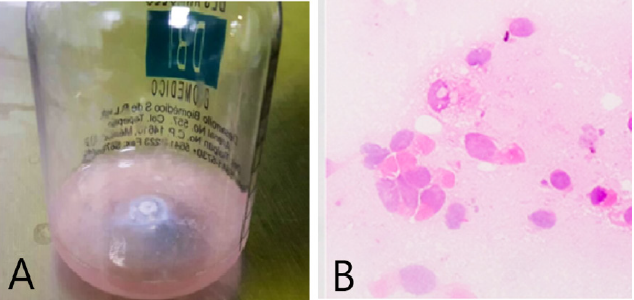
Figure 2: Bronchial aspiration.
(A) It shows an opalescent appearance with a halo of supernatant fat.
(B) Bronchoalveolar lavage. Lipid-loaded alveolar macrophages are observed.
The patient experienced rapid and progressive evolution of respiratory difficulties, increased work of breathing, episodes of bronchospasm, fever, and elevation of procalcitonin to 6ng/ ml. Within seven days of escalating coverage, a computerized axial tomography was performed, observing severe lung damage (Figures 3-5). Thoracic computed tomography lung window and high-resolution; the ground glass areas are observed towards the anterior segments and the consolidation area towards the posterior segments with air bronchogram suggestive of interstitial occupation. Subsequently, she presented ventilatory and hemodynamic deterioration, so the endoscopic therapeutic procedure was deferred, meriting vasopressor amines, and high ventilatory parameters. Radiology control (Figure 6) was observed. The patient presented progression of the ventilatory impairment due to the severe lung injury with multiple organ failure and death (Figure 7-9).
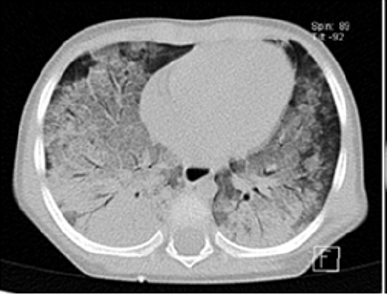
Figure 3: In axial view.

Figure 4: In axial view.

Figure 5: Coronal view.
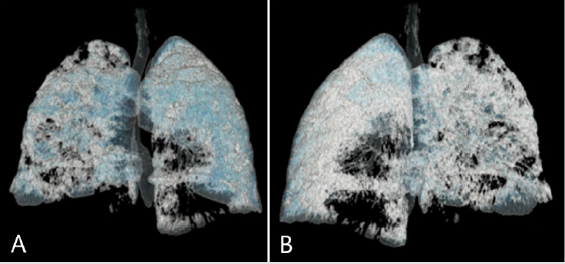
Figure 6: Three-dimensional (3D) thoracic computed tomography reconstruction
(A) Anterior and
(B) Posterior with significant decrease of airspace and lung volume.
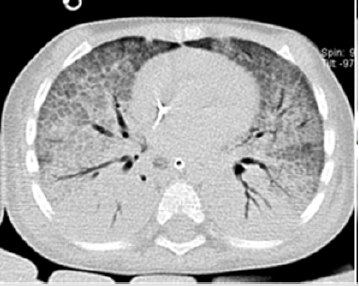
Figure 7: High-resolution thoracic computed tomography lung window in axial and coronal cuts, observing an increase in the extension of the consolidation zones, as well as increase in the extension of the ground glass areas.

Figure 8: High-resolution thoracic computed tomography lung window in axial and coronal cuts, observing an increase in the extension of the consolidation zones, as well as increase in the extension of the ground glass areas.

Figure 9: Three-dimensional (3D) thoracic computed tomography reconstruction, we can observe a significant decrease in air volume in both lungs, compared to previous volumetric reconstruction.
Discussion
Lipoid pneumonia was first described by Laughlen in 1925, when he observed in four autopsies the presence of oil in the lungs [11] Lipoid pneumonia or exogenous pneumonitis is an uncommon disease in pediatrics whose exact incidence is probably underestimated in developing countries [12]. In children, it is usually caused by the accidental ingestion of exogenous lipids that are used in developing countries as part of the treatment for constipation [4,13,14]. In this clinical case, the accidental ingestion was of an oily substance used for tanning. The clinical presentation includes dry or productive cough with increased work of breathing; upon physical examination, patients present bronchoalveolar rales, stridor, wheezing, and clinical data of hypoxia [2,15], as in this clinical case that progressed to ventilatory failure [16]. The radiological and tomographic imaging assessment is critical, especially when a bronchoscopy cannot be performed, as it allows to assess the severity of the lung damage as diagnostic suspicion and substantiate the therapeutic [9] by sending a sample from a bronchoalveolar lavage to pathology to confirm lipid-loaded macrophages [17], which are responsible for the acute inflammatory reaction [18,19] that can progress to fibrosis in the terminal stage of the disease [16,17]. Although it is radiologically indistinguishable from various pathologies with alveolar occupation and ground-glass such as bacterial pneumonia; a common denominator in thorax x -rays are the diffuse ground-glass appearance with alveolar interstitial opacities, presence of air bronchogram with consolidation, nodular lesions, reticular and alveolar interstitial pattern, which are the most common findings in the thoracic x-ray and CAT [6,8,20]. The lower lobes and the right middle lobe are commonly involved, but multifocal and bilateral lesions can also be observed [21-23], as well as bad-defined nodules, pneumatoceles, and pleural effusion [24]. The treatment is based on multiple bronchoalveolar lavages that can eliminate lipid-loaded macrophages as the main cause of fibrosis in the alveoli and the interstitium [9,25], which, in the present clinical case, had to be differed due to the ventilatory and hemodynamic instability. The extracorporeal membrane oxygenation (ECMO) is indicated for respiratory failure but the hospital did not have it available [26].
Conclusion
The radiological imaging has a great impact in the case of lipoid pneumonia as it can establish the severity and condition a prognosis factor of poor evolution for pediatric patients, with the evolution of this case the patient it had to be used ECMO and perform wash bronchial alveolar lavages for decreased the high probability of early death. We currently use ECMO and have used it in patients with severe respiratory failure with excellent results in some patients.
References
- Sachdev anil, Anand Preeti, Gupta d (2015) Lipoid Pneumonia - An Unusual Cause of Acute Respiratory Distress Syndrome 52(1): 63-64.
- Lu G, Xie Y, Huang L, et al. (2016) Study of Acute Exogenous Lipoid Pneumonia. Indian J Pediatr 83(8): 787-791.
- Marchiori E, Zanetti G, Mano CM, Hochhegger B (2011) Exogenous lipoid pneumonia. Clinical and radiological manifestations. Respir Med 105(5): 659-666.
- Hu X, Lee JS, Pianosi PT, Ryu JH (2015) Aspiration-related pulmonary syndromes. Chest 147(3): 815-823.
- Furuya MEY, Moreno Córdova V, Ramírez Figueroa JL, Vargas MH, Ramón García G, et al. (2007) Cutoff value of lipid-laden alveolar macrophages for diagnosing aspiration in infants and children. Pediatr Pulmonol 42(5): 452-457.
- Betancourt SL, Martinez Jimenez S, Rossi SE, Truong MT, Carrillo J, et al. (2010) Lipoid pneumonia: Spectrum of clinical and radiologic manifestations. Am J Roentgenol 194(1): 103-109.
- Garzón Lorenzo P, Torrent Vernetta A, Server Salvà L, De Vicente CM, García Cendón C, et al. (2008) Neumonía lipoidea exó An Pediatr 68(5): 496-498.
- Zanetti G, Marchiori E, Gasparetto TD, Escuissato DL, Soares Souza A (2007) Lipoid pneumonia in children following aspiration of mineral oil used in the treatment of constipation: High-resolution CT findings in 17 patients. Pediatr Radiol 37(11): 1135-1139.
- Dengler NF, Antoniadis G, Grolik B, Wirtz CR, König R, et al. (2017) Mechanisms, Treatment, and Patient Outcome of Iatrogenic Injury to the Brachial Plexus–A Retrospective Single-Center Study. World Neurosurg 107: 868-876.
- Cuevas Schacht F, César Ortega Iglesias J, Ma Cristina Sosa de Martínez D, Claudia Garrido Galindo D, Felipe Pérez Fernández L (2005) Broncoscopia en pacientes pediátricos con atelectasia persistente. Hallazgos endoscópicos y resultados de la aspiración selectiva (1990-1992). Acta Pediátrica México 26(2).
- Laughlen GF (1925) Studies on penumonia following naso-pharyngeal injections of oil. Am J Pathol 1(4): 407-414.
- Annobil' SH, Tahir M El, Kameswaran M, Morad N (1997) Olive oil aspiration pneumonia (lipoid) in children 4: 383-388.
- Tukaram SJ, Sastry SDS, Mehta RM (2018) Bronchoscopic Segmental Lavage for Refractory Lipoid Pneumonia in a Toddler. J Bronchol Interv Pulmonol 25(2): e19-e21.
- Hoffman LR, Yen EH, Kanne JP, Effmann EL, Gibson RL, et al. (2005) Lipoid Pneumonia Due to Mexican Folk Remedies Cultural Barriers to Diagnosis. Arch Pediatr Adolesc Med 159: 1043-1048.
- Marangu D, Gray D, Vanker A, Zampoli M (2019) Exogenous lipoid pneumonia in children: a systematic review. Paediatr Respir Rev 33: 45-51.
- Bush D, Deterding R, Weinman J, Galambos C (2017) Hypoxemia in lipoid pneumonia: Role of intrapulmonary bronchopulmonary anastomoses. Am J Respir Crit Care Med 195(11): 1531-1532.
- Athayde Salgado I, Cavalcante Santos C, Victor Salgado J, Consorte Ferraz P, Maria Haidar D, et al. (2012) Exogenous lipoid pneumonia in children: a disease to be reminded of. Rev Assoc Med Bras 58(2): 135-137.
- Ridaura Sanz C, López Corella E, Salazar Flores M (2006) Exogenous lipoid pneumonia superinfected with acid-fast bacilli in infants: A report of nine cases. Fetal Pediatr Pathol 25(2): 107-117.
- Goussard P, Rabie H, Morrison J, Schubert PT (2019) Superinfection with Mycobacteria goodii in a young infant with exogenous lipoid pneumonia. Pediatr Pulmonol 54(9): 1345-1347.
- García AA, Roberto J, Serratos V, Hinojos LC, González IM (2009) Tres casos de neumonía lipoidea exógena en niños y revisión de la literatura.
- Marangu D, Pillay K, Banderker E, Gray D, Vanker A, et al. (2018) Exogenous lipoid pneumonia: an important cause of interstitial lung disease in infants. Respirol Case Reports 6(7): e00356.
- Harris K, Chalhoub M, Maroun R, Abi Fadel F, Zhao F (2011) Lipoid pneumonia: A challenging diagnosis. Hear Lung J Acute Crit Care 40(6): 580-584.
- Modaresi M, Dadkhah M, Sayedi SJ (2015) Exogenous lipoid pneumonia: Dramatic clinical and radiological improvement after multiple segmental bronchoalveolar lavages. Iran J Pediatr 25(6): e3172.
- Chiang IC, Lin YT, Liu GC, Chiu CC, Tsai MS, et al. (2003) Exogenous lipoid pneumonia: serial chest plain roentgenography and high-resolution computerized tomography findings. Kaohsiung J Med Sci 19(12): 593-598.
- Sias SMA, Daltro PA, Marchiori E, Angela S Ferreira, Regina L Caetano, et al. (2009) Clinic and radiological improvement of lipoid pneumonia with multiple bronchoalveolar lavages. Pediatr Pulmonol.
- Frenckner B (2015) Extracorporeal membrane oxygenation: a breakthrough for respiratory failure. Journal of Internal Medicine 278:586-598.
