 Research Article
Research ArticleAbstract
Objective: Describe the characteristics of lower limb atherosclerosis in diabetic patients on MSCT angiography.
Methods: 45 patients with diabetes mellitus aged 49 to 91 (mean 72.2), including 31 male and 14 females, with stenotic lower extremity symptoms according to Leriche and Fontaine classification. MDCT angiography was performed for all patients.
Result: 890 arterial segments of 3 stages studies. Arterial occlusions at the infrapopliteal, femoral-poplitealand iliac level were 30.1%, 9.8% and 7.2% respectively. Arterial calcifications presenting 60,2%, most multiple segments (65,9%). More than one stage of stenosis ≥ 50% was 73,7%, which the most common infrapopliteal stage (50.6%). Severestenosis>70%, collateral circulation at the iliac, femoral and infrapopliteal levels were 75%, 70.6% and 37.5% respectively.
Conclusion: Stenosis of lower extremity atherosclerosis in diabetes are diffuse multi-stage, multi-location and common infra-popliteal stage. In severe stenosis cases, collateral circulation was less common on infra-popliteal level.
Keywords:Diabetes mellitus; Lower extremity Atherosclerosis; Multidetector CT Angiography
Introduction
Diabetes mellitus (diabetes) tends to increase markedly with the development of economic and social life. In 2000, there were 171 million people in the world with diabetes and this number was estimated to be 366 million in 2030 [1]. Atherosclerosis is both a combined disease and a cause of serious diabetes complications. In which damage to the arteries of the lower limb is a silent complication but it greatly affects the quality of life, causes disability and can increase mortality. Doppler ultrasound is still the first method used to investigate lesions of the lower limb arteries, but in diabetic subjects with calcification, sclerosis of the arterial walls will cause more or less restriction for the process. examination. MSCT has angioplasty correcting the disadvantages of ultrasound and giving a more general picture of the lower limb arteries lesions.Therefore, this study is conducted with the aim of describing images of coronary artery disease in diabetic patients on MSCT with angiogram.
Materials and Methods
The study was conducted at radiology department, Bach Mai hospital, including 45 patients with type II diabetes, including 13 patients who reviewed the medical records from January 2014 to September 2014 and had 32 patients were studied from October 2014 to July 2015. Patients were 49 to 91 years old (average of 72 years), including 31 men and 14 women. All patients had symptoms of coronary artery stenosis and were clinically classified according to Leriche and Fontaine. Cross-sectional descriptive study design. Choose a purposeful sample, convenient sample size. Using the Siemens Somatom Sensation 64 and 256 Multi- Slice CT. Pre-injection evaluation calcification. After injection, use Xenetic Contrast (300mg / ml) to inject intravenous machine, total dose of 100ml, speed of 3ml / s. Using techniques to regenerate arteries in 3-dimensional space (MPR, MIP, VR, CPR). The lower limb arteries on each side are divided into 3 levels, including 10 segments: pelvic floor (2 segments): general pelvic artery, external pelvic artery; femoral thigh (4 segments): general femoral artery, shallow femoral artery, deep femoral artery; lower layer of knee (4 segments): body of a lateral lobe, anterior anterior lobe, posterior anterior lobe, anterior lateral lobe. Of the 45 patients, two patients had amputation on one side of the limb from a limp, so the total number of study segments was 890.
Study variables: Vascular stenosis, calculated automatically by software and according to NASCET, has 5 levels: nonsterosis, mild stenosis <50%, moderate stenosis 50-70%, severe stenosis 70-99% and completely sterosis. Calcification lesions, there are 3 levels: no calcification (<50HU), mild calcification (<50%) and severe (accounting for> 50% of the circumference of the vascular wall). Number of lesions per segment: 1 site and more than 1 site. Assess the collateral circulation (upper left arm) in the narrow layer> 70% heavy: good case height (with 3 or more branches of upper arm with diameter> 1mm); Poor collateral circulation (many bladder branches but any branch has diameter ≤ 1mm or maximum of 2 branches with diameter> 1mm). Data processing using SPSS 20.0 software.
Result
Most patients showed signs of severe anemia, with stages III and IV, accounting for 82.2% (37/45). 30 patients showed symptoms of toe necrosis. Among the conditions associated with diabetes, hypertension accounting for 82.2% (37/45 patients). The proportion of patients with coronary and cerebrovascular disease associated with coronary artery disease was 17.8% (8/45) and 22.2% (10/45, respectively).The percentage of patients with MSCT lesions at a slight stenosis degree accounted for the highest proportion (35.6%). The proportion of patients with significant hemodynamic significance (stenosis> 70%) accounted for 38.0%, of which occlusion was 17.3% of the total number of patients. 30.1% of patients showed embolism in the infra-popliteal stage, this rate in the iliac stagewas 7.2% and in the femoral-popliteal stage was 9.8% (Table 1). Nearly two-thirds of the segments have calcification of the wall (60.2%), severe calcification (calcification accounts for more than 50% of the circumference of the vessel) is 24.4%. Calcification is most common in the iliac stage (85%), followed by the femoral-popliteal (65.4%), the infra-popliteal stageaccounting for 42.3% (Table 2) (Figure 1).
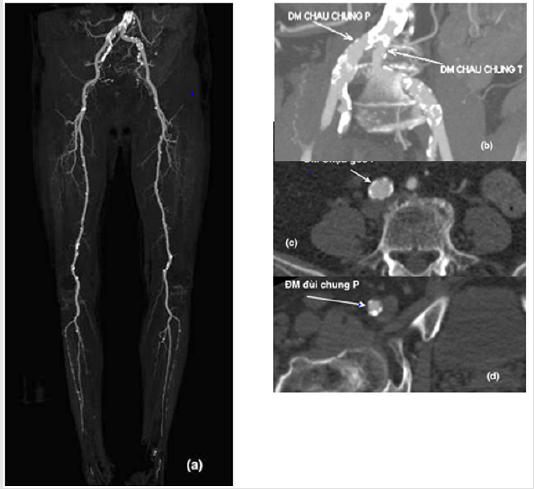
Figure 1: MSCT of patient, 85 years old, 18 years diabetes.
a) Calcification lesions spread to 3 arterial stages of lower limb.
b) Severe calcification of the right iliac artery.
c) Severe calcification of the right iliac artery.
d) Right femoral artery.

Table 1: The rate of vascular obstruction is narrowed according to the anatomical stage on MSCT.

Table 2: The rate of calcification of the arterial wall by anatomical stage on MSCT.
The calcification lesions of the lower limb artery in patients with diabetes had a high rate, mainly the diffuse lesions in all 3 stages (58/88) limb lesions in all 3 stages) accounted for 65.9% (Table 3).Of the 338 segments with a stenosis of more than 50%, 249 of them were lesions with more than one site or whole segment, accounting for 73.7% and 71.9%, respectively. In which the infra-popliteal stageis often the most damaged position (50.6%) (Table 4). There is no low risk and low risk in the group with poor collateral circulation, we found that: In the arterial or narrowed artery segment ≥ 70%, the occurrence of collateral circulation mainly in the iliac stageand femoral-popliteal stage with high rate (75.0% and 70.6%). The infra-popliteal stage appears poorer (48/128 cases of severe stenosis) (Table 5).

Table 3: The ratio of floors with calcified arterial wall on MSCT.

Table 4: The number of stenosis sites ≥ 50% on a vascular segment according to the anatomical stage.

Table 5: Collateral circulation in Completely stenosis and narrow lesions ≥ 70%.
Note: Non – collateral circulation; +: Little collateral circulation; ++: Good collateral circulation
Discussion
The further outward, the proportion of the arterial lesions in severity level will increase. 30.1% of patients showed completely stenosis in the infra-popliteal stage, this rate in the iliac stage was 7.2% and the femoral-popliteal stage was 9.8%. This is also consistent with the lower limb artery disease in diabetic patients who often suffer more damage in the infra-popliteal stage [2]. R.Schernthaner et al researched on 50 patients with the lower limb artery disease with 1351 vascular segments, there were 353 stenosis segments ≥70% (accounting for 26.1%), 161 segments infra-popliteal stage [3]. XiangJiang Guo et al studied 162 diabetic patients on 3 anatomical stages and found that 660 vascular lesions were found, of which 223 were severe stenosis (accounting for 33.8%) [4,5].
Rahul J. Shiro, et al. [6] studied the role of MSCT in assessing the lower limb artery lesions and found that 43/60 cases (71.7%) encountered calcification on MSCT. Swain Jayshree et al studied calcification lesions in both anterior and posterior tibial arteries in 74 patients with diabetic foot ulcer found this rate was 42% [7]. The reason our results are higher than this group is because the total number of segments we studied is more.We evaluate imaging of the collateral circulation on MSCT in the segment of lesions with severe stenosis ≥ 70% and completely stenosis. The criteria for assessing the quality of the collateral circulation are applied according to the author Omran Khodary Qenawy, et al. [8], there are 3 levels: non - collateral circulation (grade 0), little collateral circulation (grade 1) good collateral circulation (grade 2). The results show that the collateral circulation occurs in the iliac stage and femoralpopliteal stage, while the infra-popliteal stage appears poor. This is easy to explain because the iliac stage and femoral-popliteal stage have many lateral branches, good collateral circulation and large diameter of the lateral branches. In contrast to the infrapopliteal stage with small diameter. Especially, diabetic patients often hurt small arteries, so the collateral circulation is as poor as the periphery [9]. The research of Aoife N Keeling et al also noted a relationship between the number and diameter of the collateral circulation branch with the stage of disease, the ABI index, the thickness of atheroma, the average diameter of the main artery ..., especially the number of the collateral circulation branches in the group of the lower limb artery disease due to hypertension is more 2 times higher than the cause of diabetes [10].
Conclusion
Our study of lower limb atherosclerosis on MSCT in 45 diabetic patients with a total of 890 arteries, we found that: Arterial stenosis has many multi-stages, multiple-position and common features in the infra-popliteal stage (occlusion accounts for 30.1%). Arterial calcification is a common lesion in diabetic patients (60.2%). Collateral cirrculation is usually in severe stenosis> 70%, but the infra-popliteal stage is the poorest.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest to this study.
References
- Leoniuk J, Lukasiewicz A, Szorc M, F Izabela Sackiewicz, Jacek Janica, et al. (2014) Doppler ultrasound detection of preclinical changes in foot arteries in early stage of type 2 diabetes. Pol J Radiol 79: 283-289.
- Xiang Jiang Guo, Ya Xue Shi, Xiao Zhong, Meng Ye, Guan Hua Xue, et al. (2013) Features analysis of lower extremity arterial lesions in 162 diabetes patients. Journal of Diabetes Research.
- Schernthaner R, Stadler A, Lomoschitz F, Weber M, Fleischmann D, et al. (2008) Multidetector CT angiography in the assessment of peripheral arterial occlusive disease: Accuracy in detecting the severity, number, and length of stenoses. Eur Radiol 18(4): 665-671.
- XiangJiang Guo, YaXue Shi, XiaoZhong, Meng Ye, GuanHua Xue, et al. (2013) Features analysis of lower extremity arterial lesions in 162 diabetes patients. Journal of Diabetes Research.
- Tran Van Luong (2013) Features of 64 sequences of CLVT images and evaluation of the early results of treatment of chronic lower limb anemia by intravascular intervention, Graduation thesis of resident physician, Hanoi Medical University.
- Rahul J Shirol, Aathish Shetty, Chethan TK (2015) Role of MDCT in Evaluation of Peripheral Vascular Disease of the Lower Limb Arteries and Comparison with Colour Doppler", Journal of Evolution of Medical and Dental Sciences 4(54): 9336-9346.
- Swain Jayshree, Tiwari Shalbha, Pratyush DD, Awanindra Dwivedi, Balram Gupta, et al. (2012) Vascular calcification in diabetic foot and its association with calcium homeostasis. Indian Journal of Endocrinology and Metabolism 16(8): 450-452.
- Omran Khodary Qenawy, Wahid Hussein Tantawy, Abdel Karem Hasan Abdalla, Samy Abdel Aziz Sayeda (2015) Comparative study between multi-detector CT angiography and digital subtraction angiography in evaluation of peripheral arterial occlusive disease. The Egyptian Journal of Radiology and Nuclear Medicine: 1-8.
- Sharad Pendsey, Marvin ELevin (2014) Evaluation of neuroischemic foot. Contemporary Management of the Diabetic Foot: 111-118.
- Keeling AN, Carroll TJ, McDermott MM, Liu K, Liao Y, et al. (2012) Clinical correlates of size and number of collateral vessels in peripheral artery disease. Vasc Med 17(4): 223-230.
