 Case Report
Case ReportAbstract
Chryseobacterium indologenes (C.indologenes) presence in soil, water, plants and can be detected in water systems, tap wetter and wet surfaces in the hospital environment because of its vitality in the chlorinated waters. C.indologenes is not involved in the human flora and rarely isolated as infectious agent. A 80 years old female patient, with known hypertension, who applied to hospital with complaint of nausea and vomiting was diagnosed as prerenal acute renal failure according to clinical and laboratory findings (TA: 75/ 50mmHg, urea: 85,06mg/dl, creatinine: 10.4mg/dl, pH: 7.22mmol/L, HC03: 16.3mmol/L, Na: 129mg/dl, K: 4.3mg/dl, Cl 93.1mg/dl,). Hemodialysis catheter was inserted due to hemodialysis requirement. It was seen that following hydration therapy, creatinine levels decreased. On the fifth day of hospitalization, the patient's fever was increased (38.5 °C) and the CRP value was 82.14mg/L. After the blood culture samples were taken, ceftriaxone and clindamycin were used as empirical treatment. The isolate was identified from blood samples as C. indologenes with both conventional methods (Gram strain, oxidase, indole, lactose, citrate, urease) and Microscan (Beckman Coulter, USA) automated system. Antibiotic susceptibilities were determined by both disk diffussion method and Microscan (Beckman Coulter, USA) automated system too. The isolate was found to be susceptible to ciprofloxacin, levofloxacin, piperacillin tazobactam, trimethoprim-sulfamethoxazole and resistant to cefotaxime, gentamicin, amikacin, tobramycin, ceftazidime, aztreonam, imipenem, meropenem, tetracycline, chloramphenicol. On the third day of antibiotic therapy, CRP (21.03 mg/L) started to decrease. During the follow- up, renal function was improved and fever control was provided. The patient was discharged on the 11th day after the treatment with clindamycin and ciprofloxacin. As a result, it should be noted, C.indologenes can be found in the hospital environment, may cause infections with intravenous catheter applications. So avoided unnecessary applications and infection control measures should be taken in this regard.
Keywords: Chryseobacterium Indologenes; Catheter Associated Blood Stream Infection; Hemodialysis Catheter; Hospital Control Measures.
Introduction
Chryseobacterium indologenes (C.indologenes) formerly Flavobacterium indologenes is not generally known as infectious agents and are rarely isolated in human infection [1]. C.indologenes is found primarily in soil and water. The organism can survive in chlorinated water supplies, frequently colonizing taps and be reservoirs for infections in the hospital. Colonization of patients through contaminated medical devices involving solutions such as respirators, intubation tubes, the intravenous catheter [2]. Previous studies have reported that C.indologenes can cause pneumonia, sepsis, and tracheobronchitis. C.indologenes is the primarily opportunistic pathogen in newborns and immunocompromised patients [3-6]. This report presents the case of a non-immunosuppressive patient developed C. indologenes related catheter-associated bloodstream infection, following acute renal failure treatment.
Case Presentation
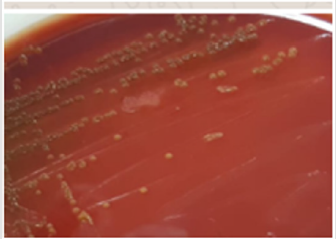
Figure 1: A typical yellow-pigmented C. indologenes colony in blood agar medium.
An 80 years old female patient, with known hypertension, admitted to hospital with the complaint of nausea and vomiting was diagnosed as prerenal acute renal failure. It is detected that pulse rate was 88/min, the temperature was 36.8 °C, and blood pressure was 75/ 50mmHg. The laboratory data were urea: 85,06mg/dl, creatinine: 10.4mg/dl, pH: 7.22mmol/L, HCO3: 16.3mmol/L, Na: 129mg/dl, K: 4.3mg/dl, Cl 93.1mg/dl. Hemodialysis catheter was inserted due to hemodialysis requirement. Following hydration therapy, creatinine levels decreased. On the fifth day of hospitalization, the patient's temperature was increased 38.5 °C and the C-reactive protein (CRP) value was 82.14mg/L. Two sets of blood culture samples were sent to the Microbiology Laboratory for investigation. After the blood culture samples were taken, ceftriaxone and clindamycin were used as empirical treatment. Cultures were processed with the BacT/ALERT System (BioMerieux, Marcy l'Etoile, France). Bacterial growth was revealed within 48 to 72 hours. Specimens were cultured in 5% Sheep blood agar (HiMedia, India), Eosin Methylene Blue agar (HiMedia, India) and Chocolate agar (HiMedia, India) and incubated at 37 °C for 24 hours. After incubation, yellow-pigmented colonies were observed in the blood agar (Figure 1). Oxidase and indole tests were positive and lactose, citrate and urease tests were negative. In addition, the Microscan Walkaway Plus (Beckman Coulter, USA) automated system was used to identify the microorganism. C. indologenes was identified as the causative agent. According to the minimum inhibitory concentration (MIC) values, C. indologenes was found to be susceptible to ciprofloxacin (0.25mg/μl), levofloxacin (≤ 0,5mg/μl), piperacillin/tazobactam (≤8mg/μl) and trimethoprim-sulfamethoxazole (≤ 1/19 mg/ μl), while it was shown to be resistant to, gentamicin (>8mg μl), amikacin (32mg/μl), tobramycin (>8mg μl), cefotaxime (> 16mg/μl), ceftazidime (> 16mg/μl), aztreonam (> 16mg/μl), imipenem (>8mg μl), meropenem (>8 mg μl) [7]. On the third day of antibiotic therapy, CRP (21.03mg / lt) started to decrease. During the treatment, renal function was improved and fever control was provided. After the patient was treated with clindamycin and ciprofloxacin over eleven days, clinical improvement of the bloodstream infection was observed. The patient was discharged on the 11th day after the treatment.
Discussion
Opportunistic infections due to this organism, often arising from colonization of indwelling mechanical devices [8]. C. indologenes is of low pathogenicity. The production of biofilm on foreign materials may play an important role in the virulence of invasive infections caused by C. İndologenes [9,10]. Risc factors of C. indologenes were hospitalization, malignity and especially immunosuppression [1,3]. C. indologenes reported related tracheobronchitis in transplante patient who take anti-tuberculosis treatment for six months [4]. Ceylan, et al. [3] observed a case of fatal C. indologenes septicemia developed in a newborn with hydrocephalus. Christakis et al. [11] indicated non-catheter-related bacteremia caused by C. indologenes in a patient with a solid tumor. They highlihted, although the majority of C. indologenes infections are linked to the use of indwelling devices. In the literature, C. indologenes appears to cause infection in immunosuppressed patients [3,4,11]. However, it has been reported that it may be an infectious agent in immunocompetent individuals. McKewa, et al. [5] reported case of severe sepsis from a 53 year old man with no underlying medical conditions was admitted with the septic shock one week after returning from hiking. They indicated the organism has the potential to be highly pathogenic. In this report, C. indologenes infection occurred due to intravenous catheter use during the treatment of acute renal failure in an immunocompetent patient in hospital.
Antimicrobial susceptibility data of C. indologenes is limited since this pathogen has been barely isolated from clinical specimens. The SENTRY Antimicrobial Surveillance Program conducted by using results from North America, Latin America, Europe, and the Asia-Pacific region detected that the most active agents against C. indologenes are the quinolones and trimethoprim-sulfamethoxazole, followed by piperacillin-tazobactam. In addition, aminoglycosides, chloramphenicol, linezolid, and glycopeptides are not appropriate for treating infections due to this organism [12]. Also, C. indologenes strains are the natural reservoir of chromosomally linked metallo-β-lactamases [13]. In this report in accordance with previous studies quinolones, piperacillin tazobactam and trimethoprim-sulfamethoxazole seem the most susceptible antibiotics to C. indologenes infection. And the isolate was resistant to carbapenems. In conclusion, C. indologenes can cause infection not only in immunosuppressive patients but also in immunocompetent individuals. It should be noted, C.indologenes can be found in the hospital environment, may cause infections with intravenous catheter applications. So avoided unnecessary invasive applications and infection control measures should be taken in this regard.
Conflicts of Interest
The authors have no conflicts or interests to declare.
References
- Yasmin S, Garcia G, Sylvester T, Sunenshine R (2013) Chryseobacterium indologenes in a woman with metastatic breast cancer in the United States of America: a case report. Journal of Med Case Rep 7: 190.
- du Moulin GC (1979) Airway colonization by Flavobacterium in an intensive care unit. J Clin Microbiol 10(2): 155-160.
- Ceylan A, Guducuoglu H, Akbayram S, Bektas A, Berktas M (2011) Sepsis caused by Chryseobacterium indologenes in a patient with hydrocephalus. Microbiol Bul 45: 735-740.
- Caliskan E, Kilic N, Alasan F, Kilincel O, Sahin I, et al. (2016) A Case of Tracheobronchitis Caused by Chryseobacterium indologenes in an Immunosuppressed Patient. Anatol Clin J Medi Sci 21(2): 139-142.
- McKewa G (2014) Severe Sepsis Due to Chryseobacterium indologenes in an Immunocompetent Adventure Traveler J Clin Microbiol 52(11): 4100-4101.
- Imataki O, Uemura M (2016) Chryseobacterium indologenes, a possible emergent organism resistant to carbapenem antimicrobials after stem cell transplantation Clin Case Rep 5(1): 22-25.
- (2013) CLSI. Performance standards for antimicrobial susceptibility testing; Twenty-third informational supplement. CLSI document M100-S23. Wayne, PA: Clinical and Laboratory Standards Institute.
- Stamm WE, Colella JJ, Anderson RL, Dixon RE (1975) Indwelling arterial catheters as a source of nosocomial bacteremia. An outbreak caused by Flavobacterium species. N Engl J Med 292(21): 1099-1102.
- Hsueh PR, Teng LJ, Ho SW, Hsieh WC, Luh KT (1996) Clinical and microbiological characteristics of Flavobacterium indologenes infections associated with indwelling devices. J Clin Microbiol 34(8): 1908-1913.
- Pan HJ, Teng LJ, Chen YC, Hsueh PR, Yang PC, et al. (2000) High protease activity of Chryseobacterium indologenes isolates associated with invasive infection. J Microbiol Immun Infect 33(4): 223-226.
- Christakis GB, Perlorentzou SP, Chalkiopoulou I, Athanasiou A, Legakis NJ (2005) Chryseobacterium indologenes non-catheter-related bacteremia in a patient with a solid tumor. J Clin Microbiol 43(4): 2021-2023.
- Kirby JT, Sader HS, Walsh TR, Jones RN (2004) Antimicrobial susceptibility and epidemiology of a worldwide collection of Chryseobacterium spp: report from the SENTRY Antimicrobial Surveillance Program (1997-2001) J Clin Microbiol 42(1): 445-448.
- Bellais S, Poirel L, Leotard S, Naas T, Nordmann P (2000) Genetic diversity of carbapenem-hydrolyzing metallo-beta-lactamases from Chryseobacterium (Flavobacterium) indologenes. Antimicrob Agents Chemother 44(11): 3028-3034.
