 Case Report
Case ReportAbstract
Since December 2019 the world has been experiencing a state of alert due to a novel virus, now known as SARS-CoV2. In recent days the World Health Organization (WHO) has declared it officially a pandemic. As far as the date of this article is sent, we do not have any other report in Mexico of Coronavirus diseases 2019 (COVID-19) with severe pneumonia. We report the case of a 68-year-old male with comorbidities and the course of action taken and also the clinical behavior during his hospital stay.
Abbreviations: WHO: World Health Organization; MERS-CoV: Middle East respiratory coronavirus; SARS-CoV: Severe Acute Respiratory Syndrome Coronavirus; ICU: Intensive Care Unit; CT: Computed Tomography; RT-PCR: Reverse Transcription Polymerase Chain Reaction; ER: Emergency Room
Introduction
Since December 2019 the world has been experiencing a
state of alert due to a novel virus, now known as SARS-CoV-2. In
recent days the WHO has declared it officially a pandemic. The
coronaviruses are classified within Nidovirales order, the viruses
that affect humans are: alpha coronaviruses (HCoV-229E and
HCoV-NL63) and beta coronaviruses (HCoV-HKU1, HCoV-OC43,
Middle East respiratory coronavirus (MERS-CoV) and severe
acute respiratory syndrome coronavirus (SARS-CoV) [1]. The new
coronavirus reported is the seventh strain to cause respiratory
disease in humans, this virus falls into the genus beta coronaviruses
[2]. According to Guan Z et al. in the recent article of clinical
characteristics of coronavirus disease [3]. They had studied a total
of 1099 patients with confirmed COVID-19. They measured three
endpoints: admission to intensive care unit, the use of mechanical
ventilation, or death. They reported that from the 1099 patients
the median age was 47 years, the proposed endpoint occurred in
67 patients (6.1%), 5.0% were admitted to the Intensive Care Unit
(ICU), 2.3% required invasive mechanical ventilation and 1.4%
died.
The frequency of symptoms were reported as follow: fever
43.8% on admission and 88.7% during hospitalization, cough
67.8%. It is reported a median incubation period of 4 days in this
study, but this information is slightly different than the one reported
by Li Q [4] in which the median of symptoms is 5.2 days with the
95th percentile of the distribution at 12.5 days. Regarding radiologic
findings the most common image in computed tomography (CT)
scan is ground-glass opacities in up to 56.4% on admission, it is
important to mention that in patients with severe disease a total
of 2.9% of the patients didn’t have any radiological findings in
the CT scan [3]. In the laboratory tests in another series of cases published by Chen N et al. it is mentioned that out of 140 patients,
61 patients (44%) had lymphopenia, 58 (41%) had elevation of
hepatic transaminases, procalcitonin levels were normal in almost
all patients except those with secondary infection [5].
The diagnosis in Mexico is made according to international standards similar to the ones reported by Ying-Hui J et al. At this moment the first approach is to assess if the patient is within the standard definition of suspicious case; which recalls for anyone who has been in contact with a confirmed COVID-19 infected patient or someone who has traveled to any of the high incidence countries. Then ask about the symptoms being of high suspicion the ones who report fever, dry cough or shortness of breath. The first step is to take a rapid flu test, if this one is negative we proceed to order reverse transcription polymerase chain reaction (RT-PCR) of respiratory pathogens, if this second test proves to be negative, we request the sanitary jurisdiction to take a respiratory swab for COVID-19 testing. The test is done also by RT PCR for COVID-19 with an estimated time for response of approximately 12 to 24 hours.
Case report
We present the case of a 68-year-old male that was admitted
at the emergency room (ER) of the San Angel Inn Universidad
Hospital in Mexico City, last March 11th, 2020; due to presenting
disorientation and delusion ideas.
The patient presents the following relevant background:
a) Intense tobacco use suspended 30 years ago.
b) Intense alcohol use suspended 5 years ago.
c) Chronic ischemic cardiopathy, 7 years ago, the patient
presented acute coronary syndrome requiring the placement of
a stent currently with double platelet antiaggregation.
d) Diabetes mellitus type 2 currently treated with metformin.
e) Systemic arterial hypertension, treated with olemsartan/
hydrochlorothiazide
f) Previous to his admission, the patient visited the following
tourist destinations:
i) February 24th, 2020 - 7 day stayed in Madrid.
ii) March 1st, 2020 - 2 day stayed in Mexico.
iii) March 3rd, 2020 - 7 day stayed in Cuba.
Condition started 5 days prior to his admission by presenting
asthenia and adynamia accompanied by hyporexia; and subsequently
presenting fever 38.3°C (100.9°F) and incoherent speech. Due to
the persistence of the symptomatology, his companion decided to bring him to the ER. During the led interrogatory, patient reported
presenting the last days before his admission, dry cough, and mild
dyspnea. During the initial physical examination, the patient’s vital
sings with blood pressure 120/77mmHg, heartbeat rate 124 beats
per minute respiratory rate 32 breaths per minute temperature
37.8°C (100.0°F) peripheral oxygen saturation 79% without
supplementary oxygen, no alteration in consciousness state, lung
examination with disseminated crackles. During initial approach,
patient is identified with radiographic data from an unenhanced
chest computed tomography with multiple consolidative peripheral
opacities with ground-glass density in multiple lobes (Figures
1-6) with a peripheral distribution, which has been reported as a
common finding of SARS-CoV-2 pneumonia [6].
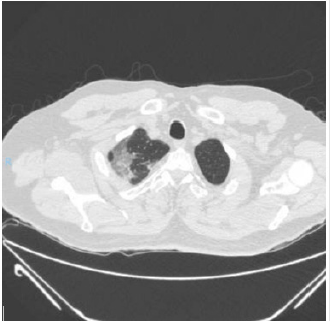
Figure 1.
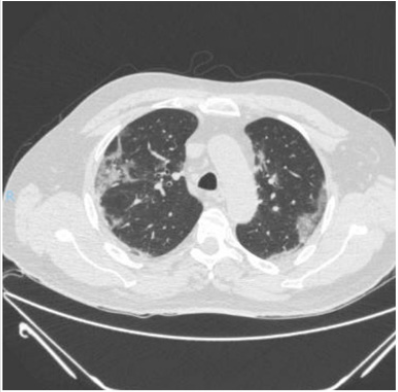
Figure 2.
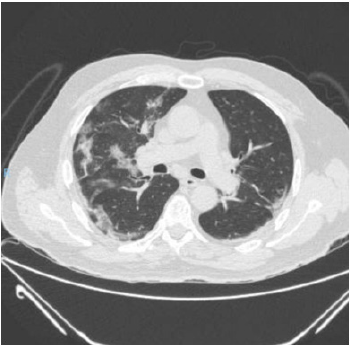
Figure 3.

Figure 4.

Figure 5.

Figure 6.

Table 1: Laboratories at admission.
Once identified the risk factors and suspicious for a COVID-19 case the patient was isolated according to hospital policies. RTPCR samples were taken for respiratory virus and then notified to the epidemiology department. Empirical treatment was initiated in cooperation with infectious diseases department for atypical pneumonia and possible COVID-19 with supplementary oxygen, bronchodilators (ipratropium, fluticasone and olodaterol/ tiotropium), ceftaroline, clarithromycin and oseltamivir. The day after, the INDRE (Instituto de Diagnóstico y Referencia Epidemiólogica) notified that the patient´s nasopharyngeal swap was positive for SARS-CoV-2, therefore we withdraw oseltamivir and instead hydroxychloroquine 400mg po bid the first day and continue 200mg po bid and lopinavir 400mg/ritonavir 100mg po bid were started. Laboratory findings on admission showed leukocytes of 9.27 x 103/μL, neutrophilia 8.15 x 103 /μL, total lymphocytes of 0.464 x 103/ μL, Lactic dehydrogenase 311 U/L, TGO 190 U/L, TGP 160 U/L (Table 1).
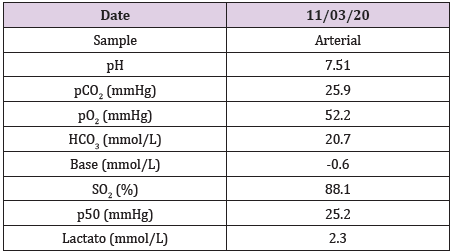
Table 2: Blood Gas.
Arterial blood gases moderate hypoxemia (pAO2= 52.2mmHg), acute hypoventilation (pACO2 25.9mmHg), pH 7.51, values adjusted to Mexico City height. PaO2/FiO2 249 mmHg (mild ARDS). At admission, the following severity scales were estimated: CURB65 (2) mortality of 9.2%, PSI (128) Class IV; 9.3% mortality, SMARTCOP (5) high risk of admission to the Intensive Care Unit (ICU). We would like to remind that the SMART-COP score reflects better the clinical condition of the patient. During hospitalization the respiratory treatment consisted in high flow nasal cannula witch gradually was stepped down to conventional nasal cannula 6 days after, as the patient remains stable without inflammatory systemic response or clinical data of respiratory distress we decided to discharge the patient with no need of supplementary oxygen. On a subsequent follow up he referred clinically stable without signs of active COVID-19 disease (Tables 2 & 3).
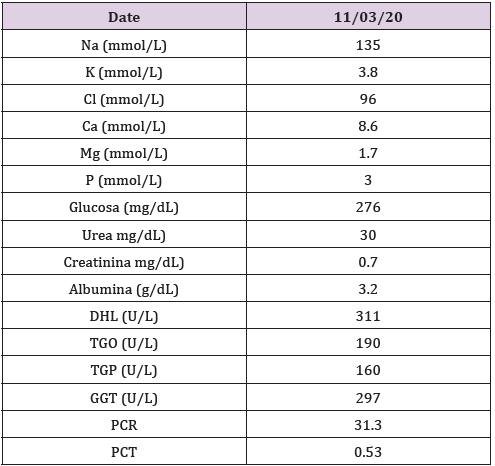
Table 3: Blood Chemistry.
References
- Chan JF, Lau SK, To KK, Cheng VCC, Woo PCY, et al. (2015) Middle East respiratory syndrome coronavirus: another zoonotic betacoronavirus causing SARS-like disease. Clin Microbiol Rev 28(2): 465-522.
- Zhu Na, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China 2019. N Engl J Med 382(8): 727-733.
- Guan W, Ni Z, Hu Y, Liang W, Ou C, et al. (2020) Clinical Characteristics of coronavirus disease2019 inchina. N Eng J Med 382:1708-1720.
- Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med382:1199-1207.
- Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395: 507-513.
- YingHui J, Lin C, ZhenShun C, Hong C, Tong Deng, et al. (2020) A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus(2019 nCoV) infected pneumonia (standard version). Military Medical Research 7(1):4.
